
You are currently browsing the category archive for the ‘Advocacy’ category.
Recurring themes in diabetes recur for a reason: they impact people with diabetes. And stigma is one theme that you will hear people with diabetes speak about a lot. A. Lot.
Last week at the World Health Assembly in Geneva, there was much discussion about stigma – both within the diabetes and in other health condition spaces.
Stigma harms everyone. It goes without saying that there is no good form of stigma.
When speaking with people from other health organisations, it was interesting to learn that many see diabetes stakeholders as being leaders in addressing stigma.
There was a lot of interest in how we had come as far as we have. I shared what I knew and what I’ve been involved in and there was awe at the number of different activities that have involved so many stakeholders.
I agree that we are making strides in addressing diabetes-related stigma. But I’m afraid I wasn’t quite as enthusiastic as the people I spoke to who seemed to think that we had it all sorted. That’s sadly not the case. Every single week I hear from people with diabetes about the stigma they are experiencing, and the discrimination they have to deal with because of diabetes.
Last week, I found myself cringing at the airport when a security guard mentioned that perhaps if my diabetes was better managed I could stop using the devices attached to my body. He knew, you see. His niece has diabetes and she doesn’t need one of those machines.
I was too tired after hours of travel to do anything more than roll my eyes and say ‘That’s not how diabetes works’, and suggest that he doesn’t offer strangers unsolicited advice. I wondered if he had the same level of comfort telling someone wearing a pacemaker what to do to better manage their heart condition. Probably not.
And I snapped a sassy response on the Instagram page of one of my favourite bakers when someone suggested that dipping rhubarb in sugar was a one way ticket to diabetes. As if that’s all there is to this highly complex condition.
I’m tired and yet the stigma I deal with seems quite superficial when compared with that of many of my diabetes brothers and sisters living in other parts of the globe.
Diabetes stigma is real. It is harmful. It needs to end. And we all have a role to play in getting us to that end. I say that knowing that sometimes it’s too exhausting to do anything – and that’s perfectly okay. The full time job of managing diabetes is more than enough. Busting stigma shouldn’t also be on our to do list.
But if you have time, if you have the energy, if you have the will, there are some easy things you can do.
Sign the pledge to end diabetes stigma. You probably already have, especially if you’ve been hanging around here for a while. So perhaps, you could spend five minutes sharing the link to the pledge, or finding someone you know hasn’t signed it, and asking them to. It takes under a minute.
If you’re doing any sort of diabetes advocacy about stigma, circulate the International Consensus Statement to End Diabetes Stigma. Evidence matters, and this document brings together 51 experts across 18 countries. It was published in the Lancet and it is an excellent foundation for any work in the stigma space.
And if you want to see a video of joy, watch the one linked below. This is a compilation of what happened at the Summit to End Diabetes Stigma held in Jaipur in March this year. I assure you that amongst the colour and vibrancy you see in the video, there were difficult discussions, impactful panel sessions and plans for how to make real change.
My new friends from last week were impressed with what’s been done in the diabetes space, and I agree – the community has done so much already. But we’re not done. There’s a lot more to do. We’ve come this far because dedicated people have worked collaboratively. Community members have shown up to share their experiences. I’m so pleased to be part of these efforts. And will keep rolling up my sleeves as we address what still needs to be done.
There are some words that are very hard to write.
This post is full of those words, as is the announcement you can read in full below. I wrote those words over the weekend with such sadness and the heaviest of hearts.
There are few people in the diabetes community who don’t know the name Bastian Hauck. I’ve known Bastian for almost fourteen years now. We met at a European Bloggers Summit, hosted by J&J who, at the time, was the distributors of the Animas Insulin Pump. I don’t know why I was invited, but I am forever grateful I was there, because I met some of the most important people in my diabetes world at that meeting in Berlin.
Bastian was one of those people. He spoke about his adventures sailing around the world in a (small) boat. Not remotely relatable to me, but nonetheless, we became friends and since then, we have worked together in the diabetes advocacy space. The weekly #dedoc° tweetchat premiered the same week as the weekly #OzDOC tweetchats. (Remember those days?)
When Bastian started thinking about a program to bring people with a diabetes to diabetes professional conferences, he spoke with me about it at length. Any time we found ourselves in the same place, he’d share his thoughts and from there we tried to shape what would become the #dedoc° voices scholarship program. That program was launched in 2020, and since then, hundreds of people with a diabetes have been the recipients of a scholarship. The program is so precious and important, and it all happened because Bastian had an idea and didn’t stop working until he made it happen.
Bastian and I haven’t always agreed on things. In fact, there have been many occasions where we have come from polar opposite sides of an argument. In my role as an advisor to #dedoc°, I provide my advice, and he then does what he wants. Sometimes his decision ends up being fine, other times, he has realised that his decision was, perhaps, not the right one. I am pleased to say that I have screenshots of messages from him and videos of him saying. ‘Renza was right’. Damn, straight she was! (I write this knowing he is reading this and laughing/grimacing.)
Bastian’s big picture thinking will be his legacy. I’ve just used a word that he doesn’t like and has forbidden the #dedoc° team from using. But on this space, he doesn’t get to tone police my words. His refusal to stop until community is centred and valued is the reason that organisations such as ATTD, EASD and ISPAD now have dedicated roles for people with lived experience of diabetes. It’s the reason that so much global advocacy has happened the way it has – because the #dedoc° scholarship program provided opportunities for people to come together and build their ideas. This is, indeed, a legacy, and one of which I hope he is incredibly proud.
For the last few years, Bastian has been living with terminal cancer. During this time, I’ve listened to him share his experiences, his frustrations, details of his treatments, the positive moments. And, heartbreakingly, the moments where the news he has been given is incredibly confronting. Now is one of those times.
And so, please read the below message. It is for the #dedoc° voices and the diabetes community more broadly. It has been shared across #dedoc° channels, and I would encourage everyone to leave a message, if you’d like.
Our community has been built on the actions of giants, and one of those giants is Bastian Hauck. How fortunate so many people are to have benefitted from the community he has built and the opportunities he created.

Sunday is Feminist Christmas*. It’s the day that social media feeds turn pink and women get celebrated with morning teas (organised by women) and the lady folk are handed a cupcake (made by women) to shut us up and make us forget that women continue to live in a world designed and defined by patriarchy.
Isn’t that a joyful start to this article? I’ll wait while people shift uncomfortably and refer to me as an angry/difficult woman.
In the coming days in the diabetes world, you’ll see posts pointing to women in the diabetes landscape. These women are generally remarkable and doing great things. But oddly, rarely are the women whose faces appear on a social media carousel actually living with diabetes. A few years ago, I pointed out that while we should be recognising the clinicians and researchers improving our lives, women with diabetes are completely ignored.
So, a little hint to anyone who is putting together content for next week: don’t forget to also highlight the women with lived experience of diabetes who are actually doing so much of the work in our community. Those grassroots initiatives that continue to be life saving and life changing are very often powered by women with diabetes. And, as is often the case, these women do this work on a volunteer basis. All while managing a very demanding chronic health condition on top of all the other work women do.
In the meantime, you should all register for this year’s DiaLeb Annual Diabetes and Women Panel. This is the 7th year and I’m very excited to be on the panel with two remarkable women living with diabetes, and another two women with loved experience of diabetes. Be quick! It’s tomorrow!

Seriously, women with diabetes are brilliant. we deserve way more than a cupcake. But I’ll take one all the same if some bloke would like to organise it.
More on International Women’s Day at Diabetogenic
2023 – Deserving more than a cupcake
2019 – Interweb Jumble #34 – The IWD edit
*The brilliant Wilhelmina Stracke coined this term. You should follow her on Instagram.
So what has been occupying your minds over the first few weeks of the year? Well, for a while there (and still), mine was trying to understand the veritable PR disaster of the Adelaide Writers Week (AWW). Niche? Yes. Relevant to diabetes? Also yes. In a roundabout way.
Let me set the scene. A writers festival in Australia was cancelled after one of the speakers had her invitation rescinded. The simple explanation of this is that the speaker, academic and author Dr Randa Abdel-Fattah had made some comments on social media that were deemed controversial by the AWW Board. More concerning, they connected these comments with the shootings in Bondi in December last year, effectively associating Dr Abdel-Fattah with the shooters. I’m actually not here to comment on Dr Abdel-Fattah, other than to say her treatment was appalling. There has been a lot of commentary, and if you’re not from Australia (or are from Australia but somehow managed to miss it) simply google AWW for details of what happens when decisions are made without consultation or understanding of the affected community.
I specifically want to focus on one part of the whole saga and that is the decision makers responsible for the PR nightmare. The Board of the Adelaide Festival (who is also responsible for the AWW) made the decision without the support of AWW director, Dr Louise Adler AM or her team. Dr Adler, in a letter published in the Guardian after she resigned from her role highlighted that the board was ‘composed of individuals with little experience in the arts ‘, which lead to decisions being made without cultural context and an absence of understanding consequence.
Even before I’d read Dr Alder’s compelling and commentary, the conversations I was having with friends and family were homed in on the same themes. We knew that the other writers at the festival would withdraw from the festival, one by one. We knew that Dr Adler had been treated terribly. And we were waiting for the gaslighting that would come from the Board, and anyone else involved in the decision making.
We knew, because we are a family of artists. My husband is a professional musician. My daughter is studying writing and journalism and has a part time job writing for a local newspaper. I studied music at university. Our friends are musicians, composers, writers, film makers, makers and journalists. We’d had discussions with many of them about how the Board’s lack of understanding of the arts sector, the way the community would respond, and how the community would be impacted. The words I used were ‘They have no skin in the game’, and by that I meant that not only couldn’t they see what was coming, they could also walk away relatively unscathed. Their careers were unlikely limited by their involvement in the decision and even though the entire board resigned, I would bet that it hasn’t made a dent professional standing or income.
Yet it wasn’t the arts scene that was the focus of my thoughts when I considered the AWW board, the decisions they made, the lack of insight into community response or the inevitable and highly predictable fallout.
It was, of course, diabetes.
I found myself wandering around the house and on daily walks muttering ‘Nothing about us without us’ with a growing frustration that this lesson keeps having to be learnt the hard way.
It may be different communities and different contexts, but we’ve seen similar incidents play out just like this in the diabetes world for years. People with diabetes are not included in decision making processes. But then sit there, watching the fall out.
The process is the same. The positioning from the people making decisions is the same. Think about some pretty ridiculous diabetes decisions in recent years and think about who made them, and who wasn’t consulted. Think about the fallout from a particularly nasty diabetes campaign that adds to diabetes-related stigma. It’s with disbelief that I think back to campaign discussions when I was told outright that offending and upsetting people with diabetes when a campaign launched was the price to pay because we weren’t the intended audience, as if we would be magically shielded from the stigmatising messaging. And that it was an unintended consequence in efforts to inform the general public.
Those gaslighting me weren’t going to be in the firing line next time someone made some horrid comment about diabetes. It wasn’t their weekend that was going to be ruined when some smartarse in a supermarket queue or café said something about sugar causing diabetes or personal responsibility or how diabetes is a ticking time bomb.
When a decision is made that directly impacts people’s lives, surely those people should be in the room, at the table and have their voices heard the loudest. Surely. It’s so frequently not the case when diabetes decisions are made. It wasn’t the case when the AWW Board decided to cancel Dr Abdel-Fattah’s speaking engagement.
And so, the AWW was cancelled after almost all the writers on the program withdrew and the Board resigned. Interestingly, most of the Board members sit on other boards, so their status as ‘leaders’ and ‘decision makers’ doesn’t seem to be too impacted. Meanwhile, those writers have lost one of the few (and seemingly shrinking) opportunities to meet to share ideas and celebrate their community. Their incomes have been impacted. The chance to get their work in front of an audience has disappeared.
Nothing about us without us. It seems that this little catch phrase has been ignored too often, unless being used in convenient and cute attempts to demonstrate (usually lacking) community engagement. Instead, maybe it’s time to put us on boards and in leadership and decision-making positions. Maybe it’s time to actually listen to the people who know. Because our skin? It’s the one in the game more than anyone else’s. Raw, exposed and in the firing line.

It’s been a hot minute, hasn’t it. And by ‘hot’ I mean sweltering here in Melbourne. While my friends in the northern hemisphere are sharing snow photos, we’ve been dealing with days in the high 30s and 40s. (For my US friends – we hit almost 120°F this month. It was not nice.)
Anyway, now that the weather discussions are over, let me wish you all a belated happy new year. I’d like to say that I hope that your start to 2026 has been gentle and kind, but instead, picture me gesturing wildly at the world and shaking my head in despair.
I finished up 2025 feeling pretty damn exhausted and burnt out. But, really, who wasn’t feeling that way? There was a lot of good stuff that I could look back on, but the never-ending travel wore me out. I feel compelled to say that I know I am fortunate to do the work I do, and I love my job. Being able to work with people in the diabetes community who are making real change is a gift every single day. I would just be so happy if someone could find out a way for Australia to not be a 30-hour trip away from most of the places I need to visit.
I was lucky to have a three-week break over the Christmas/New Year period where I travelled no further than 5kms from my house, and I’ll have had a 10-week hiatus before I next find myself in an airport. Both of these breaks feel like a luxury!
But as we gear up for 2026, it’s undeniable that the global health world is in a mess and diabetes is not immune to that. I’m really pleased that some of my work will involve addressing issues that are important to people with diabetes. I’m beyond honoured to have been invited to give the Anita Carlson lecture at this month’s Psychosocial Aspects of Diabetes (PSAD) Conference (even happier that it’s being held in a regional city in my state and I only have to drive for an hour to get there!). I’ve called my lecture ‘Building Diabetes Healthcare from the Ground Up’ and it’s given me an opportunity to imagine just what diabetes healthcare could be if people with diabetes were actually centred and involved in its creation.
Next month the first Global Summit to End Diabetes Stigma is being held in Jaipur, India. Can you imagine hundreds of people with or working in diabetes coming together in one place to come up with meaningful and real strategies to end stigma? For disclosure purposes, this event is being funded via a grant from Breakthrough T1D (I work there), and I am involved in the planning of the event. It feels like a culmination of a lot of efforts highlighting the impact of stigma to get to a place where the diabetes world is ready to collaborate to end it. I’m so thrilled to be working for the organisation that has recognised that.
For me right now though, there is an overarching feeling that the world really is burning. While the US gets a lot of our attention, diabetes healthcare and access to insulin and care remains incredibly lacking in other parts of the world. As always, the most vulnerable in our world are impacted the most negatively. I don’t know about you, but a lot of the time I feel helpless.
Now it’s February, you may have once again seen that the annual Spare a Rose campaign has started. I think this is the fourteenth year of the campaign. I think back to what the diabetes community was like when Spare a Rose first started, and honestly, it feels very different to what we have today. I don’t know if a campaign like this would be started in today’s community. In fact, sometimes I find it harder and harder to find community and advocacy these days, as “influencer culture” takes hold.
And so, it’s worth remembering where Spare a Rose came from and the intentions behind it. It was a group of advocates in the US who wanted to give back somehow. I should point out that the advocates who started Spare a Rose had already given so much to the community. Many of them have taken a back seat to front-facing advocacy efforts but their legacies live on, even if fewer and fewer people see how they shaped the DOC. It’s diabetes advocates who have driven this campaign over the years and made sure that it has remained in the view of people with diabetes.
I have always loved the simplicity of Spare a Rose. The donation being asked for is small – US$5. For those needing a refresher, the idea is to give your loved one eleven rather than twelve roses and donate the saving to the campaign. In our house, we forgo flowers completely and recognise that empty vases are a small price to pay for making a donation to the value of a year’s worth of insulin.
I know that many are doing it tough these days. I also know that a lot of people who would have donated without a second thought in the past are unable to do so now due to changes of circumstances in so-called high-income countries.
But if you can support Spare a Rose by making a donation, please do. All funds go directly to the brilliant charity Insulin for Life, and each contribution makes a difference to a person with diabetes in a low-income country. If you can’t make a financial contribution, please share the website across your networks. Someone else in there might be able to donate. Every single dollar counts.
Click to donate!

How are we all doing this Diabetes Awareness Month? Are you feeling it? Or are you already over it – even though we’re just out of the first week, and the long haul is still ahead of us?
I’m on my way home from the ISPAD meeting. I’m at Montreal airport and I have another thirty hours ahead of me before I walk in the door home. I’m tired. But I’m energised. The privilege of spending a few days with diabetes advocates will do that.
Sitting here in the airport lounge, I opened Instagram and saw a post from Breakthrough T1D Advocacy. (And a little disclosure that I work in the Global Responsibility team at Breakthrough T1D.) The first slide was the statement ‘Why I Advocate’, and the following tiles shared responses from community members. I’m so annoyed I hadn’t seen this post before I got to ISPAD, because I would have loved to ask the #dedoc° voices their reasons for being such fierce and impactful advocates.
So…why do YOU advocate?
My answer? I advocate because I don’t know any other way to live with diabetes. Every day with diabetes is an act of advocacy. Some days that adds a burden that casts a very dark shadow, but some days it’s just life with diabetes. The wonderful Linxi Mytkolli introduced herself during her presentation at the #dedoc° symposium this week with ‘My full time job is managing my diabetes’, and then she went on to talk about her day job.
That’s diabetes: two jobs in one life.
While we may need to advocate all the time to simply live with diabetes, that doesn’t mean we need to be outspoken in the way we do it. It doesn’t mean we need to speak up or speak loudly or speak to rooms full of people. I hope people understand that advocacy can be on their terms, in their space, in their own way.
This week, my way has been to stand on the stage at ISPAD and talk about how research is one of the ways to end diabetes stigma. It was to amplify the #dedoc° voices and very loudly remind anyone who would listen that people with diabetes belong anywhere diabetes is being discussed. It was to chair two sessions which featured people with lived experience of diabetes speaking about their advocacy efforts.
And my way has also been a discussion in the airport lounge just ten minutes ago after changing my Omnipod and the person next to me wanted to chat about what I was doing. They were polite… ‘Do you mind me asking,’ they started. And no. In that moment, I didn’t. It felt light to share and answer questions about costs and advocacy initiatives to reduce those costs. It felt good to gently set the record straight when they said that diabetes was everywhere and it would just be better if people ate whole foods. And it felt positive when their response to me pointing out that stigma harms was, ‘I had no idea and I’ll be more careful about what I say’.
Two jobs. One life. Every little act of advocacy. Every little act of diabetes. Every single day.

Disclosure
ISPAD invited me to speak at this year’s meeting and covered by accommodation costs. Travel was part of my role at Breakthrough T1D.
My dad has always taken his parenting duties very seriously, and as such, he made sure that by the time I was ten years old, I had watched and rewatched all Marx Brothers movies to the point that I was able to recite the scripts word for word. I can’t tell you how many times I’ve watched ‘A Night at the Opera’, but it’s probably that movie and not twenty years of classical music training that means I can sing along to most of Il Trovatore.
My mum has never been a fan of the Marx Brothers. She’d roll her eyes while we were rolling around on the floor in fits of laughter, shaking her head and muttering that she simply didn’t understand what we found so amusing.
Does this mean she doesn’t have a sense of humour? Of course not, contrary to dad’s constant suggestion of as much. Mum regularly shares killer memes and jokes that are laugh out loud hilarious. It’s just that the Marx Brothers have never made her laugh (weirdo).
This showed me that people laugh at different things. One person’s funny bone tickler is another’s shrug of utter indifference.
One thing I learnt pretty early on when I started hanging out in the global online diabetes community is that humour is a really important coping mechanism for living with the condition. It makes sense, right? I mean, there are some pretty grim aspects of life with T1D, and having a laugh can lighten especially dark days, and help us keep perspective when things feel overwhelming.
Back in the OG DOC days, there were awards given to writers and people on social media, and one of the award categories was humour. I’ve tried to inject some humour into this blog over the years – you can be the judge how successful I’ve been. Read to the end and you’ll see I’ve linked to some posts where I tried to use jokes and humour to keep things a little lighter.
Sometimes, however, attempts at humour don’t land all that well. Or they land at the expense of others. And when that’s the case, I think we need to stop for a minute and check ourselves. Is it worth getting a laugh when you are punching down?
I don’t think so – especially because the result of punching down is often stigma. And we all know how I feel about that. Right? RIGHT?
None of this is new from me. I’ve been talking about how when people stigmatise any type of diabetes, we all suffer. I’ve been pretty blunt when calling out the T1D community for being outright nasty about people with other types of diabetes, especially people with T2D. The stigma we experience is a direct result of misinformation and ignorance about all types of diabetes. Contributing to it is not only nasty, but it is also voting against our own interests.
This post today has come about because over the last 24-hours a T1D Facebook group that I’m a member of has been embroiled in a fiery debate because one of the group’s moderators posted a meme that stigmatises type 2 diabetes. I’m not sharing the meme here, (because why would I add to diabetes stigma?) but I can describe it by saying that it highlighted a risk factor of T2D in a very stigmatising way. It was unoriginal, unamusing and unkind.
And it got messy. A number of people asked for the meme to be removed. Many were upset and found it offensive.
The moderators of the group doubled down. There were demands to scroll by and reminders that we were not there to ‘defend’ other types of diabetes. Comments pleading for the post to be removed were deleted and people were told they ‘Can’t take a joke’. I asked a few times for someone to please explain the ‘joke’, because I didn’t understand it. No one was able to do that. My comments were deleted anyway.
It astonishes me that the moderators of this group have chosen the hill they want to die on to be that it’s okay to stigmatise T2D and people should get over it if they don’t like it. They must have spent hours deleting comments and telling people to ‘get over themselves’. They repeatedly pointed out that the group is a T1D meme group with what seems an assumption that all people with T1D are happy for there to be nasty memes about T2D. Reassuringly, that’s not the case. A lot of people with T1D in the group are not impressed about the stigmatising posts and pop their heads above the parapet to let that be known.
A T1D meme page could be a source of joy, amusement, unity and some pretty clever humour, but instead, this group seems to regularly descend into bickering about what’s a joke and what’s just plain cruel, because many people with T1D don’t want to see T2D stigmatised or for misconceptions to be perpetuated. I’m one of those people.
And yes, I know that I can just leave the group. But one of the other things my dad, (and mum) taught me is that the standard you walk by is the standard you accept, and posting crappy, stigmatising, false and outright mean things about people with any type of diabetes is not a standard I accept. I call it out – regardless of who it is posting it.
I also want people to understand that these sorts of posts contribute to not just stigma about T2D, but to stigma about T1D as well. It constantly befuddles me that people who defend the right to be nasty and stigmatising about T2D are the same people who are up in arms when someone says something incorrect or stigmatising about T1D. The intellectual disconnect that can’t join the dots between the two issues is really something!
We can do better as a community. There are brilliant stories, jokes, and moments of wit that are truly hilarious, and we should be able to laugh about the shared absurdities and frustrations of life with T1D. But we can do it without throwing another group of people under the bus.

Want to see some truly funny things?
Watch Melissa Lee’s D-Parodies. Truly brilliant and hilarious.
Spoonful of Laughter from the team at dStigmatise brings comedians together to show how we can laugh about diabetes, and check stigma at the door.
Sam Morrison is one of the featured comedians on A Spoonful of Laughter and you can follow him, here.
Follow Brad Slaight! He’s hilarious.
Miss Diabetes manages to address some pretty serious issues around diabetes using her fabulous comics and artwork.
His Instagram handle is @type1comedian, and he’s damn funny! I’m not sure if any of Chelcie Rice’s stand up is online, but search for it and see if you get lucky.
And some questionable attempts of humour from me
Pancreas performance review (it’s really all about Effin’ Birds!)
My Lie on a Plate (rubbish influencers influencing rubbish)
Are you a diabetes expert? (This quiz has the answer!)
This is a transcript of a talk I gave earlier this year to a European-based health consultancy and creative agency about my take on global diabetes community-based advocacy – the opportunities and challenges. The title I was given was ‘Making Engagement the norm rather than the exception’. AI did a remarkably decent job with this transcript, but I expect that there might be some clunky language in there that I missed when I read through it on a plane after being in transit for 27 hours straight. Or, I could simply have used clunky language. Either way, it’s my fault.
I often say that community is everything, but I want to begin by saying that it’s important to understand that there is no single, homogenous diabetes community. Everyone’s diabetes experiences are different. I truly believe that there are some issues that unite us all, but really, we are a very disparate group – something I have come to understand more and more the longer I have been involved in diabetes community advocacy. This poses possibly the largest challenge for everyone in this room wanting to work with “THE diabetes community” because if you’re looking for a group that agrees on everything and believes the same thing, I’m sorry to say that you’re going to be in for quite a ride!
But it is also the biggest opportunity – and the way to get an edge – because it gives anyone who works in the diabetes space – from healthcare professionals, researchers, industry, diabetes organisations, policy makers, the media – to roll up their sleeves and make a concerted effort to talk with a wide range of people with diabetes to understand our experiences and what we need. Look, I know that it would be easier for all of you if I said, ‘Speak with one person and then you’re good to go’, but that would be a lie. Sadly, a lot of people and organisations still believe this to be the case, and I have a great example to show you why that doesn’t work.
And that example? It’s me, hi, I’m the problem, it’s me.
A number of years ago, a researcher reached out to me with an invitation to be the ‘consumer representative’ on their project. After bristling at the term “consumer”, I asked what the project was about, and this is what they said, word for word because I wrote it down and have told this story a million times as a cautionary tale: ‘It’s a project on erectile dysfunction in men with type 2 diabetes, diagnosed over the age of 65.’
There was not a note of irony in this invitation. When I pointed out that I fit literally none of the categories in the study and then went on to point out that I am a woman; I have T1D; no erectile dysfunction; diagnosed at 24; was not within a decade of 65 years of age, the response was ‘Oh, but you have diabetes, so you’ll be great’.
Friends, I would not have been great.
For the purposes of this discussion, when I say diabetes community, I am referring to people with lived experience of diabetes. There is a lot of cross over in the diabetes advocacy space, and there are many examples I can point to that show how valuable advocacy efforts can be when people with diabetes are involved in efforts led by diabetes organisations or other stakeholders. In fact, at the end of last year, we saw a brilliant example of that with Breakthrough T1D in Australia receiving $50.1 million in funding from the Australian government for their Clinical Research Network. This is the power of an organisation meaningfully engaging with their community to tell the story of why their advocacy is important. I mean, what is more compelling than hearing from people with diabetes and their families about how research holds the key to a better diabetes future?
I’d encourage you to look at Breakthrough T1D Australia’s socials to see just how beautifully they centred people with lived experience to get their message across, and how it was people with diabetes who literally marched on parliament to tell the story. The coordination of the campaign may have come from a passionate advocacy and comms team in an organisation, but the words were all people with diabetes. (For transparency: I work for Breakthrough T1D, formerly JDRF, but not for the Australian affiliate. I am, however, extraordinarily proud of what Breakthrough T1D Australia has achieved and so, so impressed with the way their communications campaigns are never about the organisation or staff, but rather about the community.)
I believe that our community excels in telling the stories of our lives with diabetes, what we need to make our lives better, what works in our communities and how we can better work together. Some standout examples of this include the #dedoc° community, and, in particular, the #dedoc° voices scholarship program. This is the only truly global community where diabetes advocates are not only present but are leading conversations. #dedoc° has no agenda other than to provide a platform for people with diabetes which results in diverse stories and experiences being heard. And it also means that organisations want to work with #dedoc° because it’s an easy way to connect with community. (And another point of transparency: I’m the Head of Advocacy for #dedoc°.)
Organisations that thrive on working with community demonstrate their commitment to improving the lives of people with diabetes in ways that matter. If you don’t know about the Sonia Nabeta Foundation (SNF), you really should! The foundation has a network of ‘warrior coordinators’ who provide peer support and a whole lot more! I have now had the honour of chairing sessions at international conferences with four of these warrior coordinators and I can say without a doubt that Hamida, Moses, Nathan and Ramadhan’s stories resonated and stayed with the audience way beyond the allotted ten minutes of their talks. Addressing the challenge of a limited workforce and resources by engaging and employing people with diabetes to educate and support younger people with diabetes is so sensible and clever. And the results are remarkable.
I have seen similar examples in India. Visiting Dr Archana Sarda’s Udaan centre in Aurangabad and Dr Krishnan Swaminathan’s centre in Coimbatore completely changed my understanding of peer-led education. And groups like the Diabesties Foundation and Blue Circle Diabetes Foundation (also in India) are prime examples of the successes we can expect when people with diabetes take charge of programs and lead diabetes education.
Seeing these examples firsthand lit a fire under me to challenge what we have been told in high-resourced countries like Australia, and here across high-income countries in Europe. Why is it that we, as people with diabetes, are told to stay in our lane and not provide education? We may be considered ‘higher resourced’, but people fall through cracks because they are not getting what they need. Health systems remain challenged and overwhelmed.
The challenge we have in places like Australia is that PWD are very clearly told that we are not qualified to provide education. Rubbish! Our lived experience expertise puts us in the prime position to do more than just tell our own story, and I believe we need to boldly push back on beliefs that only health professionals are equipped to fill education and knowledge gaps. Because in addition to what we know, the expertise we hold and our ability to speak in the language that PWD understand, we also know about ‘going to the people’ and not expecting a one size fits all approach to work.
It would be naïve to think that community-led, and -driven programs and initiatives aren’t already happening. Community is integral in providing information that PWD are desperate for, even with caveats about consulting HCPs. There are 24/7 support lines available in the community, something that is simply not available in most healthcare settings. And anyway, who better than others with diabetes to give practical advice on real life with diabetes than those walking similar paths? In the moment and with direct experience.
The #WeAreNotWaiting community was established to not just offer advice but develop technologies to improve lives of people with diabetes and continues to do so today. A five minute lurk in any of the online community groups dedicated to open-source technologies is all it takes to see people with diabetes who had been at the end of their tether with conventional care now thriving thanks to community intervention.
And that is replicated in low carb groups where community provides advice and education on how to eat in a way that is often not recommended by HCPs. People share experiences how they are flourishing thanks to making informed decisions to eat this way, and air their frustrations about how they are often derided by HCPs about those decisions. The support that comes from these groups is often just as focussed on how to deal with the healthcare environment when going against the grain (unintended pun) as sharing ideas and advice on how the science behind how low carb diets work.
T1D groups talk about incorporating adjunct therapies into their diabetes management, moving from a glucose-centric approaches to looking at other meds and interventions that can support better outcomes. GLP1s may not be approved for use by people with T1D, but they are increasingly being used off label because of their CVD and kidney protective nature. These community discussions include suggestions on how to have conversations with HCPs to ask about how adjunct therapies might help, including pushing back if there is a blanket ‘no, it’s off label’ response. Before anyone thinks this isn’t a good thing, I remind you that we still need prescriptions from our HCP before we can start on any new drug. We should be listened to when we ask to have a discussion about new and different ways to manage our diabetes.
And there are also businesses led by community that have stepped into spaces that are traditionally organisation or HCP-led. A few years ago, Aussie woman Ashley Hanger started Stripped Supply to fill a massive gap when diabetes supplies could no longer be ordered online and shipped, instead necessitating a backstep where PWD had to go into pharmacies to pick up supplies. Ashley’s start up gave the people what we wanted and meant that, for a small subscription fee, supplies could be straight to our doors again. And it’s run by community – what’s better than that?
There is contention about people with diabetes working with industry, and that is a conversation for another time. But I will say that when we have people with diabetes involved in the development of the devices that we use and/or wear on our bodies every day, the end products are better. That’s just a fact. When you have people with diabetes employed by device manufacturers writing education and instruction manuals for those devices, they make sense because they are written from the perspective of someone who actually understands the practical application of using those devices. It’s a massive opportunity for industry to engage – and employ – people with diabetes. Way to get an edge!
What I would say to everyone here today is that if you are not directly working with people with lived experience of diabetes, you are missing out on the biggest piece of the diabetes stakeholder puzzle. But you have to do it meaningfully and perhaps the biggest challenge I face is dealing with the rampant tokenism that exists in the diabetes ecosystem. For my entire advocacy career I have been urging the implementation of meaningful engagement, and to be honest, a lot of the time I feel that I have failed in those attempts. Every time I see a crappy program or campaign come out of somewhere that claims to work with community, I realise that people with diabetes are being used in possibly the most nefarious way possible: to ‘lived experience wash’ the work of the organisation. I wrote a piece earlier this year about this and was completely and utterly unsurprised to receive comments justifying poor attempts of consultation.
But then, I see something like the video I am going to finish with from Breakthrough T1D in the UK, and I know that there is intent there to do the right thing and do it properly. To involve people with diabetes from the beginning, and centre them throughout the work. The result is a beautiful piece of storytelling that has been shared across the globe. I don’t know the metrics, and quite frankly, I don’t care. All I need to see is the response from the community to know and understand that this hits the spot. And you can too with your work if you engage properly. We’re here to help.
You can watch What a Cure Feels Like, the Breakthrough T1D UK video that concluded my talk here.
Disclosure
I was invited by a health consultancy firm to give a talk to fifty people working on public-facing health campaigns (NDA, can’t say anything more) and then run a workshop about working with lived experience representatives. I was paid for my time to present and prepare for the session, and reimbursed for ground transfers to and from the location of the meeting.

Last week I was in Geneva for the 78th World Health Assembly (WHA78). It’s always interesting being at a health event that is not diabetes specific. It means that I get to learn from others working in the broader health space and see how common themes play out in different health conditions.
It’s also useful to see where there are synergies and opportunities to learn from the experiences of other health communities, and my particular focus is always on issues such as language and communications, lived experience and community-led advocacy.
What I was reminded of last week is that is that stigma is not siloed. It permeates across health conditions and is often fuelled by the same problematic assumptions and biases that I am very familiar with in the diabetes landscape.
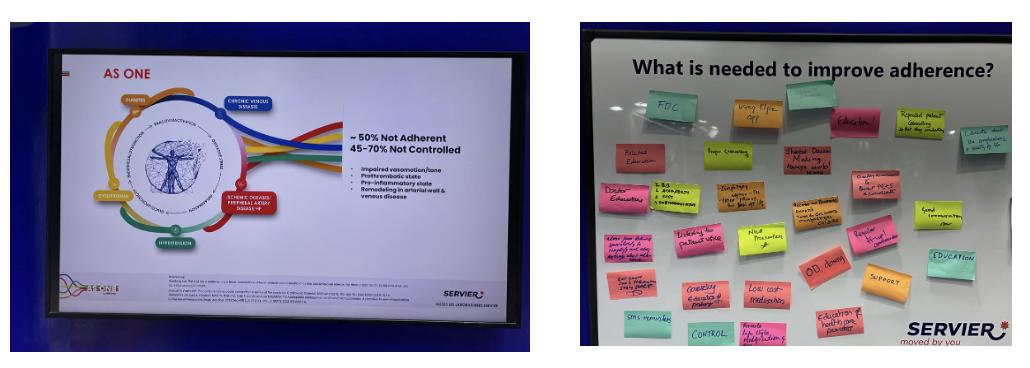
I eagerly attended a breakfast session titled ‘Better adherence, better control, better health’ presented by the World Heart Federation and sponsored by Servier. I say eagerly, because I was keen to understand just how and why the term ‘adherence’ continues to be the dominant framing when talking about treatment uptake (and medication taking). And I wanted to understand just how this language was acceptable that this was being used so determinately in one health space when it is so unaccepted in others. This was a follow on from the event at the IDF Congress last month and built on the World Heart Foundation’s World Adherence Day.

While the diabetes #LanguageMatters movement is well established, it is by no means the only one pushing back on unhelpful terminology. There has been research into communication and language for a number of health conditions and published guidance statements for other conditions such as HIV, obesity, mental health, and reproductive health, all challenging language that places blame on individuals instead of acknowledging broader systemic barriers.
I want to say from the outset that I believe that the speakers on the panel genuinely care about improving outcomes for people. But words matter as does the meaning behind those words. And when those words are delivered through paternalistic language it sends very contradictory messages. The focus of the event was very much heart conditions, although there was a representative from the IDF on the panel (more about that later). But regardless the health condition, the messaging was stigmatising.
The barriers to people following treatment plans and taking medications as prescribed were clearly outlined by the speakers – and they are not insignificant. In fact, each speaker took time to highlight these barriers and emphasise how substantial they are. I’m wary to share any of the slides because honestly, the language is so problematic, but I am going to share this one because it shows that the speakers were very aware and transparent about the myriad reasons that someone may not be able to start, continue with or consistently follow a treatment plan.
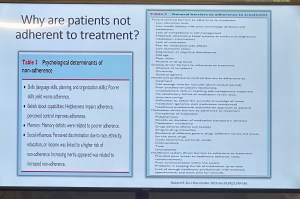
You’ll see that all the usual suspects are there: unaffordable pricing, patchy supply chains, unpleasant side effects, lack of culturally relevant options, varying levels of health literacy and limited engagement from healthcare professionals because working under conditions don’t allow the time they need.
And yet, despite the acknowledgement there is still an air of finger pointing and blaming that accompanies the messaging. This makes absolutely no sense to me. How is it possible to consider personal responsibility as a key reason for lack of engagement with treatment when the reasons are often way beyond the control of the individual?
The question should not be: Why are people not taking their medications? Especially as in so many situations medications are too expensive, not available, too complicated to manage, require unreasonable or inflexible time to take the meds, or come with side effects that significant impact quality of life. Being told to ‘push through’ those side effects without support or alternatives isn’t a solution. It is dismissive and is not in any way person-centred care.
The questions that should be asked are: How do we make meds more affordable, easier to take, and accessible? What are the opportunities to co-design treatment and medication plans with the people who are going to be following them? How do we remove the systemic barriers that make following these plans out of reach?
One of the slides presented showed the percentage people with different chronic conditions not following treatment. Have a look:

My initial thought was not ‘Look at those naughty people not doing what they’re told’. It was this: if 90% of people with a specific condition are not following the prescribed treatment plan, I would suggest – in fact, I did suggest when I took the microphone – the problem is not with the people.
It is with the treatment. Of course it is with the treatment.
The problem with the language of adherence is that it frames outcomes through the lens of personal responsibility. It absolves policy makers of any duty to act and address the structural, economic and systemic barriers that prevent people from accessing and maintaining treatment. Why would they intervene and develop policy if the issue is seen as people being lazy or not committing to their health?
And it means the healthcare professionals are let off the hook. It assumes they are the holders of all knowledge, the giver of treatment and medications, and the person in front of them is there do what they are told.
There is no room in that model for questions, preferences, or complexity. There is no room for lived experience. There are no opportunities for co-design, meaningful engagement or developing plans that are likely to result in better outcomes.
When the room was opened up to questions, I raised these concerns, and the response from the emcee was somewhat dismissive. In fact, she tried to shut me down before I had a chance to make my (short) comment and ask a question. I’ve been in this game long enough to know when to push through, so I did. I also don’t take kindly to anyone shutting down someone with lived experience, especially in a session where our perspective was seriously lacking. Her response was to suggest that diabetes is different. I suggest (actually, I know) she is wrong.
And I will also add: while there was a person with lived experience on the panel, they were given two questions and had minimal space to contribute beyond that. I understand that there were delays that meant they arrived just in time for their session, but they were not included in the list of speakers on the flyer for the event while all the health professionals and those with organisation affiliation were. There comments were at the very end of the session, and I was reminded of this piece I wrote back in 2016 where health blogger and activist Britt Johnson was expected to feel grateful that the emcee, who had ignored her throughout a panel discussion, gave her the last five minutes to contribute.
Collectively this all points to a bigger issue, and we should name that for what it is: tokenism.
I didn’t point this out at the time, but here is a free tip for all health event organisers: getting someone to emcee who is a journalist or on-air reporter does not necessarily a good emcee make. Because when you have someone with a superficial understanding of the nuance and complexity involved in living with a chronic health condition, or understand the power dynamics and sensitivities required when facilitating a conversation about long-term health conditions, you wind up with a presenter who may be able to introduce speakers, but you miss out on meaningful and empathetic framing of the situation. There are people with lived experience who are excellent emcees and moderators, and bring that authenticity to the role. Use them. (Or get someone like Femi Oke who moderated the Helmsley + Access to Medicine Foundation session later in the day. She had obviously done her homework and was absolutely brilliant.)
I know that there has been a lot of attention to language in the diabetes space. But we are not alone. In fact, so much of my understanding has come from the work done by those in the HIV/AIDS community who led the way for language reform. There are also language movements in cancer care, obesity, mental health and more. And even if there are not official guidelines, it takes nothing to listen to community voices to understand how words and communication impact us.
So where to from here? In my comment to the panel, I urged the World Heart Foundation to reconsider the name of their campaign. Rather than framing their activities around adherence, I encouraged them to look for ways to support engagement and work with communities to find a balance in their communications. I asked that they continue to focus on naming the barriers that were outlined in the presentations, and shift from ‘How to we get people to follow?’ to ‘How do we work with people to understand what it is that they can and want to follow?’.
Finally, it was great to see International Diabetes Federation VP Jackie Malouf on the program on the panel. She was there to represent the IDF, but also brought loved experience as the mother of a child with diabetes. The IDF had endorsed World Adherence Day and perhaps had seen some of the public backlash about the campaign and the IDF’s support. Jackie eloquently made the point about how the use of the word was problematic and reinforced stigma and exclusion, and that there needs to be better engagement with the community before continuing with the initiative.
One of the things of which I am most proud is seeing how the language matters movement has really made people stop and think about how we communicate about diabetes. Of course, there’s still a long way to go, but it is very clear that there have been great strides made to improve the framing of diabetes.
One area where there has been a noticeable difference is at diabetes conferences. I’m not for a moment suggesting that there is never negative language used at conferences and meetings, but the clangers stand out now and are likely to be highlighted by someone (i.e. #dedoc° voices) in the audience.
Earlier this month, the 75th IDF World Congress was held in Bangkok. Sadly, there was no livestream of the Congress, but it’s a funny thing when you have a lot of friends and colleagues (i.e. #dedoc° voices) in attendance. It meant that I had my own livestream. Sadly, the majority of what I was being sent were the language clangers.
But let’s step back a week or so to before the Congress even started. I was feeling horrendous and my brain was in a foggy, virus haze, yet I still managed to be indignant and vent at the horrendously titled ‘World Adherence Day’ which was being ‘celebrated’ on 27 March. Here is my post from LinkedIn, which has been viewed close to 12,000 times:

What I didn’t say in my post was that the IDF had eagerly endorsed the day with a media release and social media posts. My LinkedIn post took all my energy for that day, and I didn’t get a chance to follow up with the IDF. Plus, I assumed their attention would have been focused very much on the upcoming Congress.
Also, I hoped that it was a one-off misstep. I mean, surely the organisation had learnt its lesson after the Congress in South Korea when I boldly challenged incoming-president Andrew Boulton for his suggestion that people with diabetes need some ‘fear arousal’ to understand how serious diabetes is. You can see the video of my response to that at the end of this post and read the article I co-authored (Boulton was another co-author) about language here.
Alas, I was wrong. Just days before the Congress started, I saw flyers for this session shared online:

I was horrified and commented on a couple of the posts I saw. I was surprised to see some responses from advocates which amounted to ‘We can deal with it when we get there.’ Here are reasons that isn’t good enough. Firstly – not everyone is there, so all they see is the promotional of an event, comfortably using stigmatising language. It suggests that this language and the meaning behind it is okay. The discussion shouldn’t be happening after the fact. In fact, the question we should be asking is: HOW did this even happen? Where were the people with lived experience on the organising committee of the Congress speaking up about this? Did they get to see it before it was publicised? And how did the IDF miss it? This is, after all, the organisation that launched a ‘Language Philosophy’ document in 2014 (which sadly seems to be unavailable online today). It’s also the organisation that has invited me to give a number of talks about the importance of using appropriate and effective communication to IDF staff, attendees of the Young Leaders Program and as an invited speaker at a number of Congresses.
A major sponsor at the IDF Congress seemed to be very excited about the word adherence. In fact, it appeared over and over in their materials at the Congress. Here is just a couple of their questionable messaging sent to me by people (i.e. #dedoc° voices) attending the Congress:
I will point out that the IDF obviously understands the impact of stigma on people with diabetes and the harm it causes. There were sessions at the Congress dedicated to diabetes-related stigma and how to address it. In fact, I had been invited to give one of those talks. But what is disappointing is that despite this, terminology that contributes to stigma is being used without question.
I wasn’t at the Congress but from what I saw there was indeed a vibrant lived experience cohort there. #dedoc° had a scholarship program, and, as usual, there was a Living with Diabetes stream. However, I will point out that the LWD stream was not chaired by a grassroots advocate as has been the case for all previous LWD streams. It was chaired by a doctor with diabetes and while I am in no way trying to delegitimise his lived experience, I am unapologetically saying that this is a backwards step by the IDF. When there is an opportunity for a person with diabetes who is not also a health professional is given to a health professional or a researcher, that’s a missed opportunity for a person with diabetes. There were seven streams at the IDF Congress. All except for one are 100% chaired by clinicians and researchers. Only the LWD stream is open to PWD. I know that when I chaired the stream, the four members of the committee were diligent about looking through the entire and identifying any sessions that could be considered problematic for people with diabetes. It appears that didn’t happen this time.
All of this points to a persistent disconnect. It is undeniable that the language matters movement is growing, but it is still not embedded across the board—even within organisations that should know better. If we are serious about addressing stigma and centring lived experience in diabetes care, then language can’t be an afterthought or a debate to have after the posters are printed and the sessions are underway. It must be part of the planning and the review process. The easiest way to connect the dots is to ensure the lived experience community is not only present, but also listened to, respected, and in positions to influence and lead. We are long past the point where being in the room or offered a solitary seat is enough – the room is ours; we are the table.
Postscript:
I have written extensively on why language – and in particular the word ‘adherence’ – is problematic. It’s old news to me and to many others as well. This piece isn’t about that. But if you want to know why it’s problematic, here’s an old post you can read.
Disclosures:
I was an invited to give a talk about diabetes-related stigma at the IDF Congress in Bangkok, but disappointingly, had to cancel my attendance due to illness. The invitation included flights and accommodation as well as Congress registration. I was also on the program for two other sessions and was due to present to the YLD Program.
Other IDF disclosures: I have been faculty for the YLD Program for the last 10 years; I chaired the LWD Stream at the 2019 Congress and was deputy chair of the 2017 Congress.






