
You are currently browsing the category archive for the ‘technology’ category.
Spend enough time trawling through social media posts with a #DOC somewhere in the hashtag, and it is inevitable that you will see photos of people’s CGM graphs. Often, it’s PWD getting excited at their flat line graphs because they have managed to stay within range for a certain period of time. Or perhaps it’s to show shock and utter disbelief at loop systems doing all the work. It can be because we won’t to show how we have managed to nail the timing and amount of a bolus, and that usually-difficult to manage food nemesis (hello, rice!), completely avoiding a spike. Or, it could be just because we feel like sharing.
I don’t share my graphs a heap these days, but have in the past. It’s a personal decision as to whether we want to share their data online, and if you do, knock yourself out. Your data, your rules! I understand why some feel that it can be considered not especially helpful for others, setting us up to feel we are failing if we compare. But the conversation sharing can generate is really useful for a lot of people.
Every now and then, a non-PWD will share their libre or CGM trace to show that even those with a perfectly working pancreases are subject to glucose fluctuations. This is done with the intention of support and encouragement and to show that flat lines really are unrealistic. While I’m sure that those sharing glucose graphs of people without diabetes is never done with any malice – in fact, completely the opposite – I believe it is nonetheless problematic, and misses the point.
I get it. It’s a noble goal to try to make PWD feel less negative when we are unable to manage a perfectly flat line at 4.0mmol/l for hours on end. And to also understand that’s not how the body actually works, even when everything is doing what it should be doing.
But it is totally redundant. And downright annoying. And also, completely inconsiderate.
I live with diabetes and am fixated on trying to limit the variation of my glucose levels because I have to. PWD are told that keeping those numbers between 4mmol/l and 8 mmol/l is the goal. And we’re told that when we go outside of those numbers – especially when we go beyond the upper limit, all manner of nasty things will happen to us. That’s what was told to me the day I was diagnosed with diabetes, and repeatedly what I have seen since.
Showing me your graph that just happens without any effort on your part is not reassuring. It’s pointless. And somewhat heartless. When your level goes up to 12 because you ate a family block of chocolate, it comes back in-range fairly quickly. And not because you had to do any fancy-pants calculations, or micro (or rage) boluses.
When I eat a block of chocolate, whatever happens next is pretty much 100% due to my efforts. I have done some fancy pants calculations. I have had to bolus – maybe once, most likely a number of times – to get my glucose level back in range. And then I sit there and hope that I haven’t over bolused…
Oh – and when you show me that your glucose levels dipped into the low range or sat there for a while, it doesn’t reassure me or make me feel ‘normal’. Because the difference is that when that happens to me, I am doing all I can to make sure that I am okay, that I don’t pass out, that I don’t overtreat (again!), and that I am safe. And then I get to recover from a hypo hangover – something you are fortunate to never experience.
To be honest, I actually find it completely ironic when it is HCPs sharing their data to make me feel better, and a little thoughtless because the reason that I am in constant pursuit of these straight, tightly-in range lines is because it is HCPs that told me in the first place that is where I must stay to ‘prevent’ all.the.nasty.things.
And finally, when this happens, it centres people without diabetes in a conversation that should very much have the spotlight firmly shone on us. Your glucose level data, and the patterns they make are not like ours. They do not represent the blood, sweat and tears, the emotional turmoil, the frustration, the fear that that is somehow reflected in our data.
Perhaps rather than sharing non-PWD data, instead acknowledge just how difficult it is to do diabetes, and commend people with diabetes for showing up, day after day, to do the best we can – regardless the shape of our CGM graph.
A real-life PWD CGM graph. Mine, from about 10 minutes ago.
Sometimes it feels as though discussions in the diabetes are seasonal. Like clockwork, we see the same conversations happen at the same times. Without missing a beat, almost as soon as a scientific conference is over, someone will comment about how difficult it is for PWD to get to conferences (true, however this year, #dedoc° voices could have assisted a number of the people who were stating that), and then there are discussions about disclosure by PWD who are fortunate to attend, even though pretty much every advocate I know who attends these sorts of things does a stellar job of disclosing.
And of course, the nature of the first big meeting of the year, ATTD, means that there inevitably will be noise about the gap in technology access. And you bet this is a discussion that we need to be having on regular rotation.
After attending my first ATTD, I wrote a piece about the complete and utter dichotomy of being at a conference that was only talking about the latest and greatest in technology while, at the same time, whilst the community was in the midst of its usual Spare a Rose month of fundraising. I struggled to balance the idea that we were talking about automated insulin delivery at the same time as urging donations so people could just get insulin!
Today, I’m revisiting the piece I wrote after last year’s ATTD, where my worlds of diabetes technology and language matters merged, and combined this with the over-representation of those at the super-dooper-tech-y end of the diabetes technology spectrum. (‘Super-dooper-tech-y’ is, obviously, a very technical term.)
I don’t for a moment think that meetings with a strong tech focus should end, or that those who are innovators in technologies should take a seat and let others speak. I don’t believe that at all. I will be forever grateful to the pioneers who continue to push the envelope and make things better for people with diabetes. But I do think that we need to ensure that there is equal attention to those who – by choice or because of their circumstances – are not walking around with an algorithm driving their diabetes.
If we truly believe that all diabetes stories matter, then we need to hear from people doing diabetes in every way possible. Perhaps if we make more of an effort to find and hear those stories, we will stop minimising our experiences, and starr seeing that whatever we are managing to do is truly enough…
DISCLOSURE 1 (for ATTD 2020)
I was an invited speaker at #ATTD2020, and my registration was covered by the conference organising committee. My airfare and part of my accommodation to attend ATTD was covered by Lilly Diabetes so that I could participate in the DOCLab advisory group meeting which took place on Friday, Saturday and Sunday. Other accommodation was covered by DedocLabs (I am an advisor for the #dedoc° voices program) and Novo Nordisk (I am a member of DEEP). I have not been asked to write or speak about any of the activities I attended, or anything I have seen at the conference.
We all do a good job at undermining ourselves at times. We use a four letter word that diminishes what we are doing, and limits the value of our experience and expertise. That four letter word is ‘just’.
In diabetes, we hear it all the time: ‘Oh, I just have type 2 diabetes’ as though it is insignificant and doesn’t have any challenges. ‘I’ve lived with diabetes for just a couple of years’ because we think there is only currency in decades of living with the condition, when really any length of time with diabetes is meaningful.
And we are all about minimising our experience when it comes to the treatment of our diabetes. ‘I just use diet and exercise to manage my type 2 diabetes’ or ‘I’m just on tablets’ or ‘I’m just on injections twice a day’ or ‘I’m just on MDI’. The list goes on and on. And on.
I realised just how ridiculous we have become with this when I heard myself, during a conversation with a fellow Looper, ‘Oh, I just use Loop’. (More on that later…)
At the Ascensia Social Media Summit at ATTD we spoke about this, specifically how there is almost a stigma within the diabetes for those seen to not be using the shiniest and brightest and newest of technologies. It seems that some people almost feel embarrassed if they are not constantly updating their technology toolkit with the most recently launched product.
The idea that anything that we are using today is ‘yesterday’s technology’ is wrong. Blood glucose monitoring can’t be ‘yesterday’s tech’ if it is what most people are using to track their glucose. And syringes and pens can’t be considered the ‘old way to deliver insulin’ when that is how the vast, vast majority of inulin-requiring people with diabetes get insulin into their bodies. Plus, every single one of us using a pump must be able to deliver insulin this way because machines break.
Somewhere in discussions about our treatment technologies, we seem to have forgotten that, actually, not everyone wants to be using the latest kit. And that is okay. There is a spectrum of diabetes technology, and as long as we are on it somewhere and managing our diabetes the way that works best for us, then elephant stamps all around!
There is clearly an over-representation of people at one end of that spectrum dominating on and off line conversations. Spend a couple of hours in a diabetes Facebook group and it would be a reasonable assumption that most people are wearing pumps and CGM. But that’s not true.
And it could appear that DIYAPS is the way to go for most people with T1D, when the fact is that numbers are relatively low. It’s hard to estimate exactly, but there may be somewhere between 2,000 and 3,000 worldwide how have ‘built their own pancreas’. That is just a drop in the type 1 diabetes ocean.
It’s fantastic for those of us interested in this technology to be able to (virtually) congregate and talk amongst ourselves. I learn so much from my peers in these groups – just as I have with all aspects of life with diabetes. The lived experience continues to trump any other way of learning about diabetes.
Of course, that doesn’t mean that we shouldn’t be talking about technology used by limited numbers. Of course we should. We want others to know about it so they can make an informed choice about whether it may be right for them. We want our HCPs to know about it and to support those of us using all sorts of technologies and treatments.
Where it becomes problematic is when there is the misconception that this is the norm. Or when those not using the newest technology feel that they are wilfully doing diabetes the ‘old way’. It’s unfair to think for a moment that those who are not using the tech ‘don’t care’ enough about themselves – especially when decisions are made based on a very good understanding of what is available and what they have decided works best for them.
So, back to my ‘Oh, I just use Loop’ comment. It was directed to someone far more technologically advanced than me; someone who runs all sorts of other programs alongside their DIYAPS. They generate lots of reports and make lots of changes and seem to have far more bells and whistles than I even knew were available.
I nodded as they told me all they were doing and then, when they asked me how I manage my diabetes, I answered that I just use Loop. I heard myself saying it and stopped and corrected myself. ‘I mean…I use Loop. It works for me. Perfectly.’
We don’t need to make excuses for doing diabetes our own way. If we truly have choice (which I know is not always the case), and we have made the choice based on what we believe to be the best possible treatment and technology for us at that moment, then surely that’s a great thing. We shouldn’t ever be made to feel less committed to our own health and wellbeing. That’s not how it works.
DISLCOSURE 2 (for ATTD 2019)
I was invited by Ascensia to co-chair the Diabetes Social Media Summit at ATTD (#ATTDDSMS). I did not receive any payment or in-kind support from them for accepting their invitation. I have co-written a piece for the blog, however this was not edited (apart from inevitable jet-lag-induced typos) and all words are those of mine and the piece’s co-author. You can read that piece here.
These days, I usually don’t show my glucose data online. When I first started Looping (about two and a half years ago), I regularly posted the flat CGM lines that amazed and surprised me. I also shared the not-flat lines that showed how hard my Loop app was working as temp basal rates changed almost every five minutes. The technology worked hard so I didn’t need to, and the results were astonishing to me. I shared them with disbelief. (And gratitude.)
I stopped doing that for a number of reasons. It did get boring, and I definitely recognise my privilege when I say that. I also acknowledge my privilege at being able to access the devices required for the technology to work. And there was the consideration that sharing these sorts of stats and data online inevitably lead to comparisons and competition. That was never my intention, but I certainly didn’t want to add to someone having a crappy diabetes day while I blabbed about how easy my day had been.
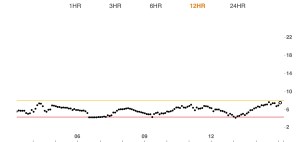
But today, I’m sharing this:

This was my previous 30-day time in range data from the Dexcom Clarity app on the day I arrived back home in Australia after returning from New York. (My range is set to 3.9mmol/l – 8.1mmol/l.) I’m not sharing it to show off or to boast. I don’t want congratulations or high fives. In fact, if anyone was to see this and pat me on the back, I would respond with the words: ‘I had very little do with it’.
I can’t really take credit for these numbers and would feel a fraud if anyone thought I worked hard to make this happen. Using an automated insulin delivery system full time means that I do so much less diabetes than ever before while yielding time-in-range data that I could once only dream of.
I want to share it, not to focus on the numbers (because it’s NEVER about the numbers!), but to explain what happens when diabetes tools get better and better, and what that means in reality to me.
Those thirty days included the following: End of year break up parties for work and other projects (four of those); ‘We-must-catch-up-before-the-end-of-the-year’ drinks with friends (dozens of those!); actual Xmas family celebrations (three of those over a day and a half– and I’m from an Italian family, so just think of the quantities of food consumed there). Oh, and then there were the three weeks away in NY with my family. Our holiday consisted of long-haul flights from Australia, frightful jet lag (there and back), a lot of food and drink indulgences, out-of-whack schedules, late nights, gallons of coffee, no routine, and more doughnuts than I should admit to consuming.
Add to that some diabetes bloopers of epic proportion that had the potential to completely and utterly railroad any best laid plans: insulin going bad, blocked infusion sets, sensors not lasting the distance, a Dex transmitter disaster.
And yet, despite all of that, my diabetes remained firmly in the background, chugging away, bothering me very little, with the end result being time in range of over eighty per cent.
This graph is only part of the story of why I so appreciate the technology that allowed me to have a carefree and relaxed month. Diabetes intruded so little into our holiday. I bolused from my iPhone or Apple watch, so diabetes devices were rarely even seen. Alarms were few and far between and easily silenced. I was rugged up in the NY cold, so no one even commented on the Dex on my upper arm. The few times I went low, a slug of juice or a few fruit pastilles were all it took, rather than needing to sit out for minutes or hours. Diabetes didn’t make me feel tired or overwhelmed, and my family didn’t need to adapt and adjust to accommodate it.
That time-in-range graph may be the physical evidence that can point to just how my diabetes behaved, but there is a lot more to it, namely, the lack of diabetes I needed to do!
As I spoke about this with Aaron, he reminded me of my well-worn comments about not waiting around for a diabetes cure. ‘You’ve always said that although you would love a cure, it’s the idea that diabetes is easier to manage that excites you. Ten years ago, when you spoke about what that looked like, you used to talk about diabetes intruding less and being less of a burden to your day. That is what you have now. And it is incredible.’
In a couple of weeks, the diabetes conference juggernaut will descend on Madrid for ATTD.
This one is all about new treatments and technologies in the world of diabetes and, in its thirteenth year, looks to once again be a busy and enlightening meeting.
There is so much on the program that focuses on user-led technologies and initiatives. I think it’s fair to say that PWD have long recognised that technology in diabetes is more than just the devices we wear on our bodies. We have long used technology for support and to connect to others who help us manage the day-to-day life of diabetes, and to learn and share. DIYAPS may be about the systems, but grasping the role of online platforms and support is essential in understanding the #WeAreNotWaiting movement as a whole.
 It’s great that a number of PWD already know that they will be part of ATTD this year, attending satellite events run by different device and drug companies. Some are on the program and some will be there through other opportunities and work.
It’s great that a number of PWD already know that they will be part of ATTD this year, attending satellite events run by different device and drug companies. Some are on the program and some will be there through other opportunities and work.
The more the merrier, I say! Different voices with different experiences sharing and learning is always a great thing. And having the opportunity to meet people in real life after only seeing them online adds another dimension to our peer support networks.
For European diabetes friends yet to secure a place at ATTD, there is another possible avenue in, but you need to be quick. Launching at ATTD is the new #dedoc° voices program. Although #dedoc°has its foundations in Germany it is truly an international community, involving people from all over the world. #docday° events (always a highlight at these conferences) involve diabetes advocates from across Europe and the US, and even the odd Australian, too. It’s great to see this new initiative is helping more advocates get a seat at the diabetes conference table as active participants.
APPLY NOW
If you want to be considered for the #dedoc° voices program, you need apply, which is super simple – just go here, where you will find out all about the program and how to throw your name in the ring! Applications close on Friday, so chop chop!
Successful applicants will have their travel and accommodation costs reimbursed, and will receive full registration to the conference.
Good luck. And hope you see you there.
Disclosure
I am an advisor to the #dedoc° voices program. I do not receive any payment for this role.
I am an invited speaker at ATTD 2020. Lilly Diabetes is covering my travel and part of my accommodation so I can participate in the DOCLab advisory group meeting held during ATTD.
Busan is a very different city today than it was last week. There won’t be warmly dressed people hurrying into BEXCO with IDF2019 lanyards around their necks, eager to learn about diabetes. The word ‘diabetes’ won’t be uttered in almost every language of the globe. There won’t be Melbourne diabetes people loudly lamenting that Starbucks seems to be the coffee of choice in the city.
And you won’t see groups of people from all around the world standing together talking about what it’s like to live with diabetes. Most of us have gone home to our respective corners of the world, back to our families, back to our jobs, back to our real lives. But we will always have Busan and the incredible week of the IDF Congress.
By the time I arrived in Busan on Monday, the IDF was already a different beast. There was a new President and Board in place and some of the concerns that we’d had about the handover had melted away to nothing. This paved the way for what we really there for: a week of learning, networking, hearing different perspectives and truly uniting for diabetes.
We did that.
Was it a perfect conference? Of course not; they never are. There were hiccoughs and AV fun. There were controversies that played out online very differently to the way they actually happened in real life. There were sessions – critically important and brilliant sessions from all streams– with disappointing turnouts.
But these are all minor concerns that are the reality of every conference I have ever attended. There will be a time for post-mortems and evaluations and planning for improvements to future conferences. That time, however, is not now. Now is the time to celebrate.
IDF 2019 was a brilliant showcase of diabetes from around the globe. As expected, I only attended sessions from the Living with Diabetes stream and every single story was beautifully presented, and enhanced by the professional expertise of the HCPs who shared the stage. Amongst the incredible tales were moments of discomfort. It’s challenging to hear of the struggles many of my sisters and brothers with diabetes face in their day to day lives. I was forced to confront my privilege in a way that demands more than just acknowledging it there.
Also, difficult to accept is realising that sometimes the chasm between what people living with diabetes want and need and what HCPs and researchers think we want is gulf-like. For every HCP who ‘gets us’ and understands the value of lived experience in the healthcare space dialogue, there are many others who just don’t accept it, and, despairingly, don’t want to listen.
But more on that another day. Because for now, I’m focused on the people who did such a stellar job. So here are just some of them!

Two hours after touching down in Busan, and we kicked off the sixth Ascensia Social Media Summit with these gems.

Bright and early on day 1 of IDF2019, and the auditorium was packed to hear about diabetes and tech.

Always, ALWAYS, pleased to share the stage with Jane. Here we are just before the panel session.

Georgie excited to TALK ABOUT HYPOS! (We couldn’t understand why there was an explanation mark at the end of that sentence.)

Manny Hernandez gave the LWD Stream Award Lecture and there is no one more qualified to talk about the importance of diabetes community. How honoured I was to introduce him!

Celebrating Manny! (Photo courtesy of Boudewijn Bertsch)

From Melbourne to Busan. Neighbours at IDF2019. Jo was speaking about living with a rare type of diabetes and Andy was there for support (and photos from rooftops).

This woman! Sana, deputy lead of the LWD Stream and a bright, fierce force.

Anita eloquently explaining the challenges of living with diabetes-related complications in Indonesia.

Apoorva highlighting #LanguageMatters in her talk.

Some of the most dynamic young people I have ever met at the Young Leaders in Diabetes Training Summit.

Cherise can always be relied upon to ask thoughtful questions.

I’ve lost count of the cities we’ve done our #DiabetesOnTour this year, but these blokes have made all my travel so much better! Thanks Bastian and Grumps.

My favourite people at IDF2019? The two baristas running this uber-hipster coffee van.

We were all surprised to see the room packed full at 8.30am on the last day of the Congress. Sex sells. Or people just want to talk about it…

One of the best pieces of advice I was ever give was this: surround yourself with smart women. This is the LWD stream from IDF2019. I truly was surrounded by the smartest of women! Thank you Sana, Pei Yan and Elizabeth.

The final session in the LWD and my highlight of the whole congress was my neighbour, Sol, talking about living with MODY 3. We could not have scripted a closing remark better than his: ‘Being at this conference has made me feel part of something and with people that understand.’ Welcome to the world of diabetes peer support, Sol. You are so, so very welcome here.
DISCLOSURE
I was the Chair of the Living with Diabetes Stream at the IDF Congress in Busan. My flights to Busan were covered by Ascensia Global (in order for me to get to Busan in time to co-facilitate their Social Media Summit). Flights home and accommodation were covered by the IDF.
Two years ago, I walked off the stage at the inaugural ADATS event feeling very shaken. I’m an experienced speaker, and regularly have presented topics that make the audience feel a little uncomfortable. I challenge the status quo and ask people to not accept the idea that something must be right just because ‘that’s how it’s always been done’. Pushing the envelope is something that I am more than happy to do.
But after that very brief talk I gave back in 2017, a mere three months after I started Looping, I swore I would never speak in front of a healthcare professional audience again.
That lasted all of about two months.
In hindsight, I was more than a little naïve at how my enthusiasm about user-led technologies would be received. I can still remember the look of outright horror on the face of one endo when I cheerfully confirmed:‘Yes! Any PWD can access the open source information about how to build their very own system. And isn’t that brilliant?!
Fast forward to last Friday, and what a different two years makes! The level of discomfort was far less, partly because more than just a couple of people in the room knew about DIYAPS. In the intervening years, there have been more talks, interviews and articles about this tech, and I suspect that a number of HCPs now have actually met real-life-walking-talking loopers. Plus, Diabetes Australia launched a position statement over a year ago, which I know has helped shape discussions between HCPs and PWDs.
I’ve gotten smarter too. I have rejigged the words I use, because apparently, #LanguageMatters (who knew?!), and the word ‘hack’ scares the shit out of people, so I don’t use it anymore. (Plus, it’s not really accurate.) And, to protect myself, I’ve added a disclaimer at the beginning of my talk – a slide to reinforce the sentiment that I always express when giving a talk about my own life with diabetes, accentuating that I am speaking about my own personal experiences only and that I don’t in any way, shape or form recommend this for anyone else. (And neither does my employer!)
I framed my talk this time – which had the fabulously alliterative title ‘Benefits, Barriers and Burdens of Diabetes Tech’ by explaining how I had wanted to provide more than just my own perspective of the ‘three B’s’. I am but one voice, so I’d crowd sourced on SoMe for some ideas to accompany my own. Here’s just some of the responses.
 (Click to enlarge)
(Click to enlarge)And this:

One of the recurring themes was people’s frustrations at having to wade through the options, keep up with the tech and customise (as much as possible) systems to work. And that is different for all of us. One person’s burden is another person’s benefit. For every person who reported information overload, another celebrated the data.
What’s just right for me is not going to be just right for the next person with diabetes. So, I used this slide:

I felt that the story of Goldilocks and the Three Bears was actually a really great analogy for diabetes tech. Unfortunately, my locks are anything but golden, so I needed a little (basic and pathetic) Photoshop help with that.
In this fairy tale, Goldilocks is presented with things that are meant to help her: porridge for her hunger, a seat to relieve her aching legs and then a bed to rest her head after her busy day. But she has to work through options, dealing with things that are not what she wants, until she finds the one that is just right.
Welcome to diabetes technology.
On top of working out what is just right for us, we have to contend with promises on the box that are rarely what is delivered to us. Hence, this slide:

Apart from the Dex add circled in red, all the other offerings are ‘perfect’ numbers, smack bang in the middle of that 4-8 target that we are urged to stay between. These perfect numbers, obviously belonging to perfect PWD with their perfect BGLs, were always completely alien to me.
A selection of my own glucose levels showed my reality.

I explained that in my search for finding what was ‘just right’, I had to actually look outside the box. In fact, for me to get those numbers promised on the box, I had to build something that didn’t come in one. (Hashtag: irony)
Welcome to Loop! And my next slide.

And that brings us back to two years ago and the first time I spoke about my Looping experience in front of healthcare professionals. It was after that talk, during a debrief with some of my favourite people, that this term was coined:

Funny thing is, that I am now actually the very definition of a ‘compliant’ PWD. I attend all my medical visits; I have an in-range A1c with hardly any hypos; I am not burnt out. And I have adopted a Goldilocks approach in the way I do diabetes: not too much (lest I be called obsessive) and not too little (lest I be called disengaged), but just right.
It turns out that for me to meet all those expectations placed on us by guidelines and our HCPs, I had to do it by moving right away from the things there meant to help us. The best thing I ever did was start Loop. And I will continue to wear my deliberate non-compliance as a badge of honour and explain how it is absolutely just right for me!
One of the many highlights for me at last week’s EASD meeting was the satellite event about DIYAPS. It was a Hacking Health event, co-organised by the OPEN Project consortium and promised to highlight the perspective of the #WeAreNotWaiting movement through the eyes of people with diabetes, researchers and clinicians.
It was standing room only, with the event having sold out a few days earlier. I was a little late (I had to present at an event involving early researchers and PWD) so unfortunately missed the always brilliant Dana Lewis kick off the event.
If you ever need someone to warm up an audience and set the scene about the DIYAPS movement, Dana is your person! I have seen her present a number of times now, and always pity anyone who shares the stage with her. Her presentations are always enthusiastic, articulate and engaging, and leave the audience wanting more.
I followed her talk on Twitter as I was in the cab from the EASD conference centre to the Centre Cívic Sagrada Família (bonus of offsite events is actually seeing some of the tourist attractions the city has to offer!) and could see that the audience was enchanted and galvanised with her talk.
The program was packed – and provided a balanced view of not only people using the tech (because honestly, sometimes it can sound like we have all drunk the Kool-Aid!), but also about DIYAPS in clinical practice, and research settings, as well as a session on medical ethics.
There were many stand out moments for me, but perhaps the one that stands out the most was from paediatric endo, and fellow Looper, Katarina Braune where she was able to distil DIYAPS into this single sentence (as tweeted by another Looper, Andrea Limbourg):

Perfect, perfect summary of looping!
We also heard from Roman Hovorka who presented on the experience of developing the Cambridge closed loop system (CamAPS). Anyone who has been following artificial pancreas technologies and research would know of Roman. I’ve heard him speak a number of times at conferences around the world and have always been grateful for his passion and dedication to advancing technologies to benefit people living with diabetes. So, it was a little surprising that I found his talk a little challenging.
One of the things that I have always admired about the DIYAPS movement is that there is a strong sense that our chosen DIY path sits neatly alongside commercial systems and regulatory bodies. While we may not choose or want to use a commercial system (and, of course, are not waiting for them), that doesn’t mean that there is disdain or derision of other options. In fact, there is admiration and gratitude for industry working to provide this technology to a broader audience. We know that not everyone wants to build their own system, and many ARE happy to wait for a system that will be in warranty, and comes straight out of a box, rather than cobbled together.
I say this knowing that same courtesy is not always afforded to the DIY world from industry, and I can point to every single time someone from a company developing a commercial automated system claims their systems are safe – implying that those of us in the #WeAreNotWaiting world are all cowboys not concerned with safety.
I would so have loved to have heard Roman really highlight all that his system has to offer, and what sets it apart from DIY systems, and how it is one more choice that will be available to PWD, rather than put down the DIY movement. I am all – ALL – about choice and love the idea that with this choice comes a better chance for us to find the tech that works best for our personal circumstances.
We don’t need to be defensive about ‘the other’ in diabetes technology. We need to acknowledge that there is no one right, perfect choice. DIY is certainly one of those choices, and as we heard sprinkled throughout the day, has been life changing for many people. But it is not the only option out there, and few people in the DIYAPS world would even suggest that it is. I guess perhaps that is what challenged me about Roman’s talk – he did seem to throw DIYAPS under the bus a little when it would have been far better to suggest it was just another bus route people may like to take.
So how could this event have been better? Well, I wish it had been part of the official EASD program. There is a lot of opportunity for HCPs to learn from the user-led tech community, and this extends to technologies and treatment options beyond DIYAPS. Reinforcing what is an overarching fact of life with diabetes – that all diabetes is DIY – is important for all working in diabetes to remember.
While DIYAPS technology may be at a far spectrum of the whole DIY diabetes idea, having HCPs and researchers listen to just how diabetes impacts on daily life, and the decisions we need to make is critical in their approach working with us.

Panel session to finish the day.
DISCLOSURES
My airfare and part of my accommodation to attend EASD was covered by Lilly Diabetes so that I could participate in the DOCLab advisory group meeting which took place all of Monday. Another night’s accommodation was covered by Novo Nordisk as I attended their advocate meeting on Digital Health Technologies.
I am part of the OPEN Project Consortium. I did not receive payment for my involvement in the Hacking Health event.
While my travel and some of my accommodation costs have been covered, my words remain all my own and I have not been asked to write or speak about any of the activities I attended, or anything I have seen at the conference. As ever, profanities are also all mine.
‘I’m bored with diabetes. So, so bored.’That was how I opened last week’s appointment with my endocrinologist.
She nodded at me. I’m sure it wasn’t the first time someone had commented on the boring nature of diabetes. It’s programmed into the DNA of the health condition we live with. She waited for me to go on (she really is the master of not filling silences).
‘What can I do to shake things up? What should I be doing?’
It was a repeat performance of my last appointment back in February. I walked in with this need to shake things up; do more; be more proactive; add stuff to my routine.
My endocrinologist, thoughtful as ever, waited some more for me to finish my brain dump. So, off I went…
‘I am doing so little to manage my diabetes these days. I’m not burnt out – that’s not what I am saying at all. I’m not doing that thing where I pretend I don’t have diabetes. I am doing everything I need to do, except these days, it seems I don’t really do much. Loop keeps Looping and I really feel that my only input is making sure there is insulin in my pump and a working cannula and sensor in place. I bolus as required.
‘But it doesn’t seem enough. There was time each day that I had set aside for diabetes that I don’t need anymore because managing rollercoaster glucose levels, or responding to countless alarms, or managing those hypos that resulted in multiple lost hours…these things just don’t happen anymore. Or if they do, they take so little time to address that it almost seems insignificant.
‘I feel like I am not doing enough. So…what can I do?’
When she knew I had finished sharing my stream of consciousness, she looked straight at me and said: ‘You do exactly what you are doing. There is nothing more that I would suggest or recommend that you do. You asked last time about adding some different therapies to your current management, but there is nothing that would suggest any benefit to that.
‘If you were not looping and doing what you used to have to do and all that entailed and telling me what you are telling me: that you are feeling well, you feel your diabetes is in a good place, you are not feeling burnt out and that you are happy with how and where your diabetes was tracking right now…and if that was accompanied by the A1c you are running, I don’t think we would be having this conversation. I doubt that you would be asking what more you could do. You would know that you are meeting all the targets you want to and are feeling overall great about your diabetes.’
Of course, she was right. That was my situation two years ago: I was feeling fine about my diabetes (or as fine as I ever was going to) and was thrilled with my A1c (which wasn’t as low as it is now). And I certainly wasn’t thinking that I needed to do more. I accepted that I was putting in the effort and for once was seeing the outcomes I liked. The idea of adding more tasks to my diabetes life would never have entered my mind!
‘I know you are right,’ I said to her and then mentioned the talk I’d heard at #DData last year when fellow DIY-er, Justin Walker, said that since using OpenAPS he saved himself about an hour a day. ‘An hour a day. That’s a lot of extra time I didn’t have before. I don’t know what to do with it,’ I paused. ‘Maybe I should take up knitting.’
‘You could learn a language in that time,’ she suggested, helpfully.
It has me wondering if this is a thing for others who have embraced the DIYAPS way of life. Have you all just embraced this renewed freedom and extra time and run with it, or are you too wondering what to do with your hands?
Nineteen years of constantly focusing on the minutiae of diabetes, and second guessing myself and having to DO SO MUCH diabetes is a really hard thing for me to unlearn. The last two years have been really, really different. Who knew that my response to finally getting that break that I so desperately wanted would be to not know what to do with myself and want to do more?!
Since Looping, diabetes has taken a back seat in my life because the daily demands are far fewer. Sure, the emotional toll is still somewhat there – especially when it comes to the fears I have about the future. But the daily frustrations and intrusions are not there. And that means that as well as having to physically do less, I think about it less. I had no idea just how much that all took until I stopped doing it.
I get that this is coming from a position of extraordinary privilege, and feel free to file it away under not only first world, but also first-class problems. And ignore me. (Seriously, I thought of myself as insufferable when I was having conversation last week.)
Or send me knitting patterns. In the meantime, I’ll be over in the corner conjugating irregular verbs.

I am not really the type to analyse reports of glucose data. I’ve never been like that, except for a brief period where I was overly obsessive. Or, as it is more commonly known: when pregnant. Then, I was all about entering numbers into Excel spreadsheets, (hey – it was the early 2000s), and I searching for patterns in the 15-20 BGL checks I was doing every day, circling anything even closely resembling a common theme in green. (Oh – green circles may always have been my thing…!)
These days, even with reports and graphs and all sorts of other fancy pants data at my fingertips, I don’t really do any analysis.
The reason I love Loop is because of how it makes me feel in the here and now. By reducing so many of the tasks I do, and my diabetes needing less urgent attention, plus dealing with fewer lows, fewer highs and fewer pretty much all the other shitty stuff, it means that my in-the-moment diabetes is far easier to manage.
Sure – I occasionally have a look at what my Clarity app is telling me, but it’s only ever the snapshot page: TIR, average glucose level and hypo risk.
Since being on Loop, my hypo risk has always looked like this:

Minimal risk. Take that in for a moment.
Diabetes – the condition that demands so much of us in terms of being able to complete highly complicated calculations factoring in pretty much every single variable imaginable and a million more, dosing a potentially lethal drug and really, no room for error.
Diabetes – the definition of a high-risk health condition.
And my personal risk of lows? Minimal.
So, remind me again: How is Loop (or other DIYAPS options) unsafe?
The day before ADA kicked off, I managed to catch a glimpse – my only glimpse this visit to San Francisco – of the Golden Gate Bridge from the back of an Uber on the way to the Diabetes Mine Summer DData Exchange (#DData19).
This is the third DData I’ve attended, and it always delivers. The speakers are brilliant and the topics on the agenda push some of the boundaries we’re used to seeing as part of the ADA conference that runs alongside. Amy Tenderich expertly emceed the day, and Mike Hoskins’ rapid fire tweeting made sure that those not in attendance had a birds eye view of the event.
This year, there was one session that really stood out for me and it was a panel session moderated by Adam Browne from diaTribe and included JDRF International CEO, Aaron Kowalksi and Alain Silk from the FDA.
For some time now, there have been efforts to move away from the idea of HbA1c being the be all and end when it comes to assessing the outcomes of diabetes management.
This doesn’t only mean in terms of the way we measure our own personal diabetes management, or the success or effectiveness of the devices, drugs or treatments on offer, it also is directed to researchers, clinicians and regulators who continue to use A1c as THE measure to determine the value of whatever they are talking about.
The push has been towards time in range (TIR) because with tools such as CGM and Flash glucose monitoring, this is something that can be easily measured and demonstrated.
The A1c is flawed – we all know that. Anyone with diabetes will have tales of A1cs going down, despite their diabetes management being more erratic, or conversely, their A1c increasing despite having fewer roller-coaster episodes. As a one-off number, it tells very little.
But while TIR is certainly one different way of having a look at just how we are tracking, with so few people actually using CGM or Flash (due to access and affordibilty), we can’t throw out other options. The A1c is not dead yet (just ask the queues of HCPs in the Exhibition hall at ADA waiting to get theirs done. Another blog post for another time…)
Also, TIR cannot be the only other measure we look towards as a substitute for A1c, and this session at DData explored more than the idea of a simple like for like between the two.
Aaron Kowalski highlighted how one of the first things people speak about when using an automated insulin delivery device is how their sleep improves. It was indeed the first thing that I noticed, and it was life changing for me. I noted that I slept like I did before diabetes!
Yet, this is not considered as part of regulatory decisions. Neither is how our diabetes experiences can be transformed. Aaron told the story of a young woman who rarely attended to diabetes tasks when around friends because she didn’t want to pull out her pump to check her CGM trace, or bolus insulin. She didn’t want to draw attention to herself or her diabetes. But being able to do those tasks by simply looking at her phone, or her smart watch meant that she felt so much better – and she did what she needed to do when she needed to do it. How are those improved experiences being documented and considered as part of why something is valuable?
In his earlier talk, Alain Silk from the FDA noted that one of the challenges when it comes to technology regulation is too much regulatory and contractual burden and not enough innovative devices getting into the hands of people with diabetes. The DIY movement manages to sidestep that first part and that means that we do have get to have those devices – those transformative devices – in our hands a lot sooner. Our experiences – which all seem to be positive – and our diabetes outcomes – which all seem to report improvements – really should count for something.
Surely one of the goals we are all seeking (and when I say all, I mean everyone involved in any aspect of diabetes) is to increase the time we DO NOT spend on diabetes anymore. At DData last year, DIY-er Justin Walker said that he believes he has gained back an hour a day since using an automated system. That’s seven hours a week. Over a year, that’s more than a total of fifteen days we get back from diabetes. Add that up over a lifetime of diabetes. It’s significant.
Aaron said that one of his goals as CEO of JDRF is to ‘…take diabetes out of our lives as much as is humanly possible.’ When devices allow us to do that – even if it’s just one little bit – that should be assessed as meaningful.
I have been thinking about this session a lot. In fact, anyone who has asked me about ADA has received a lecture on it. My poor boss got an earful when I returned to work on Monday. I’m pretty sure he regretted asking how I’d gone in San Francisco after I launched into a tirade about how we are simply not listening enough to people with diabetes when it comes to just what we are measuring as being valuable to us.
The problem with adding TIR to A1c as a way to assess devices, drugs or other therapies is that we still are focusing on nothing more than numbers. Sure TIR may be more robust and not simply a snapshot average, but it still attributes our success to a number.
When I talk about why Loop has been so transformative to me, I do mention TIR. But the biggest bangs for my buck – the things that really ring true – is not how much time I spend between two number goal posts.
No.
It’s about how much better I feel about my diabetes. It’s about how much less time, less worry, less stress I am forced to dedicate to diabetes. It’s about how the hypos I have these days take three minutes to deal with rather than three hours. It’s about how less stubborn, and how less frequent those highs are. It’s about the much lighter shadow diabetes casts over my family. It’s about sleep – oh dear god, it’s about sleep! It’s about how easy it is to carry out those required tasks and how little they interfere with my day. And it’s about the time I have been able to claim back as my own.
The footprint of diabetes is so far smaller these days than ever before. THAT is what is meaningful. THAT is what I measure. THAT is what it means to truly go beyond A1c.

DISLCOSURES
I attended ADA as part of my role at Diabetes Australia. My economy flights and accommodation have been covered by the organisation.
Thanks to the team at Diabetes Mine, who kindly provide diabetes advocates with the opportunity to attend their DData Exchange at a significantly reduce cost.






