
You are currently browsing the category archive for the ‘Mental health’ category.
There are different types of burnout. Diabetes burnout, advocacy burnout, and just plain life burnout.
Diabetes burnout rears its ugly head for many of us living with the condition – sometimes starting as diabetes distress before building and building.
Advocacy burnout seems inevitable the more I discuss it with advocate friends. The living with, working in, supporting others with, diabetes becomes a lot. Too much. So much.
And life burnout seems to be inevitable in the fast-paced, never-pause-for-a-breath, always-switched-on lives we live.
When the three collide it’s a triple threat burnout. Welcome to mine.
The white noise hum of diabetes burnout – always there – slowly, but surely had become amplified. It was little things – I was regularly forgetting to bolus when I ate. Not immediately replacing CGM sensors when one fell off. Ignoring making the follow up diabetes appointments I needed to make, the pathology visit I needed to schedule, the supplies stocktake I needed to do to make sure I didn’t run out of anything.
I’ve been hovering on the edges of advocacy burnout for some time and found myself plunged into it earlier in the year dealing with the complexities that played out as I offered my help and support in some volunteer grassroots advocacy here in Australia.
And life burnout suddenly appeared in the form of exhaustion, but an inability to sleep soundly, and a brain fog that I explained away as a perimenopause symptom. Except it was more than that. It was getting to four in the afternoon before realising I’d not eaten a thing all day. And not remembering if I’d showered, or how many days had passed since I last washed my hair. It was a lethargy that gnawed at me all day long.
I focused on plans for a conference in the US, followed by a few days at work headquarters, knowing that it would be a busy and wonderful time, with a lot of interesting work. I could do it. And I did. The conference was excellent. The diabetes advocates there shone so brightly. And every meeting was a huge success.
Smile. Breath. Smile. Breathe.
Until I couldn’t. That moment hit like a tonne of bricks last week.
I’d spent a day in the office at the job I adore, speaking with incredible people doing so much work. I’m inspired daily by the people I work with and learn so much. There were plans set in motion for exciting things to come and I sat in the meeting room I had set myself up in for the day, feeling satisfied and pleased. The workday done, I packed up and stepped out into the street.
And then, a flash, an instant. Suddenly, the pressure bearing down and around on me was so intense and I felt my chest constrict. I struggled to breathe, and my vision blurred. The sounds on the New York streets suddenly seemed to be coming from under layers of concrete, muffled and hushed and yet piercing at the same time. The bright sunlight seared around me, causing me to shield my eyes from the glare.
‘Breathe. Breathe.’ I felt the rising fright of what I know to be a panic attack, and knew I needed to safely just ride it out. ‘Focus. Focus.’ I looked for something I could hold on to. There it was, a small dog, sitting still, staring dotingly at its human seated at an outdoor café, drinking an iced tea. I stood there, slightly hunched over, my arms wrapped around myself, watching this little dog sitting still. I started to count back from 50, getting to 34 before the dog moved, jumping onto its hindlegs, and resting its front paws on its person’s knee.
It was though the crush from the last few months had all converged. I’d tried in small ways to stem it. I limited my time online, muting more terms and accounts that sought to do nothing but argue and inflame. I welcomed the calmness that descended when my Twitter feed was devoid of people yelling about food choices, and when my Instagram feed only showed me the images of my nearest and dearest. I focused my outside of work advocacy efforts to AID access, specifically on the helpers. I threw myself into my job because it allowed me to focus and celebrate the work of others. I amplified the #dedoc° voices and other advocacy to keep my own away from the spotlight. I thought these things worked.
But at that moment, on the streets of lower Manhattan, those attempts didn’t matter or help. ‘But you seemed fine last week,’ said a friend I’d spent time with at ADA a few days earlier. I had been. I was. I thought about how I appear to others. ‘Sometimes, it’s too much. Right now, it’s too much. Forever… it’s too much.’
I felt the uptick in my heartrate. And realised that had been happening constantly. It had happened after the first difficulty with the grassroots advocacy work, and any time I had to face the source of that stress. Sometimes ‘facing’ meant a comment on a LinkedIn post. Sometimes, it meant a somewhat nasty direct message or, even worse, comments that came to me via others. I realised it had happened every time there was some nastiness or other on Twitter. It happened if there was a confrontation of any time around me, even when I wasn’t involved. Anywhere I saw conflict was enough to kickstart an anxiety response.
‘I’m okay’, I said to my friend. And then, ‘It feels too much.’ I felt myself and my mind and the space around me shatter into a million sharp, craggy pieces. And felt my skin being cut against each and every one of those shards.
This is burnout. This is what it feels like. And with it is anxiety and stress and feeling overwhelmed. We all get it to some degree. Diabetes makes it harder. Diabetes advocacy compounds the whole thing even more. Jet lag doesn’t help. Plus there’s a sprinkling of perimenopause over it all. The culmination is a fragility that scares me a bit and leaves me feeling vulnerable. ‘But you seemed fine…’ my friend had said. And I was. Until the burnout took over. And then I wasn’t anymore.

Just what is the emotional labour associated with living with a life-long health condition like diabetes? I’ve been thinking about it a lot this week, firstly because I was asked to give a talk about it to a group of researchers to help them understand barriers they may experience with getting participants into their research. It was a great discussion, with plenty of questions and hopefully a new understanding of the burden diabetes unleashes on us. And then, I thought about it when I was feeling the weight of that burden – more so than usual.
The emotional labour of living with diabetes is a complex, often invisible force, shaping our lived experience in profound ways. It’s the mental and emotional effort we put into the never-ending demands of the condition. It’s accompanied by an inner dialogue that asks if we’re doing enough, trying enough, feeling enough, being enough. It comes on top of the physical labour of doing diabetes, which in itself, is significant. It’s an ever-accruing emotional toll of being perpetually alert, constant decision making and wondering how those decisions might impact our immediate and long-term health and wellbeing. The emotional resilience required to do diabetes each day is an additional burden of itself, the sum of all these parts equalling an unforgiving weight that, at times, just feels too damn heavy to carry anymore.
But it doesn’t end there. Living with diabetes is an act of advocacy in itself, even if that advocacy is for ourselves alone and whether we use the word or not. Some people who take on advocacy issues and causes, leading efforts, participating in them, speaking about them. Whether involved in advocacy as a paid day job, consulting-type role, voluntarily, or a hybrid version (me), all of it adds to the emotional labour of diabetes.
Of course advocacy can be energising – striving for better healthcare, pushing for more understanding, and campaigning for supportive policies are endeavours close to our hearts and seeing efforts result in stunning outcomes bolster our energy levels. Working together with others with diabetes to change our communities is motivating. But it can also be exhausting. Each act of advocacy draws from our already limited reserves. The constant need to explain, to justify, to fight for our rights and needs can lead to burnout, leaving us feeling drained and disheartened in a fight that seems unending.
That’s where I spent a lot of this week: drained, disheartened, devastated and frequently teary with the weight of advocacy casting a long, dark shadow.
I know that this is something people with diabetes speak about, and the mental health of diabetes is finally on agendas, but it still needs to be said that being adjacent to diabetes, or being a champion for mental healthcare doesn’t offer a true understanding of just what it feels like. The best allies I know are the ones who recognise this gap in understanding and do all they can to ensure they don’t add to it and try to learn by stepping back and not overshadowing our voices or efforts.
One of the ways people with diabetes have attempted to deal with this labour and resulting burnout is to build peer communities and networks. Solace from the weight of diabetes can be found in others with shared experiences in sanctuaries where our struggles don’t need to be explained but they are deeply understood. These are safe spaces where we exchange stories, share tips, and buoy each other’s spirits. These communities become a wellspring of support and encouragement, where our emotional labour is shared, and our advocacy efforts are collectively bolstered. Safeguarding those spaces is essential if we’re to draw strength from them rather than find ourselves being overwhelmed by them.
In recent years, I’ve found myself becoming more and more selective about where I find that support. Twitter was probably the first to be left behind as I no longer found it a safe space. I’m reminded of that any time I venture back an innocent tweet about my own diabetes choices is attacked from some low carb bro. I replaced the openness of social platforms with closed group chats of others with diabetes, knowing that the support was there without the risk of trolling. Those chats provide the light to guide my way through the shadows.
This week, with the heaviness of all that is diabetes weighing me down, it has been difficult to find that light. The networks I have are always there, but even that is sometimes not enough when everything is overwhelming. Hosting this week’s #docday°, and hearing from advocates from around the world doing incredible things wasn’t enough to help me see clear. I thought of how to push through this, and I don’t have an answer. Except this: One of the things we do so well in our community is lift each other up because our community and other people with diabetes are everything. And so, even while I am feeling weighted down, I can focus on that. And hope that in amplifying and cheerleading my peers with diabetes and their efforts, I’ll rise too.
Two community things you should know about…
Spare A Rose, Save a Life is continuing to accept donations here. Thanks to amazing advocate Tinotenda for driving this year’s campaign.
Sign and share this petition and read the consensus statement initiated by a group of #dedoc° voices which is calling for uninterrupted insulin access in humanitarian crises. Congrats to Lucia for coordinating this work.

It’s RUOK? day and while I am ready to jump on any worthwhile bandwagon, this one, today, seems especially important. A (non-diabetes) community of which I am on the periphery is grieving today after the death of a much-loved friend and colleague. I’ve been reading beautiful tributes to this person and messages of love and support to their family. I can’t begin to grasp what their loved ones are going through today.
RUOK? is more than a single day. It’s a movement that emphasises the power of human and social connection and having conversations about difficult things. If you’ve not looked at the website, there is advice about building the capacity of support networks (the very foundations of diabetes peer support groups for decades now) and developing skills to have meaningful discussions with someone who might be struggling.
It’s applicable to everyone, including those who may appear to not necessarily need it. Undeniably, it’s very relevant to diabetes. (This article outlines the increased risk of suicide in people with diabetes.)
Diabetes and mental health may be a topic on the agenda at most conferences and we’ve certainly seen an uptick in mental health and diabetes research over the last decade. But the strides that have been made are not enough. The pathway to genuine support and treatment for people with diabetes remains elusive. Simply telling people to seek help falls short when the help they need is not available.
Our peer networks go a long way to offering support, empathy, and love, but we’re not equipped to handle complex mental health issues. While we can assure people that they are not alone and perhaps offer suggestions for where they may find help, this does not go far enough in addressing mental health care, especially in critical situations. Accessing mental health professionals that have knowledge and training to support people with diabetes is what is needed. And it needs to be easily accessible. Easily affordable. Easily available. Right now, that’s not the case.
On RUOK? Day implores us to tap into our social circles and genuinely check in. (Do it, please; just do it). But there is a braider landscape of mental health in the diabetes landscape that needs real transformation. And while it seems unreasonable to add extra burden to those of us living with diabetes – after all, we are already expected to do so much of the physical, emotional, social, and political labour just to get by – community action drives change so often. We have had successful and coordinated community efforts to increase technology funding and access. Is our next frontier turning our attention to increasing funding and access to mental health care for people with diabetes? I know that some diabetes organisations have this in their sights, but without people with diabetes making noise, the campaign is only half-baked. Our voices amplify the urgency of the issue.
Today is just one day, but if RUOK? Day is what provides the gentle nudge to initiate these conversations, it’s a step forward. The tapestry of personal narratives, community connections and shared experiences form the basis of peer support. But not everyone has a safe space where they can share or the people to share with. Sometimes we need to reach out, extend a hand and signal we’re ready to listen. Keep reaching out. Today. And tomorrow. Every time you can.

It’s World Mental Health Day and that seems as a good as any a day to speak about diabetes and mental health. Actually, every day is a good day for that, but with every health organisation’s social media manager’s attention turned to today’s health promotion day, I’m jumping on that bandwagon and adding this post to the myriad on Diabetogenic that address the very significant issue of diabetes and mental health.
I don’t think it’s fair to say that we don’t speak about diabetes and mental health these days. We do. As is so often the case, the conversations started in the community, led by people with diabetes and then were slowly, but surely picked up by other stakeholders. Many health professionals are tuned into mental healthcare being part of diabetes care. And in recent years, diabetes organisations have followed the lead of the community by running public health campaigns aimed at raising awareness of diabetes and mental health. Thanks to peer-reviewed research, we have evidence to show that diabetes impacts mental health and that mental health impacts diabetes.
But even if we say confidently say that diabetes mental health is on the agenda, there is still good reason to believe that more light be shed on the topic, and more attention be given to it. And to really advocate for mental health care to be seen as part and parcel of diabetes care. I really do believe that would make a huge difference.
When we talk mental health in diabetes, there’s a lot to consider. Of course, there are the diabetes-specific things like diabetes burnout and diabetes distress. Plus, eating disorders can take on a particularly diabetes-focus with conditions such as diabulimia (which really, really needs to be listed in the Diagnostic and Statistical Manual of Mental Disorders – it’s such a difficult, under-researched, misunderstood, yet very present reality for so many people living with diabetes).
But there are also ‘every day’ mental health conditions that are increased when someone lives with diabetes, such as depression and anxiety. Just how much of that is linked to diabetes?
And for those of us who dabble in the advocacy world, there is advocacy-related burnout to contend with too and that can and does start to impact our own diabetes management and mental health.
I couldn’t even try to estimate the number of times I’ve given talks about diabetes and mental health from a lived experience perspective. But I am always happy to be asked, and always willing to talk about it, even if it means being quite vulnerable and exposed when I do so.
I remember when my work in diabetes organisations started to focus more on mental health, and I also remember when those discussions were accompanied by a change in narrative. Suddenly, a lot of what we spoke about – from diabetes-related complications to risk reduction – came with a side serve of mental health commentary. It helped to show the undeniable link between the two. And the community responded to that favourably.
Diabetes has never just been about glucose levels, or carbohydrates. And there are healthcare professionals and researchers and organisation leaders that understand that – probably because they have spent time really listening to people with diabetes, rather than just churning out the old tropes about the ticking time bomb of diabetes. Actually, those tropes have probably contributed to a lot of diabetes-related distress.
Starting conversations about diabetes and mental health can be difficult. I like to think that all HCPs these days are aware of the intersection between diabetes care and mental health care, but sadly, I don’t think that is necessarily the case. If the stories I frequently see on social media are anything to go by, there is still a way to go when it comes to having frank, open, honest discussions that recognise that the mental health of people with diabetes needs attention.
These days, I know that my mental health is really not that great. While I know that may seem alarming, I actually see it as progress. Being able to identify that I am feeling this way means I can do something about it. In years gone by, I had no awareness about my mental state. I didn’t know what to do about it.
When I talk about how my mental health is faring – especially when feeling as I do now – there is often surprise. I am not backwards in coming forwards and I know that many people see me as confident, assertive, and self-assured. And I am that way. I’m also pretty bubbly and positive about life in general. But with it comes some dark times and dark thoughts and dark days that are really not especially easy to manage.
I don’t know about others, but when things are dark, everything seems bigger and scarier. I had a low the other night that hit below 2.0mmol/l, and ordinarily I’d deal with it and move on. But during the hypo and since then I’ve not been able to stop thinking about it and worrying about it. It never pays to play ‘what if’ in diabetes, and yet most of my thoughts when remembering the other night have started that way. The constant crap that I’ve been dealing with in the advocacy space for far too long now feels unbearable, and seems so, so nasty that I feel a wave of anxiety just being online. The burden of simply doing diabetes feels massive. The other day, I cried when my insulin pump demanded a battery change. And I can’t shake this overwhelming feeling that I have no idea what I am doing with my own diabetes management and am so anxious about complications, even though there is no good reason for it. These are the dark feelings. The reason sleep gets disturbed. The reason that my heart beats faster.
If I could wave a wand and make one thing come true this World Mental Health Day, it would be that everyone with diabetes has access to mental health care as part of routine diabetes care. And if I could wave that wand for a second time, I’d want my own mental health to build back up and become a little more robust than it is right now. That would be really, really great.
C/W This post contains content about diabetes and suicide and intended self-injury.
If you need help, this Wikipedia page has a list of mental health crisis lines around the world. And for a list of contacts actively updated and maintained by the Wikimedia Foundation, go here.
We talk a lot about taboo topics in diabetes. For years, there have been concerted efforts to shine a light on many of the issues and topics that have not received enough attention but are very important to people with diabetes. Often it is people in the diabetes community who find ways to delicately begin conversations, and that is then followed by an interest from researchers and clinicians.
But there are still some topics that are often seen as just too difficult, just too fraught, just too scary.
Suicide and intended self-injury (ISI) fall into that group.
At EASD this year, I was invited to join a meeting for the RESCUE Collaborative Community, a project that is lifting the veil on one of the most difficult issues in diabetes mental health. The name of this project is a clue to what it is trying to achieve: RESCUE (REducing SuiCide rates amongst individUals with diabetes).
The mission of this project is:
To reduce rates of intended self-injury (ISI) and suicidal acts by people with diabetes through improved understanding of the risk factors and implementing strategies to address them. In support of this mission, RESCUE works with stakeholders across the health spectrum including patients and care partners, academia, healthcare professionals, advocacy groups, industry, payers, federal and state agencies and regulatory bodies.
This is a big issue and a difficult one. There is a lot to think about, a lot of unknowns and a lot of questions to be asked. To work out how to help people with diabetes who are at risk, there needs to be a better informed workforce, with evidence to develop strategies that are going to help. And we also need to know how to approach the very basics when talking about suicide and ISI in relation to diabetes.
When it comes to diabetes and mental health something comes up frequently: there is limited dialogue and understanding between diabetes HCPs and mental health HCPs. I remember hearing Georgie Peters speak at the IDF World Diabetes Congress in 2017 about living with diabulimia. She said that she would be told to ‘go home and take your insulin’ – a completely inadequate approach. In her talk, Georgie said that is the same as telling someone with anorexia to ‘go home and eat’. But when trying to navigate care from two highly specialised health areas, that sort of response is rife.
And so, how to we make sure that when looking at diabetes and suicide and ISI, we are mindful of the specific diabetes issues that need to be considered?
At the meeting last week, we spoke about trying to identify people with diabetes who may need attention. Contemplating how insulin may be used as a way to self-harm is one consideration, so people being admitted to hospital with frequent DKA, and people admitted for a serious hypo could be a starting point to investigate. Of course, not everyone who has DKA or a serious hypo is self-harming. Diabetes gonna diabetes and sometimes, things just happen. But it certainly does seem a good place to begin, with targeted approaches to ask questions in an appropriate way that might help identify people who need mental health support, in particular about ISI and suicide, with an aim of reducing risks.
One of the other discussion points was asking about the role of peer support and the community when talking about suicide and diabetes? Is peer mentorship an idea? How can peers support each other? In the way that #TalkAboutComplications kickstarted meaningful community discussions about the taboo topic of diabetes-related complications and helped people with diabetes feel safe to first open up and speak about their own experiences of living with diabetes-related complications, could there be a way to signpost discussions about serious mental health conditions. And would this break down stigmas, help people realise they are not alone, and seek help, or at least ask where to seek help? Or, is this a burden too big for peer support?
There’s a lot to unpack here, and there really are no simple answers. But this work spearheaded by Professor Kath Barnard-Kelly with a team of dynamic health professionals, with input from diabetes advocates is lifting a veil to start to look for those answers.
MORE
#dedoc° voice, the brilliant Niki (@WhatNikiDidNext) live tweeted a symposium on suicide and ISI at EASD, and you can see her tweets here. Presenters at this session were Kath Barnard-Kelly, Marissa Town, Tadej Battelino and Simon O’Neil.
Disclosure
My travel and accommodation were covered by #dedoc°, where I am employed as Head of Advocacy. Thanks to EASD for the press pass.
I was invited to attend the RESCUE Collaborative Community meeting. I was not paid for my time to attend.
Stress impacts diabetes in different ways. And of course, everyone’s response is going to be different.
Before Loop (which now feels like almost a lifetime ago), the effect of stress on my glucose levels was tricky and unpredictable. At times, it would make me high. Other times, I’d be in Hypotown (the town no one wants to visit) for hours, without any respite. The clever Loop algorithm tidies most of that up for me these days.
But when it comes to diabetes, stress doesn’t only impact what I see on my CGM trace. It’s far more than that. Loop can only do so much… Insulin automation doesn’t mean diabetes automation. And it certainly doesn’t mean life automation.
Let me talk about how it’s affected things in the last couple of months …
To some, it might look as though I have become lazy about my diabetes management. I have run out of insulin in my pump more times than I care to admit, scrambling to find my spares bag to refill the canula. I ignore the alerts, silencing alarms and putting the task that needs to be done out of mind.
I’ve let the batteries on my pump and RileyLink wear almost right down. In fact, the batteries have got to the point where they are so crucially low Loop has stopped working. Even the Red Loop Of Doom on my Loop app hasn’t been enough to swing me into action.
I’ve almost run out of insulin. I never do this. Ever. I have a system that works for ordering new scripts to make sure that there is always at least two weeks’ supply, and then back up plans for my back up plans. And yet, there I was, staring down the last few drops of insulin in a penfill. I don’t use insulin pens. I use vials. But I’d run out of vials and was using a penfill that I have for absolute emergencies.
This had become an emergency.
Same goes for pump consumables. I was reduced to searching the depths of my diabetes cupboard and discarded handbags looking for an infusion set, desperately hoping that there was at least one, somewhere, that would do the trick before I had to knock on the door of my neighbour, asking her to tide me over.
This is one part of diabetes burnout for me – the way that I deal with my diabetes tasks. It’s not feelings of resentment that I must do those tasks; it’s not feeling distressed that I must do them. It’s not even feeling a paralysis about doing them. It’s simply not caring enough about them to take the time and energy to engage my brain and actually do it.
I know that when I am stressed, something’s gotta give, and for me, that’s always been doing diabetes.
I cannot tell you how much having automated insulin delivery sweeps up a lot of it. Forgotten boluses get sorted by Loop. Sure, it may take a little extra time and mean a bit of extra time above my upper range limit, but if I don’t engage, Loop will bring me back in range soon enough.
The low-grade nausea I’ve been living with for the last month means that eating is sometimes difficult, but I don’t even need to think about what that means for glucose levels, because Loop mostly does it for me.
And sleep! Sleep the gift that Loop keeps giving has been interrupted, not by diabetes, but by waking stressed. Or, as has happened twice in the last week, with a splitting headache, so painful that the throbbing has woken me from a deep sleep. Pre-Loop, sleep disturbances would wreak havoc with my glucose levels (often because most of the time those disturbances were because of my glucose levels). But now, as I see the upward spike start because I’ve been woken in the middle of the night and glucose is being dumped because apparently, I’m now up and awake, Loop kicks in with an ‘I don’t think so’, and that spike is shut down quickly.
But the nausea is debilitating physically. And being woken in the middle of the night is exhausting. And the stress is leaving me feel a little hopeless all around, to be honest. Teary, emotional, tired. And burnt out.
Many years ago, after a couple of periods of intense burnout, I did a smart thing and found a psychologist to help me. Together, we learnt to identify the triggers that precipitated burnout. This has truly become one of the most powerful tools in my diabetes emotional wellbeing arsenal, because learning when I am heading down the slippery slope of burnout, and realising it’s coming, has meant that I’ve been able to address it before I get so deep into that dark space, it becomes challenging to come back from.
So, right now, I know this is happening. I can feel the stress and the physical manifestation of it, and I can see how it is influencing my diabetes. Today, I spoke with my psychologist – in a way waving a white flag of surrender knowing that I need someone else to come in and help me through this, because I can’t do it myself.
The win is that I’ve seen it and I’ve recognised it. The win is I’m seeking help. The win is that I’ve caught it before I’m plunging to dark depths (I hope).
It’s not a win that I’m feeling this way. It’s not a win that this level of stress has started to affect so much, including my diabetes. It’s definitely not a win that I’ve reached the point where I’m staring down the path to diabetes burnout despite the reason being un-diabetes-related stress.
But that’s how it goes. Diabetes becomes part of it. Of course it does. Because diabetes is always part of it. Always part of everything. Always hand in hand with whatever else is going on. Stress and diabetes leading to burnout. One of the few equations in diabetes that I can count on.
(Click to be taken to Instagram for details.)
Friends, how’s your mental health today. Mine. Is. Shit.
Gosh, I feel as though I have been through the wringer, hung out to dry and then, just at the moment that everything was looking good again, dropped in a muddy puddle and trampled on by a herd of bison. I mean, not really, because bison are not typically found in the especially hipster part of downtown Melbourne I reside, but hopefully you now have a picture of how I’m feeling.
Not even the overabundance of sparkly necklaces (and ever-present red lipstick) I threw on this morning can distract from the fact that I am exhausted, look as though I’ve been weepy for most of the day (because I have) and am just feeling so damn over everything right now.

Somehow, I held it together for a live Q&A about diabetes and mental health which I may or may not have treated as my own personal therapy session. (You can watch the video here.) Thankfully, psychologist, the ever-wonderful Dr Adriana Ventura, offered some fabulous tips for how to take care of our mental health during this time that is still being referred to as unprecedented times, but I’ve taken to calling the clusterfuck period.
The moment today that was the most difficult for me to deal with was just after 11am when the NSW Premier told us the grim news out of her state. I know that I probably should stop watching the pressers, especially the ones out of NSW. It’s not my state, so most of what is being said is actually not all that relevant to me and my family, and the repeated lies that are casually thrown around like confetti at weddings we can’t have anymore make me furious. And yet, even knowing that, I find myself sitting through them most days, yelling at the screen while madly tweeting my fury.
But today, instead of yelling, there was crying. The NSW Premier said ‘We extend our condolences to the family of a man who has died. He had received one vaccination. And he DID have underlying health conditions.’ She accentuated the word ‘did’ to underline what she was saying.
And so, where back, or perhaps still, at this point. That point is where we dismiss those with health conditions as nothing more than covid collateral.
I cried as she said it, angrily wiping away tears at how easily I was once again being made to feel expendable. I felt sad and broken and just so damn beaten. I have spent the last twenty months doing all I can to protect myself, knowing full well that those efforts protect others too. I rarely go out; I never leave the house without a mask; I’ve washed my hands and rubbed so much sanitiser into my skin that I feel the dermatitis that has started will never leave; I’ve followed all restrictions; when I do go anywhere, I check in at each location; I’ve had a covid test every time I so much as feel sniffly; and I got vaccinated the second I was eligible.
I have been deliberately compliant when it comes to covid.
And when it comes to diabetes, my deliberate non-compliance has meant that I am continuing to manage in a way that, according to every HCP and researcher I’ve ever met, is giving me the best chance to live well and to live long with diabetes.
And yet, despite all that, if I get covid and die, the message is it’s because I had an underlying condition. I already have one foot in the grave; covid just gave me a gentle push the rest of the way.
Well, fuck that.
I know I’ve written about this before, and honestly, this far into it all, I should be better at just ignoring it. But when it is coming from our politicians and the media, and I’m hearing it from people in the community, it’s hard to not take it personally.
The man the NSW Premier referred to, died from covid, not his pre-existing health condition. It certainly may have meant that covid was complicated for him, but if he’d not got covid in the first place, he probably would still be alive. His underlying medical condition doesn’t make him any less worthy, or any less of a loss. It doesn’t excuse his death.
I don’t know when people will stop with this hurtful and harmful rhetoric. I’d have hoped that by now the communication efforts from those who stand up every day to tell us the bad covid news would be more nuanced and more respectful.
I guess that’s too much to hope for.
A week out from National Diabetes Week, and this piece has been sitting in my ‘to be published’ folder, just waiting. But the post-NDW exhaustion coupled with lockdown exhaustion, plus wanting to make sure that all my thoughts are lined up have meant that I haven’t hit the go button.
In the lead up to NDW I wrote this piece for the Diabetes Australia website. That piece was a mea culpa, acknowledging my own contribution to diabetes-related stigma and owning it. I also stand by my thoughts that the stigma from within the community is very real and does happen.
But what I didn’t address is just where that stigma comes from. Those biases that many people with type 1 diabetes (and those directly affected by it) have towards type 2 diabetes come from somewhere, and in a lot of cases that is the same place where the general community’s bias about diabetes comes from. It is all very well for us to expect people with type 1 diabetes to do better, but I’m not sure that is necessarily fair. I think that we should have the same expectations of everyone when it comes to stamping out stigma.
And so, to the source of stigma and, as I’ve said before, it comes from lots of places. As someone who has spent the last twenty years working in diabetes organisations, I know that the messaging my orgs like (and including) those that have paid my weekly salary has been problematic. I still am haunted by the ‘scary’ campaign from a few years ago that involved spiders, clowns, and sharks. (If you don’t remember that campaign, good. If you do, therapy works.)
For me personally, I don’t think much stigma I have faced has come at the hands of other PWD. Sure, there’s the low carb nutters who seem to have featured far too frequently on my stigma radar, however, the most common source of stigma has undoubtedly been HCPs.
It’s not just me who has had this experience. The majority of what I have seen online as a response to experiences about stigma involves heartbreaking tales of PWDs’ encounters with their HCPs.
While I will call out nastiness at every corner, and no stigma is good stigma, it must be said that there is a particular harm that comes when the origin of the stigma is the very people charged to help us. Walking into a health professional appointment feeling overwhelmed, scared, and frustrated only to leave still feeling those things, but with added judgement, shame and guilt is detrimental to any endeavours to live well with diabetes. In fact, the most likely outcome of repeated, or even singular, experiences like that is to simply not go back. And who could criticise that reaction, really? Why would anyone continually put themselves in a situation where they feel that way? I wouldn’t. I know that because I didn’t.
It’s one thing to see a crappy joke from a comedian who thinks they’re being brilliantly original (they never are) or the mundane, and almost expected, ‘diabetes on a plate’ throwaway line in a cooking show, but while these incidents can be damaging, they are very different to having stigmatising comments and behaviours directed at an individual as is often the case when it is from a HCP.
Of course, HCPs aren’t immune to the bias that forms negative ideas and opinions about diabetes. In the same way that people with type 1 diabetes form these biases because those misconceptions are prevalent in the community, HCPs see them too. Remember this slide that I shared from a conference presentation?
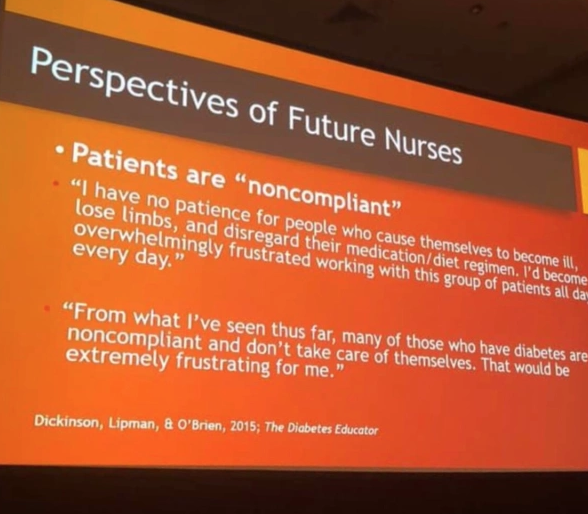
This came from student nurses. Just think about that. Students who were training to be HCPs who would inevitably be working with people with diabetes. A I wrote at the time:
‘They hadn’t even set foot on the wards yet as qualified HCPs. But somehow, their perceptions of people with diabetes were already negative, and so full of bias. Already, they have a seed planted that is going to grow into a huge tree of blaming and shaming. And the people they are trusted to help will be made to feel at fault and as though they deserve whatever comes their way.’
Is it any wonder that, with these attitudes seemingly welded on, that people with diabetes are experience stigma at the hands of their HCPs?
The impetus can’t only be on PWD to call this out. And the calls to fix stigma can’t exclusively rest on the shoulders of PWD – we already have a lot of weight there! It must come from HCPs as well – especially as there is such a problem with this group. Perhaps the first step is to see real acknowledgement from this group of their role here – a mea culpa from professional bodies and individuals alike. Recognising that no one is immune to the bias is a good step. Owning that bias is another. And then doing something about it – something meaningful – is how we make things better for people with diabetes. I really hope we see that happening.
More about this:
Becoming an ally – how HCPs can show they’re really on our side.
Ask a group of people with diabetes about their experiences of stigma, and for examples of the sorts of things they’ve heard and before long you’ll be able to compile a top ten list of the most commonly heard misconceptions that have contributed to diabetes having an image problem. When I’ve asked about this recently, the main perpetrators of these seemed to be healthcare professionals. More on that later this week.
This year, in the Diabetes Australia National Diabetes Week campaign about diabetes-related stigma, two videos have been produced and they’re almost like a highlight reel of some of the stigmatising things people with diabetes hear.
Let me tell you something I found really interesting. As part of the testing of these, I showed them to a heap of people with diabetes and a heap of people without diabetes. The reaction from people with diabetes varied from sadness (including tears), to anger and frustration, and mostly, recognition in everything they saw.
The reaction from a number of people without diabetes was disbelief that this really happens. They simply couldn’t believe that people would be so insensitive; so cruel, so shaming.
However, for so many people with diabetes, this is our reality.
Here’s one of the two videos we produced. (You can watch the second one here.) Already, this is being shared widely in our own diabetes community. I’ve lost count of the places online I’ve seen this shared. Keep doing so, if you can. Because clearly, we need to get the message out to those without diabetes so they understand that not only is this sort of stigmatising behaviour harmful, but it is also horribly common. And it needs to stop.
DISCLOSURE
I work for Diabetes Australia, and I have been involved in the development of the Heads Up on Diabetes campaign. I’ve not been asked to share this – doing so of my volition, because I think the messaging is spot on. The words here are my own, and have not been reviewed prior to publication.
There is so much about diabetes that can’t be simply explained or managed. And even if we understand the mechanism behind why something happens, we can’t necessarily fix it!
The intersection between diabetes and anxiety is certainly one of those things. When I am anxious, I go high. That’s the way it is. If I am extremely anxious and have a panic attack, the adrenalin rush sends me to insanely high glucose levels that I know I can’t treat by just bolusing insulin, because there will a swift, aggressive crash at some point and any excess insulin will make it worse. Much worse, because nausea often accompanies how I am feeling in the moment, so the thought of an ‘eat-the-kitchen’ hypo is not great at all.
I was feeling pretty anxious yesterday. It was a medium level hum that at times swelled to a loud banging noise, and I could sense that there was a topple on effect with my glucose levels. Except there wasn’t. At least not one that could be detected on my CGM graph, which was chugging along in range, albeit at the slightly higher end of that range.
But Loop was working hard to keep it that way. Micro changes to basal insulin showed a Loop graph of constantly changing dosing throughout the morning – at the same time I was feeling loud-banging-noise-anxious. At the moment there was a surge in anxiety levels – and I can pinpoint that moment – there was an accompanying surge in my insulin dose, but only for a little while. Because as my anxiety ebbed and flowed, so did my insulin dosing. All with me doing nothing.
Living with anxiety is one of the things that makes diabetes super difficult. I mean, there are so many things, but anxiety is a next level issue because the very idea of thinking about dealing with diabetes while dealing with an intense moment of anxiety is, quite simply, impossible. But even if I could, there is no way that I would be able to predict just how my glucose levels would respond, or the timing of that response, to act effectively.
As ever when writing and thinking about automated insulin delivery it comes with a very honest understanding, and acknowledgement of my privilege and knowing that I am extraordinarily fortunate to have at my disposal the technology that can help me in this way. I’ve written and spoken about this a number of times, and I am always acutely aware of the advantage of having a system that takes away so much of the brain power needed to manage such a complex health condition. I say this not as an afterthought – it is an ever-present thought.
But also ever-present is the gratitude that there is something with me that is providing such incredible insight into just how my diabetes behaves, operates and reacts to different situations. That is, of course, what CGM does. But it’s Loop gives an extra layer of insight – it shows me what my body would have been doing if my beta cells hadn’t gone on a permanent ‘tools down’ almost twenty-three years ago. And gives me an appreciation, and a reminder, of just how difficult diabetes is, and how incredibly challenging it is to attempt to perform the function of a highly sophisticated and evolved body organ!
Anxiety is unpleasant. What it does to diabetes is unpleasant. But having the tools to help manage its impacts on diabetes does help. It’s one less thing to worry about at a moment when it feels that I am being engulfed in a whole world of darkness and worry which is how I felt yesterday.
Now if someone could just magic up a DIY tool to stop the anxiety happening in the first place, that would be just dandy!







