
You are currently browsing the category archive for the ‘DOC’ category.
Sunday is Feminist Christmas*. It’s the day that social media feeds turn pink and women get celebrated with morning teas (organised by women) and the lady folk are handed a cupcake (made by women) to shut us up and make us forget that women continue to live in a world designed and defined by patriarchy.
Isn’t that a joyful start to this article? I’ll wait while people shift uncomfortably and refer to me as an angry/difficult woman.
In the coming days in the diabetes world, you’ll see posts pointing to women in the diabetes landscape. These women are generally remarkable and doing great things. But oddly, rarely are the women whose faces appear on a social media carousel actually living with diabetes. A few years ago, I pointed out that while we should be recognising the clinicians and researchers improving our lives, women with diabetes are completely ignored.
So, a little hint to anyone who is putting together content for next week: don’t forget to also highlight the women with lived experience of diabetes who are actually doing so much of the work in our community. Those grassroots initiatives that continue to be life saving and life changing are very often powered by women with diabetes. And, as is often the case, these women do this work on a volunteer basis. All while managing a very demanding chronic health condition on top of all the other work women do.
In the meantime, you should all register for this year’s DiaLeb Annual Diabetes and Women Panel. This is the 7th year and I’m very excited to be on the panel with two remarkable women living with diabetes, and another two women with loved experience of diabetes. Be quick! It’s tomorrow!

Seriously, women with diabetes are brilliant. we deserve way more than a cupcake. But I’ll take one all the same if some bloke would like to organise it.
More on International Women’s Day at Diabetogenic
2023 – Deserving more than a cupcake
2019 – Interweb Jumble #34 – The IWD edit
*The brilliant Wilhelmina Stracke coined this term. You should follow her on Instagram.
This is a transcript of a talk I gave earlier this year to a European-based health consultancy and creative agency about my take on global diabetes community-based advocacy – the opportunities and challenges. The title I was given was ‘Making Engagement the norm rather than the exception’. AI did a remarkably decent job with this transcript, but I expect that there might be some clunky language in there that I missed when I read through it on a plane after being in transit for 27 hours straight. Or, I could simply have used clunky language. Either way, it’s my fault.
I often say that community is everything, but I want to begin by saying that it’s important to understand that there is no single, homogenous diabetes community. Everyone’s diabetes experiences are different. I truly believe that there are some issues that unite us all, but really, we are a very disparate group – something I have come to understand more and more the longer I have been involved in diabetes community advocacy. This poses possibly the largest challenge for everyone in this room wanting to work with “THE diabetes community” because if you’re looking for a group that agrees on everything and believes the same thing, I’m sorry to say that you’re going to be in for quite a ride!
But it is also the biggest opportunity – and the way to get an edge – because it gives anyone who works in the diabetes space – from healthcare professionals, researchers, industry, diabetes organisations, policy makers, the media – to roll up their sleeves and make a concerted effort to talk with a wide range of people with diabetes to understand our experiences and what we need. Look, I know that it would be easier for all of you if I said, ‘Speak with one person and then you’re good to go’, but that would be a lie. Sadly, a lot of people and organisations still believe this to be the case, and I have a great example to show you why that doesn’t work.
And that example? It’s me, hi, I’m the problem, it’s me.
A number of years ago, a researcher reached out to me with an invitation to be the ‘consumer representative’ on their project. After bristling at the term “consumer”, I asked what the project was about, and this is what they said, word for word because I wrote it down and have told this story a million times as a cautionary tale: ‘It’s a project on erectile dysfunction in men with type 2 diabetes, diagnosed over the age of 65.’
There was not a note of irony in this invitation. When I pointed out that I fit literally none of the categories in the study and then went on to point out that I am a woman; I have T1D; no erectile dysfunction; diagnosed at 24; was not within a decade of 65 years of age, the response was ‘Oh, but you have diabetes, so you’ll be great’.
Friends, I would not have been great.
For the purposes of this discussion, when I say diabetes community, I am referring to people with lived experience of diabetes. There is a lot of cross over in the diabetes advocacy space, and there are many examples I can point to that show how valuable advocacy efforts can be when people with diabetes are involved in efforts led by diabetes organisations or other stakeholders. In fact, at the end of last year, we saw a brilliant example of that with Breakthrough T1D in Australia receiving $50.1 million in funding from the Australian government for their Clinical Research Network. This is the power of an organisation meaningfully engaging with their community to tell the story of why their advocacy is important. I mean, what is more compelling than hearing from people with diabetes and their families about how research holds the key to a better diabetes future?
I’d encourage you to look at Breakthrough T1D Australia’s socials to see just how beautifully they centred people with lived experience to get their message across, and how it was people with diabetes who literally marched on parliament to tell the story. The coordination of the campaign may have come from a passionate advocacy and comms team in an organisation, but the words were all people with diabetes. (For transparency: I work for Breakthrough T1D, formerly JDRF, but not for the Australian affiliate. I am, however, extraordinarily proud of what Breakthrough T1D Australia has achieved and so, so impressed with the way their communications campaigns are never about the organisation or staff, but rather about the community.)
I believe that our community excels in telling the stories of our lives with diabetes, what we need to make our lives better, what works in our communities and how we can better work together. Some standout examples of this include the #dedoc° community, and, in particular, the #dedoc° voices scholarship program. This is the only truly global community where diabetes advocates are not only present but are leading conversations. #dedoc° has no agenda other than to provide a platform for people with diabetes which results in diverse stories and experiences being heard. And it also means that organisations want to work with #dedoc° because it’s an easy way to connect with community. (And another point of transparency: I’m the Head of Advocacy for #dedoc°.)
Organisations that thrive on working with community demonstrate their commitment to improving the lives of people with diabetes in ways that matter. If you don’t know about the Sonia Nabeta Foundation (SNF), you really should! The foundation has a network of ‘warrior coordinators’ who provide peer support and a whole lot more! I have now had the honour of chairing sessions at international conferences with four of these warrior coordinators and I can say without a doubt that Hamida, Moses, Nathan and Ramadhan’s stories resonated and stayed with the audience way beyond the allotted ten minutes of their talks. Addressing the challenge of a limited workforce and resources by engaging and employing people with diabetes to educate and support younger people with diabetes is so sensible and clever. And the results are remarkable.
I have seen similar examples in India. Visiting Dr Archana Sarda’s Udaan centre in Aurangabad and Dr Krishnan Swaminathan’s centre in Coimbatore completely changed my understanding of peer-led education. And groups like the Diabesties Foundation and Blue Circle Diabetes Foundation (also in India) are prime examples of the successes we can expect when people with diabetes take charge of programs and lead diabetes education.
Seeing these examples firsthand lit a fire under me to challenge what we have been told in high-resourced countries like Australia, and here across high-income countries in Europe. Why is it that we, as people with diabetes, are told to stay in our lane and not provide education? We may be considered ‘higher resourced’, but people fall through cracks because they are not getting what they need. Health systems remain challenged and overwhelmed.
The challenge we have in places like Australia is that PWD are very clearly told that we are not qualified to provide education. Rubbish! Our lived experience expertise puts us in the prime position to do more than just tell our own story, and I believe we need to boldly push back on beliefs that only health professionals are equipped to fill education and knowledge gaps. Because in addition to what we know, the expertise we hold and our ability to speak in the language that PWD understand, we also know about ‘going to the people’ and not expecting a one size fits all approach to work.
It would be naïve to think that community-led, and -driven programs and initiatives aren’t already happening. Community is integral in providing information that PWD are desperate for, even with caveats about consulting HCPs. There are 24/7 support lines available in the community, something that is simply not available in most healthcare settings. And anyway, who better than others with diabetes to give practical advice on real life with diabetes than those walking similar paths? In the moment and with direct experience.
The #WeAreNotWaiting community was established to not just offer advice but develop technologies to improve lives of people with diabetes and continues to do so today. A five minute lurk in any of the online community groups dedicated to open-source technologies is all it takes to see people with diabetes who had been at the end of their tether with conventional care now thriving thanks to community intervention.
And that is replicated in low carb groups where community provides advice and education on how to eat in a way that is often not recommended by HCPs. People share experiences how they are flourishing thanks to making informed decisions to eat this way, and air their frustrations about how they are often derided by HCPs about those decisions. The support that comes from these groups is often just as focussed on how to deal with the healthcare environment when going against the grain (unintended pun) as sharing ideas and advice on how the science behind how low carb diets work.
T1D groups talk about incorporating adjunct therapies into their diabetes management, moving from a glucose-centric approaches to looking at other meds and interventions that can support better outcomes. GLP1s may not be approved for use by people with T1D, but they are increasingly being used off label because of their CVD and kidney protective nature. These community discussions include suggestions on how to have conversations with HCPs to ask about how adjunct therapies might help, including pushing back if there is a blanket ‘no, it’s off label’ response. Before anyone thinks this isn’t a good thing, I remind you that we still need prescriptions from our HCP before we can start on any new drug. We should be listened to when we ask to have a discussion about new and different ways to manage our diabetes.
And there are also businesses led by community that have stepped into spaces that are traditionally organisation or HCP-led. A few years ago, Aussie woman Ashley Hanger started Stripped Supply to fill a massive gap when diabetes supplies could no longer be ordered online and shipped, instead necessitating a backstep where PWD had to go into pharmacies to pick up supplies. Ashley’s start up gave the people what we wanted and meant that, for a small subscription fee, supplies could be straight to our doors again. And it’s run by community – what’s better than that?
There is contention about people with diabetes working with industry, and that is a conversation for another time. But I will say that when we have people with diabetes involved in the development of the devices that we use and/or wear on our bodies every day, the end products are better. That’s just a fact. When you have people with diabetes employed by device manufacturers writing education and instruction manuals for those devices, they make sense because they are written from the perspective of someone who actually understands the practical application of using those devices. It’s a massive opportunity for industry to engage – and employ – people with diabetes. Way to get an edge!
What I would say to everyone here today is that if you are not directly working with people with lived experience of diabetes, you are missing out on the biggest piece of the diabetes stakeholder puzzle. But you have to do it meaningfully and perhaps the biggest challenge I face is dealing with the rampant tokenism that exists in the diabetes ecosystem. For my entire advocacy career I have been urging the implementation of meaningful engagement, and to be honest, a lot of the time I feel that I have failed in those attempts. Every time I see a crappy program or campaign come out of somewhere that claims to work with community, I realise that people with diabetes are being used in possibly the most nefarious way possible: to ‘lived experience wash’ the work of the organisation. I wrote a piece earlier this year about this and was completely and utterly unsurprised to receive comments justifying poor attempts of consultation.
But then, I see something like the video I am going to finish with from Breakthrough T1D in the UK, and I know that there is intent there to do the right thing and do it properly. To involve people with diabetes from the beginning, and centre them throughout the work. The result is a beautiful piece of storytelling that has been shared across the globe. I don’t know the metrics, and quite frankly, I don’t care. All I need to see is the response from the community to know and understand that this hits the spot. And you can too with your work if you engage properly. We’re here to help.
You can watch What a Cure Feels Like, the Breakthrough T1D UK video that concluded my talk here.
Disclosure
I was invited by a health consultancy firm to give a talk to fifty people working on public-facing health campaigns (NDA, can’t say anything more) and then run a workshop about working with lived experience representatives. I was paid for my time to present and prepare for the session, and reimbursed for ground transfers to and from the location of the meeting.

Just what is the emotional labour associated with living with a life-long health condition like diabetes? I’ve been thinking about it a lot this week, firstly because I was asked to give a talk about it to a group of researchers to help them understand barriers they may experience with getting participants into their research. It was a great discussion, with plenty of questions and hopefully a new understanding of the burden diabetes unleashes on us. And then, I thought about it when I was feeling the weight of that burden – more so than usual.
The emotional labour of living with diabetes is a complex, often invisible force, shaping our lived experience in profound ways. It’s the mental and emotional effort we put into the never-ending demands of the condition. It’s accompanied by an inner dialogue that asks if we’re doing enough, trying enough, feeling enough, being enough. It comes on top of the physical labour of doing diabetes, which in itself, is significant. It’s an ever-accruing emotional toll of being perpetually alert, constant decision making and wondering how those decisions might impact our immediate and long-term health and wellbeing. The emotional resilience required to do diabetes each day is an additional burden of itself, the sum of all these parts equalling an unforgiving weight that, at times, just feels too damn heavy to carry anymore.
But it doesn’t end there. Living with diabetes is an act of advocacy in itself, even if that advocacy is for ourselves alone and whether we use the word or not. Some people who take on advocacy issues and causes, leading efforts, participating in them, speaking about them. Whether involved in advocacy as a paid day job, consulting-type role, voluntarily, or a hybrid version (me), all of it adds to the emotional labour of diabetes.
Of course advocacy can be energising – striving for better healthcare, pushing for more understanding, and campaigning for supportive policies are endeavours close to our hearts and seeing efforts result in stunning outcomes bolster our energy levels. Working together with others with diabetes to change our communities is motivating. But it can also be exhausting. Each act of advocacy draws from our already limited reserves. The constant need to explain, to justify, to fight for our rights and needs can lead to burnout, leaving us feeling drained and disheartened in a fight that seems unending.
That’s where I spent a lot of this week: drained, disheartened, devastated and frequently teary with the weight of advocacy casting a long, dark shadow.
I know that this is something people with diabetes speak about, and the mental health of diabetes is finally on agendas, but it still needs to be said that being adjacent to diabetes, or being a champion for mental healthcare doesn’t offer a true understanding of just what it feels like. The best allies I know are the ones who recognise this gap in understanding and do all they can to ensure they don’t add to it and try to learn by stepping back and not overshadowing our voices or efforts.
One of the ways people with diabetes have attempted to deal with this labour and resulting burnout is to build peer communities and networks. Solace from the weight of diabetes can be found in others with shared experiences in sanctuaries where our struggles don’t need to be explained but they are deeply understood. These are safe spaces where we exchange stories, share tips, and buoy each other’s spirits. These communities become a wellspring of support and encouragement, where our emotional labour is shared, and our advocacy efforts are collectively bolstered. Safeguarding those spaces is essential if we’re to draw strength from them rather than find ourselves being overwhelmed by them.
In recent years, I’ve found myself becoming more and more selective about where I find that support. Twitter was probably the first to be left behind as I no longer found it a safe space. I’m reminded of that any time I venture back an innocent tweet about my own diabetes choices is attacked from some low carb bro. I replaced the openness of social platforms with closed group chats of others with diabetes, knowing that the support was there without the risk of trolling. Those chats provide the light to guide my way through the shadows.
This week, with the heaviness of all that is diabetes weighing me down, it has been difficult to find that light. The networks I have are always there, but even that is sometimes not enough when everything is overwhelming. Hosting this week’s #docday°, and hearing from advocates from around the world doing incredible things wasn’t enough to help me see clear. I thought of how to push through this, and I don’t have an answer. Except this: One of the things we do so well in our community is lift each other up because our community and other people with diabetes are everything. And so, even while I am feeling weighted down, I can focus on that. And hope that in amplifying and cheerleading my peers with diabetes and their efforts, I’ll rise too.
Two community things you should know about…
Spare A Rose, Save a Life is continuing to accept donations here. Thanks to amazing advocate Tinotenda for driving this year’s campaign.
Sign and share this petition and read the consensus statement initiated by a group of #dedoc° voices which is calling for uninterrupted insulin access in humanitarian crises. Congrats to Lucia for coordinating this work.

On day 2 of the American Diabetes Association Scientific Sessions, rushing between meetings, I overhead another attendee say this: ‘I’ve never heard so many people talking about diabetes stigma’. I turned to them, a bright smile on my face and said, ‘I know, right?’, (a phrase I only ever utter when I’m in the US).
Just a few hours earlier, Jazz Sethi and I had tweeted simultaneously, setting free an open letter from the diabetes community about diabetes-related stigma. You may have seen it; thousands of people have. And others have shared, commented and even translated it into different languages (I think we’re at 6 translations and counting). Here it is!



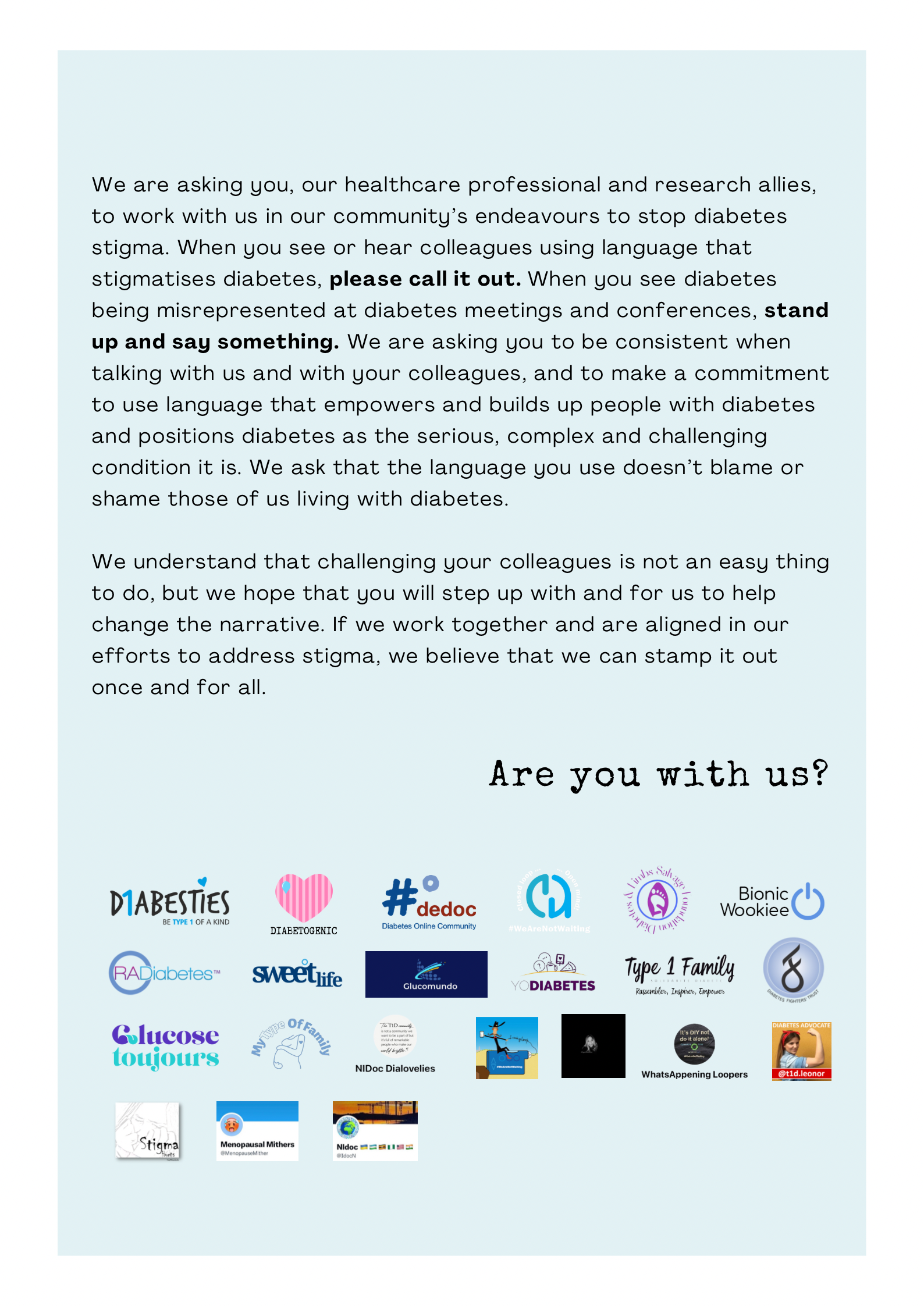
When we first asked advocates from the community if they would like to add their logo to the letter we were surprised by the quick response. Almost everyone we went to said yes. We hadn’t gone out too widely – we wanted to test the waters first. The first version of the open letter includes advocates and peer support groups from across the world. Amazing!
And after our very low-key, (i.e. a couple of tweets from unverified Twitter accounts, so who knows what the algorithm did with them!), we were once again inundated by people asking for us to add their logos. (We haven’t managed to add them yet, but absolutely will in coming weeks. Please give us time if you’ve shared your logo. We’ll get there. And I’ll update this post with the new final page when that happens.)
There is something magic about these sorts of very grassroots, very community, very inclusive initiatives. Not only are they great because they collaboratively offer a narrative from people with diabetes, highlighting an issue that is of great importance to many. They also show you just how powerful and united our community is while also pointing to individuals and groups who are keen to work together, support each other and power the importance of lived experience. And that’s pretty special!
Hey, do you remember a couple of weeks ago when it was International Women’s Day and women got a cupcake (probably baked by a woman) and a breakfast (probably organised by a woman) and then we all agreed that gender equality didn’t need to be spoken about for another year?
Look, I know I sound cynical. But that’s only because I am. Every year at Diabetogenic, I write a post celebrating the incredible women working in diabetes. Mostly I centre diabetes advocates who are generally donating their time – and emotional labour – to power advocacy efforts and make change. And if you look back at the history of the DOC, you will see that the majority of the work has been by women in the community. (Don’t @ me with your ‘But I’m a bloke and I’ve done this’ commentary. It’s not the time for #NotAllMen.)
This year, I started to write something, and then stopped, and started again. And then stopped. Anyone who is a frequent visitor to this site or follows any aspects of my personal advocacy knows that I celebrate the incredible work done by grassroots and community advocates (many/most of whom are women) throughout the year and I didn’t want to buy into the ‘It’s-IWD-here-are-the-womens-now-it’s-back-to-the-misogyny-we-usually-deal-with’ crap that seems to be the aftermath of each and every IWD.
So, I’m using today – this random day – to give a shout out to some of the great things going on that you may have seen, or you may have missed. These things are powered by women who, in most cases, are doing this as extra work on the side of their day jobs, and everything going on in their personal lives. But it’s undeniable that it’s this sort of stuff that is going on all the time, usually flying under the radar, but it’s making a difference to so many folks in the diabetes world.
And so…
There is some remarkable work out of India where the Blue Circle Foundation continues to make a mark in diabetes advocacy. On IWD, a team of women from the Foundation conducted an awareness program for 200 women inmates in Yerwada Jail in Pune, India. This is part of their ongoing Project Gaia which creates safe spaces for women with diabetes. Snehal Nandagawli is just one of the women involved in this work. You can hear more from her at this week’s #dedoc° #docday°.

From the UK, Mel Stephenson-Gray has been a brilliant force in the diabetes community for a number of years. She recently launched a fabulous new Insta page celebrating and empowering women with diabetes. It’s called Diabetes Women’s Health Club and the information she’s been sharing (accompanied by gorgeous graphics) is brilliant. I loved the profiles of some of women who were groundbreaking pioneers in diabetes research. Go give the page a follow now!
Dawn Adams hasn’t managed to convince me that she is only one person because the sheer volume of the work she is doing is immense and she’s bloody everywhere. Dawn continues to blaze trails in her research and writings about diabetes and menopause (follow @MenopauseMither on Twitter for great information and support), has been featured in a number of Diabetes UK publications, spoke at the recent #dedoc° symposium at ATTD, and continues to be a daily support and mentor to people across the global diabetes community. I’ve barely scratched the surface with this list. Someone please send Dawn a coffee and cinnamon bun so she can sit down for 30 seconds and recharge her batteries!
Another woman who is a human powerhouse and obviously works 23 hours a day (lazily, she sleeps for an hour) is Jazz Sethi whose work with the Diabesties Foundation continues to multiply exponentially. She’s also a brilliant speaker and gave an emotional talk at ATTD last month. Check out just some of what she is doing here (and stay tuned for something super exciting that we’ve been working on together!)
Also at the recent ATTD #dedoc° symposium, Hamidah Nabakka from the Sonia Nabeta Foundation captivated the packed-to-capacity room, sharing stories of children and young people living with diabetes in Africa. This was held on the first day of ATTD and for the rest of the week, I had people coming up to me and saying that it was their highlight of the whole conference.
I’m getting to this a little late because it was started last year, but Niki Breslin started a brilliant Insta page to build community called ‘My Type of Family’ for anyone with diabetes who is planning and trying to conceive, pregnant, recently had a baby and parenting. There’s lots of great information and encouragement for the community with this page and definitely worth a follow!

I was so excited to see some artwork by Miss Diabetes from New Zealand make it across the ditch Melbourne in an IWD street art exhibition. Her comic ‘Women and Diabetes’ was on show in our city’s iconic Hosier Lane! Miss Diabetes’ diabetes advocacy is super well-known in the community thanks to her tireless efforts supporting Insulin4All efforts and with work she’s done with the WHO diabetes team. You can see the artwork here.
Anita Sabidi in Indonesia continues to drive and build community with her advocacy work that shine very bright lights on issues such as emotional wellbeing and mental health, and women’s health. Anita is a regular speaker about these important topics, and also leads a number of community initiatives supporting women with diabetes in Indonesia. She’s also speaking at #docday° this week.
Dana Lewis never ceases to amaze. Last week she ran 100kms in a day, but unbelievably, it’s not her physical feats that make her name so well known in the diabetes world. It is, of course, her work in open source AID. Last month she gave two presentations at the Open Diabetes Closing Conference, and she has an upcoming session at the ADA Scientific Sessions in San Diego. On top of that, she continues to publish regularly and is a force for nothing but good!
Ashley Ng from Australia has been documenting life with two gorgeous little girls on her blog, opening up about some of the more difficult aspects of parenting while living with diabetes. I love Ash’s candidness and honesty and am always grateful for her ability to be so raw, but also hopeful. Read and subscribe to her blog here.
These women are just a few of the many who continue to make our community tick and flourish. There work is not only meaningful on 8 March: it’s making a difference every, single day. The very idea that women and their achievements get just one day of real celebration (albeit while battling the calls of ‘where’s International Men’s Day?’) is in equal parts frustrating and insulting. I celebrate the incredible work that women spearhead all the time because I know that alongside that work, they are dealing with patriarchal attitudes that make their successes all the more remarkable. That deserves far more than a cupcake!
Postscript
The UN theme for the day was DigitALL: Innovation and technology for gender equality, not the saccharine sweet ‘EmbraceEquity which means absolutely nothing and was created by some corporate machine that does nothing to advance equality in any way. So, if you spent IWD posting selfies of you hugging yourself, that’s great, but what did that really mean when it comes to advancing gender equality?
If you haven’t had a look at the website from the UN, it’s definitely worth it, even if it’s just to see the high-level details, one of which explains that online gender-based violence silences women and discourages their public participation. It may be odd to think this is a thing in the diabetes community when so much of what you see comes from women, but actually, it’s real. Harassment is a concern for many women, and I know of many women who have stopped sharing or locked down their accounts (permanently or temporarily), or deleted them completely, due to this harassment. I’m one of those women. This is something to be mindful of every day – not just a single day in March.
Like clockwork, the beginning of February heralded a sea of red in every retail store, with cutesy cupid motives and love hearts adorning shop windows. Valentine’s Day was the next big merchandising opportunity and, friends, it’s time to buy up.
At the same time, the diabetes community also starts to be sprinkled with red – this time red roses. Because once again, it’s time for Spare a Rose, Save a Life. It’s the complete opposite of consumer culture. And it’s something that is very close to my heart.
This year marks ten years since Spare a Rose was first launched by a group of diabetes advocates from the US. The story has been told many times but it’s worth repeating, because it says a lot about this community. These advocates wanted to do something that supported others living with diabetes, specifically those in under-resourced counties. And so, Spare a Rose, Save a Child (now Spare a Rose, Save a Life) was created, with a vision to bring together the diabetes community, uniting in the collaborative goal of supporting those who need it.
The simple equation of ‘sparing’ one rose and donating the $5 saving to a diabetes charity was tangible. That face dollars provides insulin for a month. That’s how it has worked for ten years now. Close to one million dollars has been raised in that time, which is truly remarkable when you think about it. It’s people in the community reaching into our pockets to help make a change.
This year, donations are once again going directly to Insulin for Life, a charity that continues to support people with diabetes in countries where there is most need. Insulin for Life has been running for many years and their work is significant. Last year, as war broke out in Ukraine, the charity was able to rally their networks within days, getting critical diabetes supplies where they were most needed. That support continues, and a big part of that is due to the generosity of the diabetes community getting behind Spare a Rose for Ukraine.
As soon as the war started, the diabetes community were desperately looking at how to help and almost immediately, people dug deep. With $400,000 raised in months, so many in the community showed just how committed we are to focusing on others. That’s the diabetes community I know and love!
And so, this year – the tenth anniversary of Spare a Rose – we’re asking again for people to dig deep and help if they can. Leave egos at the door and do the simple thing of supporting community efforts by sharing links, encouraging others to learn about Spare a Rose and, where possible, donate. The only people who benefit from this campaign are people with diabetes who need it. By the community, for the community. Truly the best way to celebrate Valentine’s Day.
Here’s your Spare a Rose, Save a Life refresher for how it works. It’s super easy, and if you click on the image, it will take you directly to the donation page. (Donations are made directly to Insulin for Life.)

Postscript and disclaimer
I have been a community volunteer for the Spare a Rose campaign for a number of years, involved in promotion and communications. I’ve taken a step back this year (for a bucketload of reasons, including this), but am no less involved behind the scenes. I have just started a new job and much of the focus is supporting people with diabetes in low to middle income countries which means I’ll be supporting efforts of many different diabetes charities, including Insulin for Life and Life for a Child (previous charity partner of Spare a Rose), A4D, CDIC and others, as well as the brilliant community groups lead by advocates on the ground.
I’ve been rationing.
I only allow myself one story a day from Kerri’s new book, because I want to rediscover her writing little by little. I skipped over the contents page, so I would to be surprised when I worked out which stories from her Six Until Me blog made it into this new collection.
So it was with delight (and then tears) when I opened up to page 56, three stories into the section called ‘Diabetes in the Wild’ and saw my favourite ever diabetes in the wild story.

Kerri tells this tale beautifully, and exactly as it happened. I know, because I was there. The general gist is that on one her visits to Australia, Kerri and I were sitting outside in the Melbourne sunshine enjoying a coffee. At the next table was a woman and her daughter. When she heard us talking about diabetes, she looked up and joined our conversation, hungry to hear about our diabetes lives, and sharing with us that her daughter had been recently diagnosed. It was only a short chat, but as is often the case with diabetes in the wild stories, it has stayed with me, and I thought about the woman and her daughter each time I walked by that cafe.
Reading the story again in Kerri’s new book, I remembered that day – the perfect blue sky, the frothy tops of our coffees, the way that we were talking a million words a minute as we tend to do when we are together. And I also remembered how five years later I had another chance encounter with the woman from the cafe. ‘You were both so lovely & made me feel so much better,’ she said. ‘I was so glad for your openness and the hope it gave me! I always wanted to tell you that.’
Kerri’s stories are full of the humanity of diabetes. It’s one of the reasons her blog was so popular for the 14 years she wrote it, and why her occasional posts now are so welcome and gratefully received by people in our diabetes community. Her writing is real and generous, and rereading each post is testament to why storytelling is just so damn powerful when it comes to healthcare. I may live on the opposite side of the world to Kerri, exist in an upside down time zone and have to navigate a completely different healthcare system, but there is a familiarity to every single word she writes.
If you’ve never read Kerri’s writing before, this book is the a great place to start. And if you have, the book is a brilliant collection to have on your bookshelf, to pull down every now and then, open at any random page and envelope yourself in her magical storytelling.
And so, Kerri: Congratulations on this book, my darling friend. I remember you once wrote about the friends that live inside your computer. I’m delighted that now, I have you living inside this book and on my rainbow bookshelf. You’ll be alongside the blue spine-d books of Helen Garner, David Sedaris and Jhumper Lahiri – some of my favourite writers. Which is exactly where you belong.
Let’s talk about perimenopause, periods, and diabetes. I’ll just wait a moment while a heap of people log off right now.
.
.
.
.
If you’re still here, hi! Shall we go on?
For the first, I don’t know, maybe 12 years I had my period, I had absolutely no regularity to it at all. I could never understand people who told me they got their period like clockwork, because for me the clock worked intermittently. It was less ‘that time of the month’ and more ‘that time of whenever’. Sometimes it came every three months. Sometimes every four and a half. It was a little surprise that showed up without warting when it felt like it, stayed for a few days, was minimally annoying (never particularly heavy and hardly any cramps at all), and then disappeared again, only to appear when it next felt like it. I spoke with my GP, and they weren’t concerned, and told me to celebrate the fact that I didn’t need to deal with period palaver each and every month.
This was all good and well until I was ready to have a baby. A regular period suggests that ovulation is happening regularly and that is kind of important if you need an egg to be fertilised. That wasn’t happening for me. Some fun fertility treatment (‘fun’, in this instance, means ‘frustrating, lots of tears, desperation and wondering why my body wasn’t doing what it was meant to do’), and I managed to get pregnant and have a baby.
And then, from six months or so after I had our daughter, my periods started happening regularly. Like clockwork. It was as though pregnancy had rebooted the reproductive bits of my body and for the last 18 years, I’ve been paying GST on period products every month.
During this time, I learnt that periods and diabetes don’t play nice. I’ve struggle to find patterns in my cycle so as to run different temp basal rates on my pump to accommodate. Anytime I’ve thought I’d nailed it and settled into a neat routine, the next month everything would go haywire. I guess I settled into another routine: a routine of no routine, where I just had to wing it at whatever time in my cycle things started to look a little sketchy. Loop certainly helped. I could see there were days each month when it was working overtime for no apparent reason, but those days didn’t correspond with the days the previous month. Or subsequent month…
And so, that brings us to present day when it’s time for another life transition or whatever euphemism you want to use to avoid using words that distract attention from hormones, uteruses, blood, and vaginas.
The pretty regular cycles have stopped. I’m not back to three or four (and a half) monthly, it’s more like six weeks or three weeks or some other weird timeframe. My period is on the most bizarre schedule now that is, quite frankly, bloody (yes, I know) annoying. And when it does deign to stop by, it either stays around longer (as in days…) or pops in for just a day or two. Or, even worse, seems to be done after a few days, only to return a day afterwards. Truly, it sucks!
I have made an appointment with my gynaecologist to check-in (it’s probably cervical screening time again) and for a check-up. I know that my experiences are in line with what heaps of other diabetes friends have experienced (yeah, we turn to each other because where else is there to go?), but I have a heap of questions to ask, and accept that there may not be answers.
And I’ve spoken with my endocrinologist. I think that I only ever think of my endo as my ‘diabetes doctor’ but really, her expertise in hormones is pretty bloody useful right now. And the fact that she does some work in a menopause clinic is hugely useful!
But here’s the thing. There are not pages and pages of information out there about diabetes and menstruation or diabetes and menopause. Or how diabetes affects your period during perimenopause. In fact, as with so many things that affect those of us dealing with periods (when they start, when they happen and when they stop), there is a dearth of information and very little research. I mean, it’s no surprise, because the patriarchy in health (as everywhere else) is all powerful. (Don’t believe me? Look at the number of resources about, and treatments for, diabetes and erectile dysfunction as compared with diabetes and menstruation or diabetes and menopause…)
Meanwhile, I just keeping trying to work it out, and speak with friends with diabetes to listen, learn and laugh as they share their stories. And watch as we start to open up more and write more and talk more in our own communities and advocate for more attention. Because that’s the story of diabetes community – we start the conversations that need to be had and that sets off a chain reaction where others get on board. So…get on board!

I recently was invited to run a workshop for health advocates (not just diabetes) who are affiliated with health and community organisations either as employees or volunteers. I was asked to primarily focus on safety in advocacy communities – both online and in person. All participants were women. This was interesting to me because the workshop was open to anyone who was a health advocate – not just women. I could see why, after a few short minutes in, it was women who were keen to come together for this topic and talk about it in a safe space, with other women.
I was delighted to be involved for a couple of reasons: 1. It’s important and 2. I know that when I run a workshop properly, I walk away learning a lot. And this was a topic I wanted to learn about. I set about developing a very vague program that would leave a lot of time for experience sharing and co-developing ideas that could be used by everyone in the room. I had a few discussion starters and things that I think have worked for me, so they formed the basis of the workshop, but most of the suggestions came from the day and with permission, I’m sharing some of the ideas here.
Before I do that, though, I want to highlight the overarching message was that health communities and groups are really important and really valuable. I know I frequently talk about not needing to love everyone in the diabetes community, and how critical it is to find the people you want to be around, who are supportive, who build you up, who you build up and who make you feel safe. That squad becomes sacred. Everyone else spoke of the same thing. One woman mentioned that it had taken her years to find the right people in her health community before truly understanding how peer support can be so beneficial. Many mentioned that it took time to work out exactly what they were looking for – was it friendship, solidarity, advocacy mates, opportunities to grow professionally? There are as many reasons to ‘do’ peer support as peer support models!
But even knowing that, it came as no surprise that every single one of the dozen or so women participating in the workshop had examples of where they had felt unsafe, vulnerable, targeted, or exposed in their own health communities. As stories were shared, there were frequent looks of recognition and heads nodding. Many said it was the first time they had ever spoken about these experiences. And others took time to warm up, asking several times if anyone would know what they had said – worried that they may be identified. This reminded me a little of the Ascensia Women’s Diabetes Social Media Summit I facilitated last year. I’d probably done close to a dozen of those before and each one involved a lot of social media outreach while the event was taking place. But this event was different. This one, was not quite as open. As facilitator, it’s my job to read a room, and the reading I got was that there were a group of women who wanted to share in private. And so, we did. As happened again at this recent workshop.
None of the ideas I’m sharing will identify anyone, and this post has been reviewed by the people who attended. Safety of the women is my primary concern. So, here are some ideas that may or may not be of use to folks out there:
- You are not alone. Feeling unsafe in a community group can feel isolating, especially if there are cliques and groups that seem to form alliances. But there will be others you can turn to – often outside the group. I know I have turned to people outside the diabetes world at times to learn about how they have managed certain circumstances. It’s fascinating just how transferable things can be and how universal others are!
- There are reasons that functions such as block and mute are available on all social media platforms. But go one further. By blocking certain accounts, you may still see people you would prefer to distance yourself from. Mute their name, their account handle and, if they are associated with any specific words, terms or hashtags, mute those too. (So, want to not see my stuff? Block #LanguageMatters and mentions of coffee, stripes, bookstores, baking and red lipstick.)
- Keep records. Even of things that seem irrelevant. I have an online folder where I collate anything that has ever made me feel unsafe or helpless. It’s shared with others, so they know what’s going on.
- Talk to your workplace or associated organisation. This was one of the points that I wanted to raise. As all participants were either employed by, or volunteers for, health organisations, they have access to several services to support them if they feel unsafe. Perhaps they can use the organisation’s EAP which can be a terrifically helpful resource. It’s also important that those records you keep are seen elsewhere and there is a timeline of when things happen, and they are reported in real time. I do this a lot, mostly because it helps to talk to someone. Sometimes it’s done proactively. Other times, it’s after something happens. For example, the first time I spoke about DIYAPS and a slew of HCPs made formal complaints about me daring to talk about something so dangerously off label. Or the time a diabetes educator wrote to my employer after I called them out for tone policing me. There have been the multiple times people in the low carb community have become aggressive and threatening. Or just weird. There have been times when I’ve spoken with the CEO or other senior managers about situations and as well as being great sources of advice and comfort, it also means that they have an idea of how things started and are going. Oh, and it means there are few surprises!
- Walk away – for a bit or a lot. No one is obliged to continue to be involved in advocacy spaces or being part of a community if it is not working or if it is feeling unsafe.
- Go incognito. My name and face have always been associated with the advocacy work I do because that is what I have chosen. But there are times that I wish I’d come up with a nifty pseudonym (Blossom?) and a cute meerkat picture. I know that probably wouldn’t have been possible considering the number of quite public facing things I do means there’s limited anonymity. But there are lots of super effective advocates who are anonymous when doing any online work, and that is absolutely an option. It doesn’t mean that you don’t need to do any media or presentations. It just means not linking the public stuff to your socials. A couple of women at the workshop do that, and I somewhat embarrassingly squealed when I realised that they were amazing anonymous campaigners I’ve learnt so much from over the years!
- Learn the anatomy of gaslighting. It’s an artform, but it’s a predictable one. And expect to be gaslit if anyone ever takes objection to what you do – especially if the source of that objection is from a group that is used to not being challenged. Don’t believe me? I present exhibit a: #AllLivesMatter and exhibit b: #NotAllMen. The term gaslighting was coined to refer to misogynistic abuse and manipulation and it often presents that way these days. Learn how it works and you’ll be astonished at how frequently it is used to disempower women.
- Be prepared for your work to be challenged; to be told you’re not good enough; to be told that you are not worthy; to be told that your work is irrelevant and insignificant; to be criticised for your successes and to be diminished. The first time that happened to me, I was crushed. Now, it’s only mildly soul-destroying. (This isn’t to say that people can’t disagree with your work. Of course, they can, and they will. And that’s perfectly fine. It’s when your work is dismissed and disparaged, and you are personally targeted that it can be especially challenging.)
- Cry. This was my suggestion. I know it sounds ridiculous, but it really helps. I think it just comes from the idea of giving myself permission to not have to be confident all the time and to admit when I am feeling especially vulnerable. When there were weird emails coming to me about fundraising activities, I spent a lot of time bawling.
- Be public about how you are feeling and your experiences. This is a tough one, because it can add being vulnerable onto an already vulnerable situation. But if you are able to assess if it is going to help you get through it, go ahead.
- Ignore it. That sounds naïve considering some of the points I’ve shared, but we all agreed that in some instances, this does work and is the best way forward (albeit with keeping notes).
It is undeniably true that women face a lot of rubbish online and a lot of that is from men. Women who dare to be strident, vocal and stand up and are confident often get it more. We see it everywhere. But I will add that as a straight, white cis woman, I know that the lousy behaviour I’ve experienced is nothing compared to women of colour and people from the LGBTQIA+ community. I’m so grateful to people from those groups who are bravely sharing the horrible attacks they receive and absolutely feel that doing what I can to support them, listen to them and believe them is essential.
The women in the workshop are so committed in their advocacy efforts. It seems unfair that they have had periods where they’ve felt unsafe or targeted. I know how hard it is. Maybe the tips in this post might help others and if they do, great! And if you are reading this and prickling because you object to what you’re seeing, please remember that these experiences are from women who have had a tough time. That doesn’t in any way delegitimise what you have experienced. But I hope that everyone does understand and accept that in living with the patriarchy and with internalised misogyny pretty much part and parcel of everyday life, women do face an unfair share of rubbish, including in advocacy communities.

Psst…forgotten something?
If you’re in the northern hemisphere right now, you’re possibly all caught up in the sunshine, splashing around at the beach or spending time off work just taking time out. If you’re from the southern hemisphere, you’re either smart and have taken a holiday to Europe because EVERYONE.IS.IN.EUROPE.RIGHT.NOW, or under fifteen quilts in front of a roaring fire, counting down the days until it gets warmer. Sadly, I’m in the latter group.
I get it. Things slip by either way.
But! You only have a few days left to make sure you don’t miss out on applying for a #dedoc° voices scholarship. Wherever you are, a scholarship means you have something to look forward to in a couple of months’ time and the absolute thrill of either virtually or in-person attending a global diabetes conference or two. That’s right – TWO! EASD (European diabetes conference) and ISPAD (paediatric diabetes conference) are the next international conferences on the diabetes conference calendar. Both will be hybrid, with the in-person locations being Stockholm and Abu Dhabi respectively.
We’re well over two years into the #dedoc° voices program now, and the awesome thing about it is that it’s not just about the few days of the conference where you get to learn from incredible researchers and clinicians, while waving the lived experience flag and being surrounded by others with diabetes. I mean, that is all pretty great. But being a #dedoc° voice goes way beyond that! Once you receive a scholarship you are part of a network of remarkable diabetes advocates from across the world, and this network is the most supportive, encouraging, brilliant group of people, always ready to help. Every single week, I see people reaching out for support and advice and the responses are swift and many. I’ve not seen a single example of anything other than support, and have watched advocates truly flourish as they have worked with others, developed mentoring relationships and been supported to do brilliant things.
Unless you’re part of the program, you wouldn’t know this. And here’s the deal: anyone can become part of it. The #dedoc° voices program is open to people from across the world and everyone is in with an equal chance. You just need to spend some time completing an application. It is a competitive process, and places are limited. The people who get accepted are the ones who have taken some time with their application and really been able to demonstrate just how they are going to #PayItForward to their diabetes community if successful. No one is a shoe in; having a high follower count on socials means nothing if your application is sub-par. We take people who are new to the diabetes advocacy space, and are looking for a hand carving out their space, as well as seasoned advocates who are keen to work with others and become part of a global network, outside their own country.
So, get on it! Click on the image below, fill in the form and join us! You get to work on your advocacy while giving back to the community, all while wearing the #NothingAboutUsWithoutUs badge. How amazing is that?!

More on #diabetogenic about the #dedoc° voices program:
#dedoc° voices helping people with diabetes get into professional conferences
How #dedoc° voices supported people with diabetes in Ukraine
More on why to apply to join the #dedoc voices program
Disclosure
I have been an advisor for a number of years, and am now working with them as Head of Advocacy.






