
You are currently browsing the category archive for the ‘HbA1c’ category.
Earlier this week, diaTribe shared this on their Instagram:

It did not sit well with me at all. And I don’t understand the reference to stigma.
A1C is flawed. People with diabetes have been saying this for decades. To have our overall diabetes management measured by an average that gives no nuance to other factors is not a good way to assess health or guide treatment.
CGM changed all that, with visibility into just what is going on with glucose levels at all times. I finally understood why I was so tired some mornings, despite eight solid hours of sleep with in-range numbers at bedtime and at waking. I saw the rollercoaster nights, or the hours at time I was low. It became very clear that my nighttime glucose adventures were exhausting me.
As more people had access to CGM, TIR was heralded as the new gold measuring standard. And it was everywhere. I wrote and spoke about it a lot because the real-time data gave me a clearer understanding of my diabetes. But with that excitement came a gnawing discomfort: were we just swapping out one metric for another?
After a couple of years of TIR, and with the advent of newer, smarter AID systems there was a new kid on the block: Time in Tight Range (TITR). Target upper and lower limits were tightened and there were expectations of remaining within those ranges.
I nodded along because I was, for the most part, comfortably sitting within those number thanks to Loop. And yet, my discomfort grew. More pressure, more expectations on people with diabetes based solely on numbers, and a continued widening of the gap between people with access to tech and those without.
At ATTD a couple of months ago, there was the announcement of a new metric: Time in Normo-Glycaemia – TING! (There is no exclamation mark after the acronym, but it reminds me of the celebratory sound my kitchen timer makes when a cake is done baking, and that deserves festive punctuation.) And horrifyingly, to this #LanguageMatters boffin, the new acronym includes the word ‘normo’. Language position statements have always, always advised against using the word normal/normo. The word shapes attitudes that contribute to stigma. In one study, 85% of PWD surveyed found the word unacceptable.
These measures still focus on one thing: our glucose numbers. There are goals for the percentage of time each day we should be aiming to be in (ever-tightening) range. So, effectively, the HbA1c percentage has been replaced with time in range percentage. It’s still focusing on nothing more than numbers. It still sets us up for a pass/fail framework.
A1C, in itself, is not stigmatising. It’s a number. The language used when discussing A1C can be stigmatising. Attributing success in diabetes to an A1C number can be stigmatising. Being told we’re failing for not reaching an A1C of a certain number is stigmatising. But all of those things are true of TIR.
Before anyone comes at me and tells me that PWD should be able to have numbers within a tight range, of course that’s true. But isn’t that already the goal of our diabetes management? Isn’t that the point with all the glucose measuring, insulin dosing, and considering the bazillion other things we do to manage diabetes? I don’t know anyone with diabetes who does the work with a goal of glucose number of 17.0mmol/l; an HbA1c of 14%; a TIR/TITR/TING of 11%.
But replacing one measure for another still traps us in a numbers-only mindset. How is ‘What’s your TIR?’ really any different to ‘What’s your A1C?’ Does it free us from being metrics-focused? (Some might argue that it ties us to numbers even more with daily updates about how we’re tracking.) Does it address stigma?
I’m not sure it does. I’m not convinced that there is any relevance at all to stigma in this conversation. And I’m a little annoyed at the conflation. Diabetes-related stigma is very topical now, thanks to important efforts by PWD, community groups, researchers and clinicians in the diabetes space. If I was being cynical, I’d suggest that this is an opportunistic attempt to jump on the buzz movement of the moment without meaningfully engaging with what stigma really is or how any type of metric can contribute to it, depending on how it’s framed and used.
Postscript – but possibly the most important part…
And finally, but perhaps most importantly: the very idea that we are suggesting this is the gold standard when it is inaccessible to the vast majority of people with diabetes is just so out of touch. According to the diaTribe article that accompanied the Instagram post I shared earlier, worldwide 9 million people are currently using CGM as part of their diabetes management. The IDF’s latest Atlas data, (launched last month) reports that there are about 589 million adults (20-79 years) with diabetes across the world. That doesn’t include children and young people. (1.8 million young people are estimated to be living with T1D.)
Isn’t this one way stigma takes a hold? When we’re talking about targets that are only available to the small fraction of the diabetes community who can access the tools to achieve them. Setting standards around tech that most can’t obtain doesn’t just ignore reality—it reinforces the stigma of not measuring up.
The longest queue in the exhibition hall at ADA was not people waiting to see an exciting new therapy breakthrough in diabetes. It was not interest in the latest shiny and bright new device. It was not even a line for free coffee.
 No. The longest queue was for on the spot A1c checks. Two booths were doing them – Abbott and A1cNow Systems. Abbott had run out after a couple of days, but the A1cNow folks managed to keep up with the demand at their booth.
No. The longest queue was for on the spot A1c checks. Two booths were doing them – Abbott and A1cNow Systems. Abbott had run out after a couple of days, but the A1cNow folks managed to keep up with the demand at their booth.
A couple of my mates with diabetes and I had commented at the never-ending line of HCPs so eager to know their A1c. Why was this the attraction of the exhibition hall?
On the final day the exhibition hall was open, I was doing a last wander around. End of conference fatigue was clearly settling in – the reps on the stands were a little less enthusiastic about approaching people walking by, and conference delegates had lost the pep in their step and seemed to be drifting a little aimlessly. Or maybe people just needed more coffee. But despite the reduced buzz, I saw that yet again (or maybe still) there was still a queue snaking its way around the A1cNow stand.
‘I need to try to understand why they are doing this,’ I said to the friend I was wandering around with. ‘Let’s go and ask them.’
So, we introduced ourselves to a few of the people standing in line. They were health professionals and were happy to chat.
‘So,’ I started. ‘I guess I’m trying to understand just why you are wanting to get your A1c checked. Do any of you have diabetes?’
They all shook their heads. Their responses ranged from ‘I’m just curious’ to ‘It’s free and I many as well have it done.’ One person said, ‘I have a family history of diabetes.’
One of them asked me why I was asking. ‘I’m really understand to know why there seems to be such a keen desire to know what your A1c is when it kind of doesn’t really matter. I generally avoid getting mine done and I am meant to have it checked every three months. I know people with diabetes who have gone years not having theirs checked. For us there is a lot tied up in it. We feel judged by it. It’s often presented as a way to measure our success as a person with diabetes. We are told we are ‘good’ or ‘bad’ depending on that number. I don’t know too many people with diabetes who would voluntarily line up to get it done really.’
Back home, and I was talking about this with my gorgeous neighbour.‘It was the longest queue at the conference. More people wanted their A1c than to get a coffee!’ (Admittedly, this could have something to do with the state of coffee in the US, but maybe not.)
My neighbour rolled her eyes. ‘It’s like at parties when someone sees you do a blood sugar check and wants theirs done. You know – they get all excited and hold out their hands ‘Do me. Do me!’and then you do and it’s four or five and then you do it again and it’s still four or five, and they’re all excited and ask, ‘That’s good, right.’ And then yell out to everyone about how ‘good’ their number is and then they see the 14 on the meter when you do yours and shake their heads and tell everyone how crap that is.’
She’s right. That’s EXACTLY how it happens!
But returning to ADA… I thanked the HCPs waiting patiently in line and walked away, sighing. I wasn’t getting my A1c checked, there was no need for me to be there. Because getting that done takes the right mindset, and a strength that I just wasn’t feeling at that point. I hadn’t psyched myself up and given myself the pep talk I need before having that measurement handed to me.
And then, it all circled around to another example of ‘doing diabetes’ at different conferences, and my similar annoyance at the long lines for hypo simulators. Or my outright displeasure at people whacking diabetes devices on their bodies to learn what living with diabetes is all about.
Setting aside the very high likelihood that I am turning into a grouchy old woman, I really think that these sorts of exercises are problematic for PWD. No one in that A1c queue was feeling any anxiety about the number the machine was going to spit out. I asked if they were worried and they all shook their heads. It was just a thing to do at a diabetes conference for them. Most likely, they were going to come out with an in range number that they would forget as soon as they walked to the next stand.
Hypo simulators make people feel a little wonky for about five minutes after they get out of them and then they are back on solid ground, not thinking about what is really going on with their glucose levels and how they will affect them for the remainder of the day.
And after wearing a pump or a CGM for a week, it can be returned and never thought of again.
I have been criticised when I have said that it is only people with diabetes who truly understand the impact of diabetes on our lives. I’m willing to wear and own the comments I make. I say this without malice or by trying to limit or minimise the experiences of those living around us. I just don’t understand why there is this idea that by ‘doing diabetes’ or rather doing some of things we have to do as part of our diabetes is really useful.
I would love it that if of HCPs lining up to have a pointless A1c check done, they had sessions in the booth given by PWD where we had a chance to speak about why some of us are so anxious when it comes time to having ours checked. We could offer suggestions about how to talk about results in a way that makes us not feel measured or judged.
And instead of hypo simulators, how about a panel of people with diabetes explaining just how we feel about hypos and how they affect us. When I did this at HypoRESOLVE, the researchers and clinicians were astounded and surprised at what I had to say.
There are a lot of ways that people not living with diabetes, but living around it, or working in it can get a better understanding of how we truly feel about having diabetes in our lives. I just don’t think that a one minute, five minute or even weeklong exercise is the right way to get that insight. The best way is to listen to us.
The day before ADA kicked off, I managed to catch a glimpse – my only glimpse this visit to San Francisco – of the Golden Gate Bridge from the back of an Uber on the way to the Diabetes Mine Summer DData Exchange (#DData19).
This is the third DData I’ve attended, and it always delivers. The speakers are brilliant and the topics on the agenda push some of the boundaries we’re used to seeing as part of the ADA conference that runs alongside. Amy Tenderich expertly emceed the day, and Mike Hoskins’ rapid fire tweeting made sure that those not in attendance had a birds eye view of the event.
This year, there was one session that really stood out for me and it was a panel session moderated by Adam Browne from diaTribe and included JDRF International CEO, Aaron Kowalksi and Alain Silk from the FDA.
For some time now, there have been efforts to move away from the idea of HbA1c being the be all and end when it comes to assessing the outcomes of diabetes management.
This doesn’t only mean in terms of the way we measure our own personal diabetes management, or the success or effectiveness of the devices, drugs or treatments on offer, it also is directed to researchers, clinicians and regulators who continue to use A1c as THE measure to determine the value of whatever they are talking about.
The push has been towards time in range (TIR) because with tools such as CGM and Flash glucose monitoring, this is something that can be easily measured and demonstrated.
The A1c is flawed – we all know that. Anyone with diabetes will have tales of A1cs going down, despite their diabetes management being more erratic, or conversely, their A1c increasing despite having fewer roller-coaster episodes. As a one-off number, it tells very little.
But while TIR is certainly one different way of having a look at just how we are tracking, with so few people actually using CGM or Flash (due to access and affordibilty), we can’t throw out other options. The A1c is not dead yet (just ask the queues of HCPs in the Exhibition hall at ADA waiting to get theirs done. Another blog post for another time…)
Also, TIR cannot be the only other measure we look towards as a substitute for A1c, and this session at DData explored more than the idea of a simple like for like between the two.
Aaron Kowalski highlighted how one of the first things people speak about when using an automated insulin delivery device is how their sleep improves. It was indeed the first thing that I noticed, and it was life changing for me. I noted that I slept like I did before diabetes!
Yet, this is not considered as part of regulatory decisions. Neither is how our diabetes experiences can be transformed. Aaron told the story of a young woman who rarely attended to diabetes tasks when around friends because she didn’t want to pull out her pump to check her CGM trace, or bolus insulin. She didn’t want to draw attention to herself or her diabetes. But being able to do those tasks by simply looking at her phone, or her smart watch meant that she felt so much better – and she did what she needed to do when she needed to do it. How are those improved experiences being documented and considered as part of why something is valuable?
In his earlier talk, Alain Silk from the FDA noted that one of the challenges when it comes to technology regulation is too much regulatory and contractual burden and not enough innovative devices getting into the hands of people with diabetes. The DIY movement manages to sidestep that first part and that means that we do have get to have those devices – those transformative devices – in our hands a lot sooner. Our experiences – which all seem to be positive – and our diabetes outcomes – which all seem to report improvements – really should count for something.
Surely one of the goals we are all seeking (and when I say all, I mean everyone involved in any aspect of diabetes) is to increase the time we DO NOT spend on diabetes anymore. At DData last year, DIY-er Justin Walker said that he believes he has gained back an hour a day since using an automated system. That’s seven hours a week. Over a year, that’s more than a total of fifteen days we get back from diabetes. Add that up over a lifetime of diabetes. It’s significant.
Aaron said that one of his goals as CEO of JDRF is to ‘…take diabetes out of our lives as much as is humanly possible.’ When devices allow us to do that – even if it’s just one little bit – that should be assessed as meaningful.
I have been thinking about this session a lot. In fact, anyone who has asked me about ADA has received a lecture on it. My poor boss got an earful when I returned to work on Monday. I’m pretty sure he regretted asking how I’d gone in San Francisco after I launched into a tirade about how we are simply not listening enough to people with diabetes when it comes to just what we are measuring as being valuable to us.
The problem with adding TIR to A1c as a way to assess devices, drugs or other therapies is that we still are focusing on nothing more than numbers. Sure TIR may be more robust and not simply a snapshot average, but it still attributes our success to a number.
When I talk about why Loop has been so transformative to me, I do mention TIR. But the biggest bangs for my buck – the things that really ring true – is not how much time I spend between two number goal posts.
No.
It’s about how much better I feel about my diabetes. It’s about how much less time, less worry, less stress I am forced to dedicate to diabetes. It’s about how the hypos I have these days take three minutes to deal with rather than three hours. It’s about how less stubborn, and how less frequent those highs are. It’s about the much lighter shadow diabetes casts over my family. It’s about sleep – oh dear god, it’s about sleep! It’s about how easy it is to carry out those required tasks and how little they interfere with my day. And it’s about the time I have been able to claim back as my own.
The footprint of diabetes is so far smaller these days than ever before. THAT is what is meaningful. THAT is what I measure. THAT is what it means to truly go beyond A1c.

DISLCOSURES
I attended ADA as part of my role at Diabetes Australia. My economy flights and accommodation have been covered by the organisation.
Thanks to the team at Diabetes Mine, who kindly provide diabetes advocates with the opportunity to attend their DData Exchange at a significantly reduce cost.
I have been interested in discussions about time in range (TIR) for some time now. It has become a key way that I assess just how I am tracking with Loop and, as I wrote earlier this year, really the only measure I’m interested in. I like it because it can give me real time information about how I am tracking. It shows that when I am at a conference and not eating properly, but doing more activity than I normally would, my TIR is going to be less than if I was at home in a regular routine. It also shows what happens when I’m not Looping for ten hours (thanks to a variety of factors) my TIR plummets!
At ATTD this year, there was a symposium dedicated to the topic and from the standing-room-only crowding of the hall, it’s clear that a lot of others are interested too. In the few presentations I attended about the Medtronic 670G, TIR was frequently referred to (in one study there was a slight increase in TIR after PWD had been using the device for 8 months, although significantly lower than what people using DIYAPS are reporting.)
Just as I did while live tweeting the session, I have to address the issue of access to the technology. TIR is all very well, but it takes tools, and those tools are prohibitively expensive. Some places have no subsidies available for CGM or Flash, others have limited reimbursement programs. And, of course, there are places around the world where accessing glucose strips is a near impossibility.
TIR is a measure for a very, very privileged few, and as much as it’s held up as the future of diabetes, it is simply incorrect and misleading to suggest even for a moment that most people with diabetes have this data at their fingertips. (They barely have finger prick data at their fingertips.)
But, this is a conferences about the latest in technologies and treatments, so let’s talk time in range…
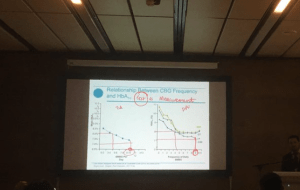
Dr Irl Hirsch is an MD from University of Washington, Seattle. His session as listed in the program was: ‘Time in Range vs. HbA1c: Are our patients ready to change?’, but he changed it to a far more suitable ‘Time in Range vs. HbA1c: Are our patients and health-care colleagues ready to change?’
Irl’s short talk was an absolute cracker and started by exploring what we already know – A1c is flawed. We’ve known this for years, but it’s taken having easy access to CGM data to truly appreciate just how flawed. The two points he raised to back this up were A1c levels can’t be compared between two people (and yet that happens all the time!); each A1c comprises a wide median glucose range. In other words, A1c sucks (they were his words, not mine!).
And then the talk got fun as the focus shifted to just how ready different groups were to shift from a focus on A1c to TIR. The three groups were: people with diabetes (and their families), endocrinologists and non-endocrinologists. Irl presented the results from a survey of diabetes HCPs asking their thoughts on the readiness of those three groups to embrace TIR. Here are the results:
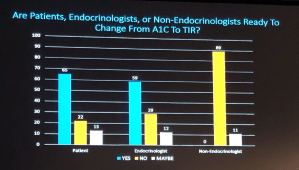
The HCPs surveyed all believe that PWD are by far the most ready to change from A1c to TIR. At the same time they believed that no non-endo HCPs were ready. We really have a problem.
The survey participants offered a lot more than just their assessment of the readiness for this shift. They provided extra comments about some of the barriers to the change. This is how some of the HCPs (all working in diabetes) assessed the inclination for PWD to move to TIR:

But perhaps the most unsettling was what they thought about non-endocrinologists willingness to start to talk TIR. (I think that they were mostly referring to primary care physicians.)
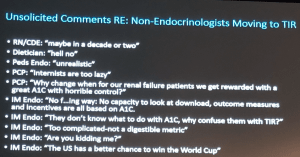
As the list was read out, and the audience responded accordingly, my confidence level about how likely it was that TIR would start to become the norm shrank away. This is despite the way that many PWD have already adopted the measure and use it daily.
In the online groups where I spend a lot of time playing, it is clear that we are already very comfortable and committed to talking TIR. People frequently post their Dexcom Clarity data showing the super-nifty image of how much time they have spent in and out of their self-determined range. This is the language we speak.
But despite my unease about just how quickly the shift will happen, it has definitely begun. The International Consensus on TIR was presented which included targets for people with type 1, type 2 and for women during pregnancy. Plus there was evidence presented that showed TIR can predict the likelihood of diabetes-related complications. With all this, and the demand from PWD, we will be hearing about this more and more in coming years.
Looking for more? This piece by Irl Hirsh, Jennifer Sherr and Korey Hood was just published in Diabetes Care is a really interesting commentary on the issue.
DISLCOSURE
I attended the ATTD conference in Berlin. My (economy) airfare and part of my accommodation was covered by DOCLab (I attended an advisory group meeting for DOCLab), and other nights’ accommodation was covered by Roche Global (I attended the Roche Blogger MeetUp). While my travel and accommodation costs have been covered, my words remain all my own and I have not been asked by DOCLab or Roche Global to write about my attendance at their events or any other aspect of the conference.
I’ve been Looping for about 17 months now. I’m a fan (perhaps you may have picked that up).
The reason I am a fan has nothing to do with my A1c. In fact, right now, I couldn’t tell you what my A1c is (more about that later). I love Looping because it works for me. It takes away a shedload of my diabetes tasks. It helps me sleep better. It gives me more energy. It means I think about diabetes less. It significantly, significantly, significantly reduces the number of hypos I have, and the impact of the almost-hypos that have replaced the doozeys used to have. It means I get to wear cool t-shirts.

Badge of honour…
Because in exactly the same way as if I have tried a different eating plan it’s never been about numbers on the scale, Loop has never been about A1c.
It’s especially never about a measurement that is so flawed that it really is time to wonder why, for me and those of us who are able to access far more informative and useful data, even bother to have this checked. (Read this piece by Dr Steven Edelman from TCOYD for more on that.)
I have to say that I feel a lot of discomfort when I see A1c as such a focus. Some if it is for the reasons I’ve already stated, but also, it reinforces that we measure our success as PWD and how we are managing with this number. If my A1c went up this time, I really couldn’t care less. I’ve not long come off three weeks of holidays where diabetes barely interrupted the flow of sunshine, sea and sleep. And family, friends and food. I have not had a hypo in months. I have not had days of wanting ‘I hate diabetes’ tattooed across my forehead.
I went to my endo appointment last week still in slight January holiday mode. I completely forgot to call ahead for a pathology request – in fact, I’d forgotten all about the appointment until I was sent the text reminder a few days earlier. I used to think it was a waste of time not showing up without results waiting for me. But I wasn’t really all that concerned this time. I had some other information at hand including how much time I am spending in range. That gave me enough to focus on before I moved onto other things I wanted to talk about: the things that are really important to me with my diabetes.
Living well with diabetes is about so many factors. Those factors will be different for different people (and yes – A1c may be how some people consider living well).
As someone who has had really dark times with diabetes, it’s the light times that demonstrate how well I am doing. Those times may not be the times that I am ticking boxes that we are told gauge our success. They have certainly not been times necessarily marked with a low or in-range A1c. They are the times when the impact of diabetes is lightest. When it dances across my conscious rather than lives there. When it casts a gentle shadow rather than a thunderous cloud. A1c has never had anything to do with that.
I had an endo appointment yesterday. It was my first in over six months, but this was by choice, rather than inattention. Last November, I decided that I really didn’t need a three month follow-up appointment, and my endo agreed. So, after settling my account for the visit, I made an appointment for May this year. A work trip to Copenhagen via London necessitated a reschedule and this was the first appointment time available that worked for me. The six month follow-up timeframe was pushed out to eight months.
Early last week, I called for a pathology request to be sent to me so I could have a blood draw before heading in. While I had a list almost as long as my arm of things I wanted to discuss, I really am trying to stay on top of having regular screenings so that we can compare results year to year.
Clearly, I am in a really good headspace about my diabetes and, in particular, diabetes HCP care, at the moment. I am happy to attend appointments. Even though I needed to cancel the May appointment, I made a follow up and kept it. I had all my bloods done beforehand. This is a far cry from how I was just a couple of years ago … when actually, I was crying just thinking about it all.
So, last Thursday, I made my way to a local pathology clinic, my request slip scrunched tightly in my hand. And I realised that even with my generally low level of worry about all-things-diabetes, I felt my anxiety levels going up in the days leading to, and the day of, the blood test.
‘I’m nervous about having my A1c done,’ I said to someone last week, and, puzzled, she asked why. It was a sensible question to ask, because truthfully, of all the things I was being checked for, that was the one that I had a pretty good idea what the result would be.
I estimated my A1c and got it right to 0.2 percentage points. The truth is, I am totally ambivalent about A1c. I couldn’t care less about the number because my TIR is where I want it, and I knew this would be reflected by a way-in-range A1c number. (I take no credit for it – it’s all Loop.)
But my kidney function? My cholesterol? My thyroid function? Coeliac screening? Everything else? I have no idea how they are tracking. There is no app on my phone to remind me how I going with those, or helping me guess what they me be. I have no Loop for my kidneys!
I realised that was the source of the anxiety, not my A1c, even though that’s where I was pointing. I guess that makes sense: feeling nervous about A1c results is expected and easy to explain. But the truth is that wasn’t my I was feeling uneasy.
Those complications screenings that I am diligently trying to make sure I have annually still terrify me. Both in the lead up to having the checks done, and then as I wait for the results.
The beast of diabetes that lives within our very core behaves in different ways. Often it is slumbering, lying almost dormant, lulling us into a false sense of all is well. I guess that is how I have felt since I started looping. I say that I am the least burdened I’ve ever been my diabetes because my diabetes is not thrashing around and making itself known so much. But this last week, it has started to wake, reminding me of its presence. I have felt diabetes more in the last week than I have in the last ten months.
I tried to describe this to a close friend the other day – a friend who has seen me live through some pretty horrid diabetes times, and celebrate some damn fine ones. She asks sensible questions and is always listening and learning. She gets it. But she struggled to understand how I could move from saying I’ve felt the best I have ever felt in relation to my diabetes to suddenly speaking of the anxieties that I hold so deep; especially when nothing had changed.
It’s the unknown. It’s the waiting. It’s the fear of what I may be told. That is the beast.
Today, the lightness in my step and in my heart as returned. The appointment went well, the results showed little, if any, change from the last screening checks. I am back to feeling the way I was before last week. After stirring, and stretching, the diabetes beast has curled up and resettled, and is hibernating again. At least, for now…

Waiting with diabetes
Yesterday an article was published across Australia detailing a new report showing that Australians with diabetes are missing out on the recommended levels of diabetes care. Most of these people receive their diabetes care in general practise.
A couple of things before I go on:
- The article was behind a paywall, but Diabetes Australia shared an image of a portion of the it, and that can be accessed here. If you have access to a News Ltd. account, you can read the article here.)
- I want to say that in writing this post today I do not want to be seen to be doctor-bashing. I don’t believe that is constructive in any way whatsoever. However, I do think that there needs to be acknowledgement that the level of diabetes care in general practise is not ideal for a lot of people.
- The language of the article was atrocious. It appeared first under the heading ‘How diabetes sufferers are dicing with death’ Seriously, journos, ready the freaking Diabetes Australia Language Position Statement.
Onwards…
There was some discussion online after the article was shared, with a few doctors believing the article wasn’t all that helpful and feeling that it was unfairly unfavourable towards GPs. Someone also commented on the language used. (I’m not sure if they meant on Twitter or in the article. The language in the article was strong and very critical of GPs.)
The report is damning, and it shows that the results for people with diabetes are not good at all with only one in three people diagnosed with diabetes receiving expected standards of diabetes care. Only half had their A1c checked, and of those, only half again were in range.
This is despite there being a documented diabetes annual cycle of care (for which GPs receive funding). If completed fully, the annual cycle of care includes: annual A1c, cholesterol, and kidney checks, weight and blood pressure checks, as well as two-yearly eye and foot checks.
For me, it shows yet again how stacked the decks are against so many people with diabetes. We don’t receive the level of care recommended and then, when we don’t meet expected outcomes, or develop diabetes-related complications, we get blamed.
If we want to talk about things that are unhelpful and not constructive, let’s begin with that.
We seem to forget that most people don’t innately know what is required to manage diabetes, or what screening checks are required – especially people newly diagnosed with the condition. A lot of people rely on their healthcare professional – in the case of diabetes, usually their GP – for this.
I’ve written before that in my case, my GP is not in any way involved in my diabetes care. This is a deliberate decision on my part. I understand it is also a privileged decision – I have easy access to my endocrinologist, and other diabetes specialists for all my diabetes healthcare needs.
But that’s not the case for everyone, and a lot of people are reliant on their GP for all their diabetes clinical care.
People with diabetes are being let down.
Even though pointing fingers and appropriating blame is not necessarily helpful, it’s what we seem to do. We can blame the system. We can blame a lack of funding. We can blame a lack of continuity of care. We can blame the fact that there are no coordinated screening programs. We can blame the need for more specialist care. We can blame a lousy and ineffective electronic records system.
But what we can’t do is blame people with diabetes. No one asks to get diabetes. No one asks to get diabetes-related complications. So how is it possible that in a system that is letting us down, we are the ones blamed when it happens?
Also, this week, we have heard story after story of missed type 1 diabetes diagnoses with people reporting that despite seeing their GP (often repeatedly) about their symptoms, they were not checked for type 1 diabetes.
It is undeniable that some GPs simply do not know enough about diabetes to diagnose it in the first place, and then to treat it in an ongoing and effective way, and this is leading to those of us living with it not receiving an adequate level of care to live as well as possible with diabetes.
While there may be some hard truths in the report, hopefully the result will be better care for people with diabetes. Because, surely, that is all that matters.

I wrote a piece last week about how nervous I was about a talk I was giving at the Victorian ADEA Branch Conference about my personal Loop experience. The conference was held on Saturday, and I did my talk and escaped unscathed. It’s a good news story!
Thanks to everyone who encouraged and sent me words of support before my talk. I decided that I’d come clean before starting and admit to the audience that I was feeling a little nervous because I understood just how contentious many may consider what I was about to say.
Having legendary CDE Cheryl Steele share the stage with me – and her story with the audience – certainly helped!
Here are my and Cheryl’s talks.
A reminder – I am not recommending using Loop. This is my personal story and my personal experience. If you would like more information, please search ‘Loop’ on the blog. (There’s lots here because I keep banging on and won’t shut up about it!)
Three days in Vienna is never going to be enough, and neither were three days at ATTD. But mother guilt is a very strong motivator for getting back home as quickly as possible.

This is the second ATTD conference I attended. Last year, I returned a little bewildered because it was such a different diabetes conference to what I was used to. But this year, knowing what to expect, I was ready and hit the ground running.
There will be more to come – this is the initial brain dump! But come back from more in coming weeks. Also, if you emailed me, shot me a text, Facebooked me, Tweeted me or sent me a owl last week, I’ll get back to you soon. I promise. Long days, and long nights made me a little inaccessible last week, but the 3am wake up thanks to jet lag is certainly helping me catch up!
So, some standouts for me:
DIY
The conversation shift in 12 months around DIY systems was significant. While last year it was mentioned occasionally, 2018 could have been called the ATTD of DIY APS! Which means that clearly, HCPs cannot afford to think about DIY systems as simply a fringe idea being considered by only a few.
And if anyone thinks the whole DIY thing is a passing phase and will soon go away, the announcement from Roche that they would support JDRF’s call for open protocols should set in stone that it’s not. DANA has already made this call. And smaller pump developers such as Ypsomed are making noises about doing the same. So surely, this begs to the question: Medtronic, as market leaders, where are you in this?

It was fantastic to see true patient-led innovation so firmly planted on the program over and over and over again at ATTD. After my talk at ADATS last year – and the way it was received – it’s clear that it’s time for Australian HCPs to step up and start to speak about this sensibly instead of with fear.
Nasal glucagon
Possibly one of the most brilliant things I attended was a talk about nasal glucagon, and if diabetes was a game, this would be a game changer! Alas, diabetes is not a game, but nasal glucagon is going to be huge. And long overdue.
Some things to consider here: Current glucagon ‘rescue therapy’ involves 8 steps before deliver. Not only that, but there are a lot of limitations to injectable glucagon.
Nasal glucagon takes about 30 seconds to deliver and is far easier to administer and most hypos resolved within 30 minutes of administration. There have been pivotal and real world studies and both show similar results and safety. Watch this space!
Time in Range
Another significant shift in focus is the move towards time in range as a measure of glucose management rather than just A1c. Alleluia that this is being acknowledged more and more as a useful tool, and the limitations of A1c recognised. Of course, increasing CGM availability is critical if more people are going to be able to tap into this data – this was certainly conceded as an issue.

I think that it’s really important to credit the diaTribe team for continuing to push the TIR agenda. Well done, folks!
BITS AND PIECES
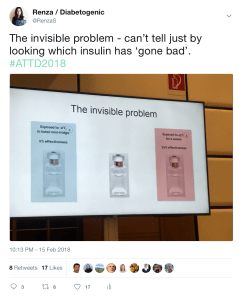
MedAngel again reminded us how their simple sensor product really should become a part of everyone’s kit if they take insulin. This little slide shows the invisible problem within our invisible illness
Affordability was not left out of the discussion and thank goodness because as we were sitting there hearing about the absolute latest and greatest tech advantages, we must never forget that there are still people not able to afford the basics to keep them alive. This was a real challenge for me at ATTD last year, and as technologies become better and better that gap between those able to access emerging technology and those unable to afford insulin seems to widening. We cannot allow that to happen.
Hello T-Slim! The rumours are true – Tandem is heading outside the US with official announcements at ATTD that they will be supplying to Scandinavia and Italy in coming months. There are very, very, very loud rumours about an Australian launch soon but as my source on this is unofficial, best not to add to the conjecture.
How’s this for a soundbite:

GOLD STARS GO TO….
Massive congrats to the ATTD team on their outstanding SoMe engagement throughout the conference. Not a single ‘No cameras’ sign to be seen, instead attendees were encouraged to share information in every space at the meeting.
Aaron Kowalski from JDRF gave an inspired and inspiring talk in the Access to Novel Technologies session where he focused on the significant role PWD have in increasing access to new treatments and his absolute focus on the person with diabetes had me fist pumping with glee!
Ascensia Diabetes packed away The Grumpy Pumper into their conference bag and sent him into the conference to write and share what he learnt. Great to see another group stepping into this space and providing the means for an advocate and writer to attend the meetings and report back. You can read Grumps’ stream of consciousness here.
Dr Pratik Choudhary from the UK was my favourite HCP at ATTD with this little gem of #LangaugeMatters. Nice work, Pratik!
ANY DISAPPOINTMENTS?
Well, yes. I am still disappointed that there were no PWD speaking as PWD on the program. This is a continued source of frustration for me, especially in sessions that claim to be about ‘patient empowerment’. Also, considering that there was so much talk about ‘patient-led innovation’, it may be useful to have some of those ‘patient leaders’ on the stage talking about their motivations for the whole #WeAreNotWaiting business and where we feel we’re being let down.
I will not stop saying #NothingAboutUsWithoutUs until I feel that we are well and truly part of the planning, coordination and delivery of conferences about the health condition that affects us far more personally that any HCP, industry rep or other organisation.
DISCLOSURE
Roche Diabetes Care (Global) covered my travel and accommodation costs to attend their #DiabetesMeetup Blogger event at #ATTD2018 (more to come on that). They also assisted with providing me press registration to attend all areas of ATTD2018. As always, my agreement to attend their blogger day does not include any commitment from me, or expectation from them, to write about them, the event or their products. It is, however, worth noting that they are doing a stellar job engaging with people with diabetes, and you bet I want to say thank you to them and acknowledge them for doing so in such a meaningful way.






