
You are currently browsing the category archive for the ‘Conferences’ category.
We got here. Thirty-two hours, four plane legs (thanks to an unexpected stop in Tampa due to thunderstorms closing Orlando airport), a kid who vomited her way through pretty much all thirty-two hours of the four plane legs, and hour and hours of low blood sugar somewhere over the ocean.
And now on my wrist is a bright green band. I’ve reconnected with friends I’ve known for years here and made new ones. And there are strangers by the pool with matching green bands and matching pumps hanging from their bathers.

My family are getting to know the Friends for Life family, being welcomed as warmly as I was when I first met everyone.
‘They look like diabetes people,’ said Aaron as we were walking around the lake the other evening.
‘How do you know?’ I asked him, wondering if he had developed a diabetes-detecting superpower.
‘She has a pump attached to her pocket,’ he said, nonchalantly.
And she was. I hadn’t even noticed.
It’s going to be a big, big week!
Follow ow along at home:
The Diabetes Hands Foundation MasterLab Summit – “A More Effective Summit’ is using #MasterLab and Friends for Life is at #CWDFFL15
One afternoon whilst in Boston, I left the confines of the Convention Centre so I could attend a DOC event. It was hosted by J&J and the event started with a two hour walking tour of Boston. This was a brilliant idea on so many levels, not least because it meant that I would actually get to see some of beautiful Boston and hear about its rich history.

Water taxi to work.
Boston is really a stunning city. Between the glimmering harbour, stunning architecture and cobble-lined streets, it’s a very pretty city to walk around. (Because, believe me, you don’t want to drive around it. The traffic is bloody horrendous!)
Our walking tour followed part of the Freedom Trail (read about that here). We made four of the sixteen stops on the walk. (Which only means that I now need to return to Boston at some point and do the whole trail!)

Some of the sights on our walking tour of Boston.
So, what do you really hate about your diabetes? was one of the questions. Not necessarily an easy question, but one that I jumped in to answer first. Because actually, for me, it has an easy answer. As much as I write about the crappy hypos, and difficult days with BGL swings resembling some sort of Himalayan mountain range, and the emotional side of diabetes, the thing I hate most about diabetes is never really far from the front of my mind.
I hate that it’s not just MY diabetes. I wish it were. But it’s not. I hate that it is also my family’s and friends’ diabetes. I hate that they know about diabetes and that they have to sometimes be a part of it – taking an active role in helping me. They don’t get a choice. And while they would never say this – and they probably don’t even feel it – I feel like I am a burden. I hate that my diabetes is also my husband’s and daughter’s and mum’s and dad’s and sister’s and in-laws’ and friends’.
I stopped speaking. Some of the others in our group were nodding. I can talk about diabetes a lot without getting too emotional. I can be pragmatic and direct. These are the facts – this is what it’s like. But when I talk about my family, I do get emotional.
I felt my eyes starting to sting and was glad that I had a pair of glasses hiding my tears. Not that it would have mattered had I openly cried. As I said, I was amongst friends and the only response would have been a huge hug. Possibly from this bloke:

The wonderful Scott Johnson.
Discussions about diabetes can be tough. But when you have kind, generous and understanding people around when having these discussions, it makes things just a little easier.
Thanks to the team at J&J who put on the walking tour and drinks afterwards for members of the DOC.
I am almost over my jet lag. I know: I’ve been back for two weeks now and I am still dealing with the effects of a messed up body clock. I expect that by next weekend, it will all be good and I’ll be fine again.
Which is terrific. Because next Sunday, I’ll be getting on another long haul flight and going back to the U.S. so I can go to Friends for Life (FFL).
I can’t tell you how excited I am about this. (The going to FFL part; not the long haul flight/more jet lag/perpetually messed up body clock part.)
I‘m more than thrilled to be given the opportunity to attend FFL. I have spoken to so many people who have gone and I get the same words from everyone: ‘It’s life-changing’, they all say. I have met Jeff Hitchcock from Children with Diabetes (who runs FFL) a number of times, and each time, I inevitably say ‘Jeff – how do we get this to Australia?’ Part of the reason I’m going next week is to see how indeed we could make that happen!
Because here in the wonderful land of Oz, we don’t have anything like FFL. Of course, we have camps for kids with diabetes and, in some states, family camps. In fact, just this weekend (and next weekend too), Diabetes Victoria will be hosting our annual family camps for kids with diabetes and one of their parents.
The difference with FFL is that is for the whole family – everyone! And it’s not just for kids with diabetes. Panreatically-challenged adults can go and take their family along too (including my little clan, which is making me explode with excitement!). This means that at FFL, everyone is considered – siblings, parents, partners, kids of parents with diabetes, even grandparents!
This completely subscribes to the It takes a Village idea. And the longer I live with diabetes, the more people I speak with who are affected by diabetes, the more I realise this is a truism like no other.
I am so happy that my family is coming along too. When it was decided that I should attend this year’s FFL, I knew there was no way that I could go without them. I was crazy if I thought the kidlet (and Aaron!) would ever forgive me for going to Disney World alone – even if it was for work.
So, I’m looking forward to joining the Friends for Life village next week, and adding my little tribe to it. It will even be worth the jet lag that will, undoubtedly ensue!
Consumer engagement. There are a couple of buzz words if I’ve ever heard them.
Today, I am attending the Health Issues Centre Forum, ‘Listening to the Consumer Voice: what does healthy dialogue look like in 2015?‘ I was the opening presenter where I spoke about the role of the consumer in healthcRe.
My position is clear – consumers have a place at every conversation taking place about healthcare. Whether it be at a governance, strategic or operational level, the voice of the consumer should be the loudest and proudest in the room.
All too often, this representation is tokenistic. It is an all-too-simple ‘tick-the-box’ requirement of health services. And it’s the same in the broader health community.
Most of what I have heard today I have heard before. This discussion has been going on for a long time, and as one of the speakers said ‘Why are we even having this conversation anymore?‘ And he is right. Why do we need to be defending the right of the consumer voice? Why is it not a given?
My talk was followed by palliative care physician, A/Professor Natasha Michael who gave a fabulous talk about the challenges faced by clinicians for finding the balance between ‘benevolent paternalism’ and patient autonomy.
Her analogy was simple – if she contracts an electrician to do some work for her, the last thing she wants is the electrician to stand in her house and ask ‘Where would you like me to put the green wire? And the red one? And the blue one?‘ They are the expert – that’s why she called them.
At face value, that sounds reasonable. But actually, I don’t think I really am comfortable with it because it completely minimises the expertise I have gathered in the 17 years I have lived with diabetes.
When I expect to engage in a dialogue with my HCP it is not discrediting their expertise; it is acknowledging that I have something to bring to the table.
At a higher level, consumer involvement can emote difficult. How are consumers included in strategic decisions, on boards and at a governance level? And how does that work?
Possibly my favourite take-home message from today came from Damian Ferrie who is the CEO of Inner South Community Health. Damian said that measuring if consumers are participating in a meaningful way is quite easy: ‘If consumers have no power to influence in your organisation, it’s tokenistic.’
I wish I could say that I am seeing more examples of consumers having power to influence, but that isn’t the case. Our involvement is still tokenistic. It is largely unpaid which further reduces our worth.
And yet, health services and health organisations claim frequently that they are listening to the consumer voice, that consumers are critically important, that consumers are the basis of their work.
By and large, I think it is lip service, with primarily examples of organisations talking the talk, but not walking the walk. And that is why we are still having these conversations. We need to be. I wish we didn’t. But we do.

It’s fan girl here again. I want to talk more about Bill Polonsky’s talk at the ADA meeting – specifically this:
 This point had me thinking. A lot. We speak frequently about how diabetes is an invisible illness. And it is a lot of the time. This piece I wrote for The Glow last year really resonated with a lot of people with diabetes who thought that it was such a good representation of what life with diabetes is about that it was shared almost 4,000 times.
This point had me thinking. A lot. We speak frequently about how diabetes is an invisible illness. And it is a lot of the time. This piece I wrote for The Glow last year really resonated with a lot of people with diabetes who thought that it was such a good representation of what life with diabetes is about that it was shared almost 4,000 times.
It’s invisible – we can’t see it. We rarely point to it. And you can’t walk down the street identifying the people with diabetes. (Although I like to think we sparkle a little brighter than the average person and have an aura of brilliance surrounding us, a rainbow above our heads and ride around on a unicorn. Just me?)
But I’m not sure that as a person with diabetes that I have ever weighed up the management aspects of diabetes against the (for want of a better term) return on investment.
ROI is such a big thing in our world. We expect some sort of return or reward for work we put in. Whether it be in our friendships or relationships or work or play. We do something and there is an underlying need to see something come back at us. We seem to expect acknowledgement or compensation and pats on the back for what we have put in.
There’s a problem with that expectation when it comes to diabetes. Because sometimes it doesn’t matter how much effort we put into our diabetes, the ROI is negligible. Not always – sometimes we see results and we can point to our efforts for the improvements. But sometimes – and unfortunately, a lot of the time – we get nothing back.
That all makes so much sense, so I’m not sure why I have never seen that before. Bill Polonsky’s point was such an ‘Aha moment’ for me. I went away and kept thinking about it and started listing the reasons I give for eliminating self-care tasks of diabetes. And they all came down to versions of ‘Because it doesn’t matter what I do, I still get crap results.’
Is it an easy excuse? Maybe. But I ask those without diabetes this: how inclined would you be to keep doing something if you got nothing back in return? It’s why people leave jobs, or relationships or other situations. Not feeling that you are getting something in return for your work? You can walk away.
Of course, we can’t leave diabetes. So how do we keep going – keep up with the hassles of self-care – when the ROI can be so minimal. I don’t have the answers to that one, I’m afraid. I wish I did. I really do.
Throw back Thursday to this post from a few years ago with a meme – 30 Things About My Invisible Illness You May Not Know. Most of it is still applicable today.
One of the highlight sessions I sat in on at ADA was Dr William Polonsky. Bill is the Co-Founder and President of the Behavioural Diabetes Institute, which you can read all about here. He also wrote the book Diabetes Burnout which is on the shelves of many, many people living with diabetes. I refer to it ALL THE TIME, and my copy has become incredibly dog-eared and annotated in recent times. And there was a period of about 6 months where I carried it around with me like a security blanket. (If you don’t have it, you can order it here.)
I’ve seen Bill speak at other conferences I’ve attended – he is one of the speakers I always make a point to hear because he absolutely ‘gets’ diabetes. His talks are always informative, amusing and offer great take-home messages for the mainly-healthcare professional audience. And he is gentle, kind and completely and utterly non-judgemental.
Yes – I am a complete and utter fan girl! But I did manage to keep myself together when I spoke with him a couple of times at the conference. And only slightly squealed when I heard he would be coming to Australia later this year. (Watch this space!)
His session at this year ADA had the title ‘Caring for the patient who doesn’t seem to care’ and right off the bat, Dr Polonsky highlighted the word ‘seem’ in the title.
He started by asking the audience how many of them had, in the past year, seen a patient who didn’t seem to care about their diabetes. Just about every hand in the room went up. Of course they did. Because for many – most? all? – of us living with diabetes, there are times when it all gets too much and we seem to not care.
But then he reminded everyone that even those who seem to not care about their diabetes want to live long, happy, healthy lives.
I don’t know anyone with diabetes – feeling good or not so good about their management – who isn’t hoping to be healthy. No one wakes up in the morning and says they want to have a crappy diabetes day. No one says ‘Diabetes is too much for me at the moment. I hope I have a really bad hypo.’ No one.
In times of burnout, where I absolutely know it looks like I couldn’t give a toss about my health, I wish so hard that I could find ways to break through the exhaustion and lack of motivation and find a way – any way – to do better at managing my diabetes.
Other take home messages from Bill’s talk included the importance of talking about diabetes with a sense of urgency – however without threats. I loved how he suggested a reframing of the oft-quoted ‘diabetes is the leading cause of <insert complication>’, reminding us all of the following:
Dr Polonsky’s take home messages from this talk were many. He provided some strategies for what might work – and some that should be avoided.
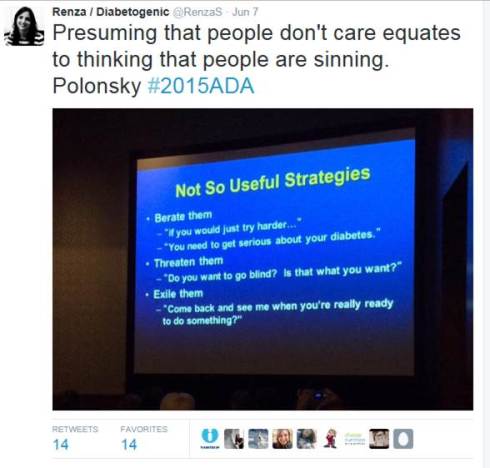
I listen to talks like this and think they sound so logical and sensible, and wonder why it even needs to be said. But of course it does. Because sometimes – all too frequently – there is this idea that not managing diabetes as expected is a deliberate choice. Or that not getting the results that we all ‘should’ be getting is the fault of the person living with diabetes. Thank you to Dr Polonsky – and others like him, including Martha Furnell, Jill Weissberg-Benchell and our very own Professor Jane Speight – for understanding that there is no fault here. Just a need for better understanding and support.

Being a total fan girl here! Dr Polonsky is my hero.
I’m back from the American Diabetes Association Scientific Meeting and I am pleased to report that the world hasn’t ended. Despite having in the same room, at the same time (and multiple times!), healthcare professionals, people with diabetes, industry and health organisations, the earth continues to rotate around the sun and we’ve not been plunged into the darkness of the apocalypse. I am relieved.
Actually, I’m totally not. Not at all.
There is much that we can be critical of when it comes to the U.S. health system. But their inclusion of consumers (patients, whatever you want to call us) at conferences is, from where I am sitting, enviable.
I cannot count the number of patient advocates in attendance at this year’s ADA conference. But we were everywhere. We presented, we attended sessions, we connected with each other, we tweeted the hell out of the talks we attended, we spoke with the aforementioned HCPs and people from industry and health organisations. We made plans for ways we could all collaborate and initiated projects that would cross seas and continents and provide support for other people with diabetes.
And the conference was all the better for it.
I return home to where there is, unfortunately, limited collaboration. When there is some sort of partnership or alliance, it is often tokenistic. Frequently, these are the words I hear when a collaboration is first suggested ‘We’ve been told that we should speak with people with diabetes about this project/resource/activity/ program. We’ve been working on it for months/years/decades now, so we think it’s time we brought in someone with diabetes to tell us what they think’.
Let’s be clear: that’s not a partnership. That’s a ‘Shit, we forgot to talk to the people this is meant for. Quick. Do it now. Then we can say we’ve consulted.’
Well, no. Not really.
At our annual scientific meeting here in Australia, you will not see a consumer contingent. There may be a few rogue people there who manage to get by all the rules and regulations because we work in the diabetes field. But by and large, we are a rare sighting. This is, of course, partly due to the Therapeutic Goods Act which prohibits direct marketing of prescription medications to consumers. We are not free to wander around expo halls with the name of drugs in our faces. It is not considered appropriate that people with diabetes attend the sessions aimed at HCPs for fear that we would misconstrue or misunderstand or misrepresent what we are hearing.
But never in my time of attending an event where consumers are welcome have I seen that.
I attended the ADA Meeting to hear about the latest in diabetes. I wanted to go to sessions and hear from speakers about breakthroughs and research and studies that aim to improve the lives of those of us with diabetes. And I did. I spent a lot of time in those sessions. I spoke with the presenters afterwards and felt welcome and included. I asked the speakers when they would be in Australia and made them promise to do consumer talks when they get here – not just talks for HCPs.
And I also spent time speaking with people from industry and hearing about in-development products. I heard about the processes in the US and in other places for subsidies and asked about how they have gone about improving access to their technologies. And I begged that when they say that they have a global team working on something that they remember Australia – reminding them that we may be a long way away, but we are still part of their market.
And I did all this alongside other advocates. It’s amazing how loud our voice becomes when we are together.
DISCLAIMER TIME: Whilst in Boston at the ADA Scientific Meeting, I attended sessions funded by: Medtronic Diabetes: Johnson and Johnson Diabetes and Dexcom. I did not receive any financial (or other) remuneration for attending these sessions.
A couple of years ago, when CGM was first launched into Australia, the typical thing happened. The device company took their shiny new product to health professionals around the country, showing off their wares. There were dinners and events and showcases, all highlighting the new technology.
Now, obviously with a product like CGM which requires HCP initiation, it is important to promote the product to the people who will be getting consumers hooked up. I understand that.
Nonetheless, it was with much envy that I saw HCPs being given a trial of the product. They were connected to a CGM and given an empty pump for four days – the number of days a sensor was meant to be worn.
I was desperate to get my grubby hands on one of these. I had read all about CGM and how much people with diabetes living overseas loved it. I read about how it made people feel safer and less frightened about hypos. I learnt that it helped to level out …well…levels. It sounded exciting. I wanted to try it myself.
The HCPs on the trial I spoke to were incredibly dismissive about this technology. Over the few days they were wearing it, I heard comments such as ‘It’s making me obsessive’ or ‘I can’t stop looking at the pump and watching what’s going on’ or ‘When I calibrate it, the numbers don’t match exactly’ or ‘The infusion set insertion process is terrible. I bled everywhere!’
I heard them say repeatedly that the technology was rubbish, that it wasn’t worth the cost, and that all it would do for people with diabetes is make them more distressed and anxious about their diabetes. Plus, it hurt.
Not one of them had diabetes themselves.
I started to get annoyed. I recall sitting with one of them after hearing this pronouncement yet again, feeling quite angry. ‘You know,’ I said. ‘You don’t get to say these things. You don’t get to write off this technology after a few days of wearing it, making claims that it is pointless. This is the latest technology that we have to manage our diabetes. It’s first generation so of course it’s not perfect. The second, third and probably even fourth gen products probably won’t be perfect either. But it is a new and worthwhile tool to help us manage our condition. It is exciting. We are hopeful. You don’t get to trash it.’
I remembered this whilst siting in a session on the first day here at the American Diabetes Association Scientific Meeting. It was a ‘Meet the Expert’ session and the topic was about personal experiences of the artificial pancreas.
Kelly Close (she’s amazing – read all about her here) was talking about her experiences of being involved in trials for a couple of different artificial pancreas projects. It was fascinating hearing about the AP and her excitement about the current technology being trialled – and about what is still coming.
Her enthusiasm was obvious. In fact she actually commented on why enthusiasm and excitement need to be employed when talking about advances in technology. We need to create a buzz and have people talking and asking questions and going on trials and writing (and blogging) about our experiences.
On the panel with Kelly was Chris Aldred (better known as The Grumpy Pumper) whose role in the session was to be the one challenging all the hype. He immediately explained that he had not used the AP, and had some questions. He was skeptical about a few things.
Being skeptical is absolutely okay. We shouldn’t ever blindly accept any new treatment without asking questions, but that actually adds to the buzz. It forces people who have experience with the device to talk about the good things and its limitations. It also helps alleviate a lot of the concerns people may have.
I thought back to my experience with the launch of CGM back home. When the HCPs who were privileged to try the then-new tech were trashing the product, I wish that there had been a voice to be able to respond to those concerns. I wish that the trial of the product had been extended to people with diabetes who could see it for what it was and how its application worked in the real world. And who could share their experiences – absolutely the good and the bad – with other PWD.
That’s exactly what I did when I finally got to try CGM. You bet the first gen was clunky. It did have accuracy problems and I did bleed a little most times the sensor was inserted. But whoa! It was amazing technology for the time and made a huge difference to me. When I understood how the trends worked, I knew how to respond to them. I could address things before they became problems.
I left the AP session on the first day pretty excited and inspired. And wanting to be part of the buzz – either as a trial participant or as someone on the periphery talking about it, reading about it, hearing people speak about it.
Read more at diaTribe where Kelly shares her AP trial experiences.
‘Are you here for work?‘ It was just after 7am in LA, and the border security officer looked tired. He studied my passport, holding it up, comparing the photo with the even-more tired-looking, and rather dishevelled, person standing in front of him.
‘Yes. For a conference in Boston.‘ I said, trying to smooth my hair.
‘Oh, the diabetes one?’
‘Yes. That’s right.’ I said. My flight from Melbourne was full of people attending the ADA conference. I know this because I knew half of them. Plus I kept hearing snippets of conversation with ‘diabetes’ being thrown around.
‘My mum (mom!) has diabetes. Type 1. She should go.‘ He said. He flipped through my passport. ‘How long are you here for?’
‘Only for the conference and then three days in New York. I’ll be home in nine days.’
‘That’s not long after travelling so far,’ he said to me.
I smiled. ‘You’re so right. But I’ve left my family home this time. So I don’t really mind only being away for a short time.’
‘Enjoy the conference.’ He stamped my passport and was about to hand it back to me when he looked at me again. ‘Do you have diabetes?’
‘Yes. I do,’ I said. ‘I have type 1. Like your mum.’
‘Do you use a pump?‘ he asked.
‘Yes. And I’m wearing a CGM as well.’
‘My mom needs to talk to you,’ he said. ‘You look healthy. Keep it up.’ He passed me my papers.
‘Thanks. I hope your mum is okay,’ I said, noticing the concerned look on his face – one frequently worn by loved ones of people with diabetes. He nodded and I walked off, heading towards the baggage carousel.

A typical, frantic, ‘I’m so disorganised’ few hours before getting to the airport. But I have insulin. And I have a CGM fastened to my stomach and an insulin pump tucked in my bra. There are pump supplies in my carry on. Anything else I’ve forgotten can be found easily at the other end.
Don’t forget to follow #2015ADA!






