I have a diabetes friend called Andrea. She lives in France and I’ve known her for close to 15 years now. She once told me a hack that she thought Podders should know. I didn’t heed her advice and should have. So, in the spirit of #PayItForward (RIP, Bastian), I’m sharing it here.
Every pod user will be familiar with the pod scream of death. Maybe you have never experienced it yourself, but I expect you will have been told of all the impossibly inappropriate places a pod decides to play the music of its people.
Hopefully, it will be a rare occurrence, but there’s no mistaking the high-pitched scream that emits from a device that usually makes no other noise than a gentle, reassuring clicking sound when delivering insulin.
For me, it inevitably happens when the eight-hour grace period has lapsed and I’ve ignored all the countdown warnings. Be better than me. Don’t do that.
Silencing the piercing alarm is usually easily remedied. A sharp needle shoved into a small hole on the back of the pod usually does the trick. There’s something magical about the peace that prevails after the screaming stops.
The other day, I was working in my office at home, and was startled by the high-frequency shriek. I looked up from my computer screen and started counting hours backwards. Why was the bloody thing screaming at me? I’d changed it only the evening before. I glanced at my phone which showed a beautiful green loop, and tilted my ear towards the pod on my right arm that seemed happily doing its pod thing. It certainly wasn’t shouting at me.
I stood up, looking around for the source of the noise. The banshee wail was coming from the cardboard box on a shelf in my office – the box where my pods rest before being sent off for recycling. (Podders – you do all know about the recycling programme, right?)
I pulled the box down and looked inside. There were about 25 spent pods in there, and one of them was not happy. I worked my way through them, until I found the offending noise maker, and shoved a needle into its back.
I then looked suspiciously at the others in the box and realised that any of them could start screeching at any moment. What if they were influenced by the non-compliant noisy one? What if they decided to do the same thing at 3am? I dumped each of the pods onto my desk and stabbed the lot of them .
And while doing so, I remembered my clever friend Andrea telling me that she always disables the old pod when she’s doing a change. For this exact reason. ‘Smart,’ I thought. ‘I’m going to do that, too.’
Reader, I did not do that, too. I waited until an old pod threw a tantrum because it didn’t like being in the box with other pods and decided to share its big feelings.
In the spirit of sharing diabetes hacks, I am passing on Andrea’s smart advice: disable your pods before you pop them in the recycling box. Do it once you’ve filled up your next pod and you have a sharp needle right there to do it. Make it part of your pod changing process. Don’t leave it until you are frantically trying to silence the little sucker. Future you will thank you. That’s what I’m doing now.
And this is just another reminder of how the most important things we learn are from our friends with diabetes who know all the tips and tricks to make diabetes that tiny bit easier to manage.
Exciting news for friends attending the IDF Western Pacific Region Congress in Melbourne later this month. New York artist Appleton will be here and I can wait to see how he decorates our beautiful city. Here is some of his work in Jaipur earlier this year.
I’ve been in India this week for the annual Udaipur T1D Summit. This year, we took the summit to Jodhpur and once again, brought together dozens of people with diabetes, clinicians, researchers, industry stakeholders and policy makers.
Jyotsana, Lakshmi, Mridula and Nupur, and me chairing the community panel.
One day, we all travelled to Nagaur, a city about three hours out of Jodhpur. We visited a T1D clinic in a district hospital, and attended a day camp for children and adolescents with T1D and their parents. This was for me, undoubtedly, the highlight of this visit to India.
The vast majority of the discussions were in Hindi and the local language. I understood nothing of the presentations other than the occasional words in English that cropped up from time to time. Afterwards, many of the people in the room spoke with me in English, and I had some lovely conversations with children and teens with diabetes, and their parents. I spoke with two young girls and they told me what they liked doing, about school and what annoys them about diabetes. A tiny toddler sat next to me and she was far more interested in the beaded bracelets on my arm than diabetes and really, who can blame her? Diabetes doesn’t compare to bright friendship bracelets! And I spoke with a remarkable young woman who I truly believe is going to change the world. She told me she wants to be a polo player, and I have no doubt that at some point I will find out that she is competing on national and international stages. She told me about how she feels about living with diabetes and her optimism and hope have stayed with me for the last few days. If only every newly diagnosed child with diabetes could connect with someone like her!
Parents spoke with each other, always keeping an eye on their children, but secure in the knowledge that in this room, everyone was looking out for each other.
I watched advocates who have become friends lead the activities, and I was in awe as they managed to show just how much peer support can mean. Jyotsana needs her own TV show – her enthusiasm and spark as she rallied the children was infectious. And Nupur and Snehal, ever calm and grounded, know exactly when to step in and when to step back. And then Prashanth rallied the children to do their injections together before they ate lunch, watching over each of them, and offering words of encouragement and words of reassurance. Worlds frequently collide in the diabetes advocacy space, and these incredible advocates are also #dedoc° voices. They are as confident and comfortable standing on stages at international professional diabetes conferences and in front of community groups. This is community at its best and most powerful.
Prashanth, Nupur, Snehal and Jyotsana rallying the enthusiastic crowd.
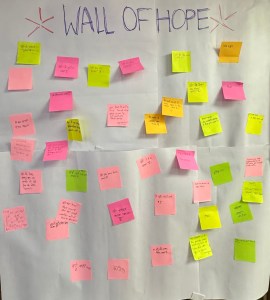
One of the activities during the day is a ‘Wall of Hope’. I asked one of the event organisers translate the words on the post it notes. It came as no surprise to me that in the wishes and hopes and dreams of these young people, diabetes didn’t feature. They wrote about wanting to be doctors and teachers and work for the government. Many wrote about wanting to have happy lives. One said ‘I want to be strong like my mother and then I want to be a doctor’. I got a bit wobbly with that one!
There are some universal truths about T1D. I’ve come to learn that after decades of working in the diabetes space and spending time with others with diabetes. We are all different and we all carry diabetes in different ways. Our experiences vary based on diverse, complex and multiple factors. There absolutely is no one size fits all for diabetes.
But there is one constant that I have seen and continue to see ant that is the power of peer support. Spending time with others living with diabetes is life changing. The shared language of diabetes connects people in ways that make sense only to those of walking our own diabetes path.
One of the organisers of the event told me that me being there was important for the families and for the kids with diabetes. She looked surprised when I told her that it was important for me to see them. I learn from each and every other person with diabetes I come across and feel energised and connected. We all leave with out batteries recharged from the energy in the room.
Living with diabetes was never meant to be a solitary endeavour. It makes it so much easier when we have others who ‘get it’ because they’re living it too. That’s the superpower of community.
Disclosure
The Udaipur T1D Summit is a collaboration between Friends of Mewar (a charity run by Princess Padmaja Kumari Parmar who lives with T1D), the William J Clinton Foundation and Breakthrough T1D. I work at Breakthrough T1D as Senior Director, Global Responsibility.
For the last 25 and a half years, I’ve used an insulin pump to keep me alive. I’ve been using CGM almost full time since 2013, and sporadically before that.
Today, newspapers across Australia have published a fear-mongering report dressed up as serious investigative journalism about the safety of diabetes technologies and devices.
This is why we can’t have nice things.
Let me start by clarifying a couple of things. Firstly, the stories quoted from a few people with diabetes who have had genuinely frightening experiences with their technology should not be minimised. I understand how terrifying they may have felt when the devices they relied on didn’t behave as expected. And now they have made them question the safety of their devices.
And, secondly, I am fully aware of the shortcomings of diabetes tech. Of course I am. I’d be lying if I said I’d never had something go wrong in the well over 9,000 days I’ve had a diabetes device attached to my body.
But when I stop and weigh up the risks and compare them with the benefits, there’s no question that diabetes technology has not only been beneficial to me, it means that I am healthier than I thought possible, sleep better and spend far less time consumed by the endless decisions diabetes demands.
Decades of evidence show that use of these technologies improves diabetes outcomes, decreases glucose variability and lowers the risk of diabetes-related complications. My n=1 experience (which, for the record should be irrelevant in anything other than me talking about my own experience) is that these devices mean that I am able to show up as the best version of myself, despite the incredible challenges T1D throws my way.
The reports today highlight an increase in the reporting of adverse events. An ‘adverse event’ can be anything from a pump failure, a cannula blockage, a sensor failing or reading incorrectly or an alarm not sounding as expected.
It can also be device tape not adhering properly. Or skin irritations.
It shouldn’t take a genius to understand that the reason for the increase in adverse event reporting is the significant increase in people using these devices, thanks to NDSS subsidies.
Should we have the right to feel confident that government agencies are evaluating and monitoring the safety of these devices and acting when necessary? Absolutely.
There are thousands of hours of research demonstrating the safety of these devices, and that, overall, the benefits of diabetes technology far outweigh the risks.
I’d like to ask the journalists who have published this beat up and cherry picked lived experience stories: what’s the alternative? Should we go back to injecting insulin and blood glucose monitoring? I mean, there can be errors with blood glucose monitors (or I could not have completely wiped Nutella from my fingers before checking my glucose), so should we go back to peeing on a stick? And should we stop using automated insulin delivery and go back to doing all the calculations in our diabetes-exhausted and burnt out brains? DIY diabetes – and a reminder that all diabetes is DIY – was always far more dangerous to me than any automation from devices.
And I’d ask them where are the stories from the thousands and thousands of Australians who use these devices every day and are not experiencing serious problems?
I’d also like to remind them that people with T1D don’t get the option of opting out of risk. The comparison isn’t between diabetes technology and zero risk. The question is which approach gives us the best chance of staying alive and living well.
The potential damage to advocacy efforts for expanding access to insulin pumps for people with T1D and access to CGM for people with other types of diabetes has been done with this ‘investigation’ – a term I use very loosely here. Or for the introduction of the next generation of diabetes tech. Sowing the seeds of doubt without countering with balance, is irresponsible journalism. And in this case, it’s people with diabetes who stand to lose out.
What you can do today:
Write to Sixty Minutes, The Age and The Sydney Morning Herald with your concerns about their biased reporting.
If what you’ve read has made you second guess decisions about your own tech use, take a deep breath and double check your contingency plans and the limitations of tech we are all told about, and how to minimise them as best we can. If you’re really worried, contact your HCP.
Disclosures, because, jeez, that’s important today (and perhaps could have been clearer from some of the experts in the reports…)
I have used Omnipod, Deltec (RIP Cozmo) and a number of Medtronic pumps since 2001, and Dexcom sensors since 2013 (as well as some Medtronic sensors prior to that, and the occasional Abbott Libre sensor). I currently use Loop (Omnipod DASH and Dexcom G6). I pay for all diabetes devices consumables via the NDSS, and private health insurance covers the cost of insulin pumps.
As part of my health consultancy business, I have consulted for Medtronic, Abbott, Dexcom and Insulet (in Australia and globally). These consultancies have been focused on community engagement, language and communications.
Today, diabetes stopped me. It does that, which is why I am always somewhat confused at the toxic positivity of statements such as ‘diabetes doesn’t need to stop you’.
It stopped my plans for a walk with my kid because my blood glucose levels, for some reason, wouldn’t budge beyond 2.5mmol/l.
Ad then it stopped me joining a meeting on time because I accidentally ripped my pod off (door frames should come with a diabetes tech hazard warning) and the entry to my home office looked like a crime scene as blood gushed from my arm, all over the paintwork and down onto the floorboards.
That was just today. These may seem quite trivial, but they are just a couple of moments in time explaining how diabetes does indeed stop us in the moment, and in more significant ways. We can say that diabetes doesn’t stop us. And that may be the case. Until it does:
Until I am paralysed by fear of my kid having inherited the genes that have meant I have T1D.
Until I am told that I have developed some diabetes-related complication and I start catastrophising about how it will mean I’ll lose my independence.
Until I am feeling so burnt out by diabetes that I am unable to do the tasks I need to make diabetes just run, keep up with and fill insulin prescriptions, remember to order pump consumables and CGM supplies. (Oh, hey! Stripped Supply can help with this!)
Until a night of high glucose levels means I need a few hours of recovery, stopping me from carrying out the plans for the following day.
Until a bout of gastro leads to a bout of DKA and I find myself being forced to stop everything, and instead spend hours in A&E. (Or, if I’m lucky and have access to the VVED diabetes service, flaked out on the sofa managing at home.)
Suggesting that diabetes needn’t stop us ignores the systemic barriers that are a very real driver to diabetes stopping us. And campaigns rooted in toxic positivity do nothing to actually address those barriers.
Diabetes still means people are stopped from pursuing the career they have always wanted. And in some cases, it stops people from continuing the careers they have already built.
The considerable costs of diabetes – even in a country like Australia – stops people from doing a lot of the things they’d like to do. For some, the impact of diabetes on the family budget stops weekly food shops, other healthcare needs being met and household expenses being covered, and stops holidays from happening.
In some countries, where insulin is not easily available, or available at all, diabetes literally stops people from living. It’s pure privilege and a luck of being born in Australia that means this isn’t my reality.
Diabetes does stop us. And when we suggest that diabetes shouldn’t be a barrier and shouldn’t stop us, it erases the reality of day-to-day diabetes. And it can make us feel as though we are failing if we do need to stop and take time out.
Happy National Diabetes Week in Australia to all who celebrate. And for those of you who occasionally, or frequently find that diabetes does actually stop you sometimes, I see you.
A post really only relevant to Australians with T1D, but the broader discussion about needing to include PWD in policy decisions and implementation processes is relevant to the entire diabetes community.
For many years, I worked for Australian diabetes organisations and one of the roles I had was to be involved in policy implantation plans. These discussions were typically highly detailed with many moving parts, and many stakeholders to consider.
One of the reasons I was included in these discussions was because it meant that there was a voice of a person with lived experience and expertise in the room who could point out the realities of proposed implementation plans or policy change. This was important, because often the practicality of what a change meant got lost as rules were drawn up.
When there isn’t a person with diabetes in the room, things happen that made our lives more difficult. Case in point – a few years ago when new AustRoads Assessing Fitness to Drive Guidelines introduced a requirement that an HbA1c below 9% be used as a measure of “satisfactory control” for licensing purposes. The result was confusion, anxiety and, in some cases, people with diabetes having their licences affected because of an arbitrary HbA1c threshold that seemed disconnected from actual driving risk and the realities of living with diabetes.
Today I received notification of an upcoming change to the NDSS and it seems there has been little consideration of how the implementation of that change will affect people T1D.
What’s the change?
Dexcom G6 transmitters and sensors will no longer be available on the NDSS from 1 October this year. Of course, this isn’t a surprise. We have seen the transition from G6 to G7 in other countries and it was just a matter of time before it happened here in Australia. While it only affects us now, Australians have known about this because we’ve seen our diabetes friends elsewhere around the world deal with it. This means we have had time to consider our options, stockpile G6 sensors and transmitters if we don’t quite feel like it’s time to change yet and chat with others about what their plans are.
In the email is this:
As you currently access Dexcom G6 through the NDSS, please see your diabetes health professional before 1 October 2026 to change to a new continuous glucose monitoring (CGM) device. They will discuss the most suitable device for your needs and make the change through the NDSS. We recommend booking an appointment soon, so your health professional has time to make the change before 1 October 2026.
My concern and outright frustration is about why the onus of this change is falling to people with T1D. Why are our NDSS preferences not being automatically changed to the new Dexcom product? Why are we required to see a health professional to do this?
If I were in the room when discussions about the implementation change, I would have pointed out the following: Many people with T1D have been using CGM products for years. It is possible to access different devices to those on our NDSS preference without a HCP.
And I would have asked:
Why isn’t there an automatic preference change to the new Dexcom product?
Why are people with T1D not able to make this decision themselves without mandated clinical oversight?
And if we must see a HCP to change brands, why isn’t that a decision we can make ourselves?
Some pumps only integrate with Dexcom CGM products, so what is there to discuss in that appointment?
Has anyone considered the expense that will be incurred by PWD needing an appointment, the lengthy wait time to see their HCP? I expect many HCPs will be happy to take care of simply making the change without an appointment, but if they insist, PWD will need to take time away from work or school.
Why is the language in this letter unnecessarily paternalistic? The idea that PWD don’t know what is most suitable for our own needs completely ignores that we manage T1D largely on our own (we get, on average, less than 4 hours a year with our HCP) and make hundreds of decisions every single day.
I completely understand that all people are different, and some PWD would prefer to see their HCP before changing tech devices, but that should be the choice of the person with T1D. Not the decision of an administrative process.
Diabetes admin will forever take up far too much of our lives. It frustrates me when unnecessary tasks are added to the never-ending to-do list because no one has asked a simple, but critically important, question: What will this mean for people living with diabetes?
During the World Health Assembly in Geneva in May, there was an interesting shift as the days of the meeting progressed. I am always on high alert about the language used at these meetings (remember the ‘adherence’ event last year?), and this year, there was a definite shift in the words used when referring to people with lived experience of the health conditions discussed in different sessions.
Lived expertise started popping up, used by session chairs and moderators. This didn’t just happen by chance. For some time now, bolshy advocates (hand raised and waving…bolshily) have been stressing that what people with lived expereince bring to the table is indeed expertise. No one else can do it, and it is an essential part of any discussion.
During one of the audience discussions, I made the point of highlighting the importance of framing what people with different conditions bring as expertise. I emphasised that there is no one else capable of bringing that perspective and knowledge. The following day the moderator from that session introduced speakers with diabetes as having lived expertise. One of my colleagues reached over to me and tapped me on the arm: ‘Look at that! She’s changed her language from yesterday’s session’.
This shift is reflected in the new Meaningful Community Engagement framework used at ALIGN-T1D, where there is the clear acknowledgement that lived experience is expertise. (Disclosure: I work in the Global Responsibility team at Breakthrough T1D, the secretariat of ALIGN-T1D). It’s not just a framework document – it’s genuinely embedded in the project’s work and governance structure, and similarly, more broadly throughout the whole organisation. Can I tell you the utter joy I feel when colleagues without diabetes are the ones spearheading this language change rather than it being the person with diabetes! I see them doing it not only deliberately, but because they mean it.
Lived expertise in the diabetes context
I think for some people with diabetes it might take time to come around to using the moniker ‘expert’. I wrote years ago about how some people feel the term ‘advocate’ is loaded, and how not everyone who engages in advocacy feels comfortable adopting the label. I imagine for those people, coming on board and referring to themselves as experts might be a stretch. I’m curious as to why, and I wish that the imposter syndrome or whatever it is that is holding them back disappears so they can recognise the skill and expertise they bring.
While everyone with diabetes has expertise in their diabetes, we also need to recognise that there are expertise and skills that are learned. If we genuinely want lived expertise to be valued in the same way as other forms of expertise, we need others to understand that too. Otherwise, we see tokenism flourish as ‘anyone with diabetes will do’
For example, my expertise as a diabetes advocate lies in the areas upon which I have lived experience and also laboured experience. (For more about the four Ls of experience, please see this incredible piece in Diabetologia last year, led by Linxi Mytkolli with contributions from other #dedoc° voices from around the world.) With that knowledge, I know that I absolutely have expertise in what it means to live every day with T1D: the relentlessness, decision-making, stigma, language, healthcare interactions and the countless ways diabetes intersects with the rest of life because I have lived that reality for decades and spent years examining and articulating those experiences through my advocacy and writing. I don’t have expertise in living with T2D, or T1D and experiences that differ significantly from my own. That’s why I say no far more than yes when asked to act as a community representative.
My work – my laboured experience – means that I bring expertise around diabetes language, stigma, peer support, community engagement, advocacy and strategic communication. I have sat on numerous advisory boards and steering committees and, over time, developed the skills and expertise to lead and chair these groups. After spending years of acting as organisation spokespeople, I have expertise in media engagement and messaging. If I was asked to lead the design a diabetes registry or epidemiological study, I’d say no – that’s not where my expertise lies.
The problem with recognising lived experience as lived expertise is that there remains the issue of tokenism. If people’s expertise and skill as advocates or advisers or community representatives are overlooked, and anyone with diabetes is considered suitable, then we diminish the expertise they bring. To be involved in decision-making and advisory processes means having the confidence to push back, to challenge assumptions, to ask difficult questions and to recognise and overcome the real and perceived power imbalances that often exist in these spaces.
I will always say that people with diabetes should be centred and involved in all aspects of diabetes, but perhaps the caveat to that there needs to be consideration to match the right person with the right expertise to the right role. And that shouldn’t be surprising. After all, we readily accept that executive leadership positions, policy roles and research leadership roles require specific expertise and experience. Lived expertise should be treated with the same respect.
Recognising lived expertise means changing the questions we ask about who is involved in projects, advisory groups and decision-making processes. Instead of asking, ‘Do we have someone with diabetes at the table?’, we should be asking, ‘Whose expertise do we need?’ and ‘What experiences, skills and perspectives are missing from this discussion?’. Those are very different questions, and they lead to very different outcomes.
It also means being prepared to invest in people. We would never expect researchers, healthcare professionals or policymakers to become experts without mentoring, support or opportunities to develop their skills. The same should apply to lived expertise. If we want meaningful engagement, we need to support people to build confidence, gain experience and develop the skills needed to contribute effectively.
Linxi and Renza: a couple of bolshy diabetes advocates with years of lived expertise at the End Diabetes Stigma Summit.
There’s a social media…thing…at the moment: Yes…but*. It’s designed to show the contrast between the glitz and glamour of perfectly curated socials feeds for the reality of life.
In fact, these days, diabetes to me is more ‘Yes…and?’.
I’m exhausted thanks to the relentlessness of diabetes? Yes…and? Of course that’s the case. Diabetes demands so much of us.
I’m over the daily grind of diabetes? Yes…and? What else is to be expected? Diabetes bores the shit out of me.
I’m burnt out thanks to diabetes? Yes…and? Who isn’t? In fact, tell me you’re not burnt out at least some of the time and I want you to speak to me as though I’m five years old and teach me your ways.
I ripped out a sensor on my arm because I walked into a doorframe? Yes…and? I still have no spatial awareness of my body. Or doorframes.
Someone said something stigmatising about diabetes? Yes…and? People are idiots and don’t understand diabetes. (Although I probably will call that rubbish out because people don’t get a free pass to be stigmatising arses.)
Diabetes technology is in equal measure brilliant and imperfect? Yes…and? Two things can be true at the same time.
Some bloke (who doesn’t actually live with diabetes) is being an arsehole to a woman with diabetes who is highly respected and trusted in our community? Yes…and? Bullies in the community have existed forever, and will forever, and misogyny online is sadly alive and well.
I had three hypos before lunch? Yes…and? Sometimes diabetes just chooses violence.
I nailed my time in range yesterday and today it’s rubbish? Yes…and? Yesterday’s diabetes has never accurately predicted today’s diabetes.
A healthcare professional referred to me as ‘non-compliant’? Yes…and? People continue to confuse judgement for healthcare.
Another miracle cure has appeared in my inbox? Yes…and? Scammers gonna scam.
A diabetes organisation says people with diabetes are at the centre of all they do? Yes…and? Until I see evidence of PWD actually having an ability to influence, holding leadership positions in the organisation and being genuine partners and not props, it’s just tokenism wrapped up in a catchy slogan.
I have diabetes, and I’m kicking goals today? Yes…and? Those things have never been mutually exclusive.
I have diabetes, and I’m struggling today? Yes…and? Those things aren’t mutually exclusive either.
Social media has finally caught on that life isn’t all shiny and perfect? Yes…and? Welcome to diabetes. We’ve kinda known that forever.
*Of course, nothing is really new. Artist Anton Gudim has been creating ‘Yes, but’ cartoons for years now, with far more finesse and creativity than any content creator jumping on the bandwagon.
I’ve started this post a dozen times over the last ten days as I’ve tried to put together a personal reflection on the life of my friend Bastian Hauck. If you’re in the #dedoc° or broader diabetes community, you will undoubtedly have seen some truly beautiful messages and tributes. What more can I say that hasn’t already been said?
What I really want to write about is my friendship with Bastian in all its glory, which to be honest wasn’t always glorious. He referred to me as his sparring partner because I was the one who challenged him and pushed him to think in different ways. I was the one who asked him to stop and take a beat before making a decision. I was the one who told him when I thought he was out of line. I was the one who asked him to listen and try to see others’ perspectives.
When we’d speak, regardless of who called, the first thing I’d hear from him was a question. ‘Renza?’ he’d say. I don’t know who else he was expecting, but the inflection in his voice rose. Making sure I could hear him. ‘I’m here,’ I’d say. And we’d talk.
Our ‘quick chat?’ messages that preceded calls were lies. It became a habit to send each other a message as soon as we eventually hung up with the minute count of our call. ‘58 minutes!’ I’d write. ‘Why can’t we have quick calls?’ ‘Let’s not change that,’ he once replied.
Bastian was one of my closest friends. Despite living on opposite sides of the world, I spoke to him more than any of my friends nearby. Thanks to crazy travel schedules, we’d see each other four or five times a year. But it was in between those in-person catch ups that we’d spend hours talking about #dedoc°. I can’t count the number of times we’d talk each other of ledges after some particularly annoying incident. He’d explode over an encounter with someone and want to start an all out war with them. ‘Don’t give it air, Bastian,’ I’d urge him. He’d rant and rage and tell me in detail what he intended to do to make the situation right and confront them. I’d ask if it were really worth the effort. Eventually, he’d calm down. Just in time for me to blow up at the nastiness of online interactions, and then it would be my turn to rant and rave. And he’d tell me not to worry about them and remind me of my advice to him: ‘Don’t give them air’.
One of the last messages I sent him asked ‘How have we managed to do this for so long and just get things done?’ What I didn’t add was: ‘How do I keep getting things done now?’
A year after he met, he came to Melbourne for the 2013 IDF Congress, and had dinner at our home with a group of global advocates. He spoke frequently about that dinner, mostly because the following day he was taken to the outer suburbs of Melbourne to see kangaroos. Monique Hanley, if you’re reading this, you were a hero to him for organising that trip!
That was one of the things about Bastian. He held on to those sorts of memories and shared them over and over. Kangaroos? Just jumping around the place? And he got to see them? Amazing! I can’t tell you the number of times I heard him say ‘And the next day after dinner at your house that wonderful woman Monique took us to see Kangaroos’. ‘I know, Bastian’, I’d say. ‘I was at the dinner. At my house. I introduced you.’
Our stories in the diabetes world have been so intertwined. This week people keep sending me photos of us on stage at different conferences, the #dedoc° logo behind us. ‘Bastian, make sure the #dedoc° branding is there. Bright. We want people to know it’s #dedoc°,’ I’d say. ‘We want people to hear the stories, Renza,’ he’d reply. ‘Yes…but also that #dedoc° made that possible’. My comms hat is never far from planted firmly on my head. It annoyed the crap out of him. I didn’t care.
And people have sent me videos and recordings of interviews and podcasts we did together. I snapped those shut before they started. Because how is it possible that Bastian’s voice – that voice I’d hear three or four times every week at the end of the phone – is now only there in old recordings?
I regret every time I told Bastian to talk less. ‘You don’t need to go over that again,’ I’d say as we were prepping for a #dedoc° symposium at one conference or another. ‘Get off the stage and let the speakers speak!’ But he just wanted to yell from the rooftops about the #dedoc° community and how far we’d come. And the allies who helped us there. And mostly the incredibly #dedoc° voices who were family. He couldn’t stop talking about it!
We’d do EASD TV each year and when we finished our interview he’d always ask me ‘How do you do that soundbite thing?’, referring to the succinct way I’d answer a question, with grabs that I knew would make it to the promo for the video. I’d laugh and tell him, ‘By saying as few words as possible, but making those words count. Fewer words, Bastian.Say less!’ Now I wish I’d let him ramble on and on.
The last time I saw Bastian was in Vienna last year at EASD. It was not an easy conference. We were managing a difficult situation at #dedoc°. He and I disagreed on how to deal with it, and I returned home feeling frustrated, angry and exhausted. ‘Renza, you need to step back from this one,’ he said. I knew he needed to feel in control of something – anything – at a time when so much of what was going on in his life was big and scary and way beyond his control.
And so I did. I stepped back. And there were a couple of months where when spoke and sent messages there was, undeniably, a discomfort in our words. It didn’t last long. He recognised the tension. He apologised, I did too. I think we both knew that we couldn’t waste time being wary around each other. There was too much to do. There was not going to be enough time. We were trying to steer #dedoc° to safe waters.
And there’s a sailing analogy, because there always are in conversations with Bastian. He wound in the fact that he was a sailor into every conversation he could. ‘When I was on the big boat last summer in Copenhagen…’ he would begin. And I’d try not to laugh because it wasn’t enough for him to mention he had a boat. He had to mention that he had a big boat, suggesting (rightly) the existence of a small boat. God forbid he said it out loud at a conference or in a room with our beautiful friend Amin. He and I would glance at each other, or send a message, desperately trying to not laugh. Amin…one of Bastian’s closest friends. My heart breaks for him too right now.
It was the weekend before last that I spoke with Bastian for the last time. ‘It will be a quick conversation.’ I was told by his friend who was organising the call. ‘I understand,’ I said, thinking that perhaps we would actually have a short call. Maybe now was the time we changed things.
But Bastian had things he needed to say to make sure I understood what he wanted for #dedoc°. ‘Bastian,’ I interrupted. ‘You’ve done enough’. ‘Shut up, Renza,’ he pushed back. Now’s not the time to tell him to watch himself, I thought, so I listened. I listened to his voice and his words and took notes, interjecting only to promise to follow up.
And then it was time. ‘I’m sorry I didn’t come to see you,’ I said. He said he was too. I know he really wanted us to say goodbye in person. I couldn’t make it work. And I think that, selfishly, I didn’t know that I could face everything.
Instead, just as we had done countless times before, we said goodbye to each other on a phone call. ‘Thank you for everything’. I said. Or did he say that? Perhaps we both did.
And then I sat there, looking at the timer on my phone. Forty minutes. Our quick call, on the day he died, went for 40 minutes. I smiled through my tears. I guess we didn’t change it after all.
There’s an urge we have when someone we know dies. We desperately try to hold onto our connection to them. In a world of social media, we want to show the world that connection – how we knew the person. How we met them. How we existed within their orbit.
Bastian’s orbit encompassed so many people. How lucky we all are to have known him.
But his passing isn’t about us. No matter how many photos we have with him.
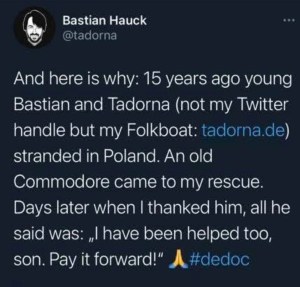
Bastian’s favourite saying was #PayItForward. It was one of the core principles upon which he built #dedoc°. It is why #dedoc° has always been a platform upon which others stand and shine. Bastian never wanted #dedoc° to be about him, or for #dedoc° to be the story. It was always about elevating others with diabetes. Making sure the platform was sturdy enough to hold as many as possible. That was how he wanted to #PayItForward.
This is the story of where that saying came from, in Bastian’s own words from a very old tweet.
Perhaps the best way to honour Bastian is to remember these words and look to how we can support others, just as he did for so many. And take a back seat while doing so.
Go well, my dear friend. Thank you for showing up.
Recurring themes in diabetes recur for a reason: they impact people with diabetes. And stigma is one theme that you will hear people with diabetes speak about a lot. A. Lot.
Last week at the World Health Assembly in Geneva, there was much discussion about stigma – both within the diabetes and in other health condition spaces.
Stigma harms everyone. It goes without saying that there is no good form of stigma.
When speaking with people from other health organisations, it was interesting to learn that many see diabetes stakeholders as being leaders in addressing stigma.
There was a lot of interest in how we had come as far as we have. I shared what I knew and what I’ve been involved in and there was awe at the number of different activities that have involved so many stakeholders.
I agree that we are making strides in addressing diabetes-related stigma. But I’m afraid I wasn’t quite as enthusiastic as the people I spoke to who seemed to think that we had it all sorted. That’s sadly not the case. Every single week I hear from people with diabetes about the stigma they are experiencing, and the discrimination they have to deal with because of diabetes.
Last week, I found myself cringing at the airport when a security guard mentioned that perhaps if my diabetes was better managed I could stop using the devices attached to my body. He knew, you see. His niece has diabetes and she doesn’t need one of those machines.
I was too tired after hours of travel to do anything more than roll my eyes and say ‘That’s not how diabetes works’, and suggest that he doesn’t offer strangers unsolicited advice. I wondered if he had the same level of comfort telling someone wearing a pacemaker what to do to better manage their heart condition. Probably not.
And I snapped a sassy response on the Instagram page of one of my favourite bakers when someone suggested that dipping rhubarb in sugar was a one way ticket to diabetes. As if that’s all there is to this highly complex condition.
I’m tired and yet the stigma I deal with seems quite superficial when compared with that of many of my diabetes brothers and sisters living in other parts of the globe.
Diabetes stigma is real. It is harmful. It needs to end. And we all have a role to play in getting us to that end. I say that knowing that sometimes it’s too exhausting to do anything – and that’s perfectly okay. The full time job of managing diabetes is more than enough. Busting stigma shouldn’t also be on our to do list.
But if you have time, if you have the energy, if you have the will, there are some easy things you can do.
Sign the pledge to end diabetes stigma. You probably already have, especially if you’ve been hanging around here for a while. So perhaps, you could spend five minutes sharing the link to the pledge, or finding someone you know hasn’t signed it, and asking them to. It takes under a minute.
If you’re doing any sort of diabetes advocacy about stigma, circulate the International Consensus Statement to End Diabetes Stigma. Evidence matters, and this document brings together 51 experts across 18 countries. It was published in the Lancet and it is an excellent foundation for any work in the stigma space.
And if you want to see a video of joy, watch the one linked below. This is a compilation of what happened at the Summit to End Diabetes Stigma held in Jaipur in March this year. I assure you that amongst the colour and vibrancy you see in the video, there were difficult discussions, impactful panel sessions and plans for how to make real change.
My new friends from last week were impressed with what’s been done in the diabetes space, and I agree – the community has done so much already. But we’re not done. There’s a lot more to do. We’ve come this far because dedicated people have worked collaboratively. Community members have shown up to share their experiences. I’m so pleased to be part of these efforts. And will keep rolling up my sleeves as we address what still needs to be done.