
You are currently browsing the category archive for the ‘Awareness’ category.
The diabetes online community is a truly global network. We see that every week in tweetchats and anytime we log onto social media. We know that connections are made that are life changing and, (as in the case of my dear friend’s ‘Pumpless in Vienna’ story – to be told here soon), life saving.
For the last three years, I have been privileged to attend the European Bloggers Summit, which is a satellite event run alongside the EASD Scientific Meeting. This event is a chance to really look at ways that consumer advocates can work together and support each other to make significant change to living with diabetes.
It was sobering to be reminded several times yesterday that those of us sitting behind our laptops, participating in the dialogue of the community are already very lucky. We looked at programs out there that are providing insulin to people who would not otherwise have access. Again – life saving.
The beauty of these events is that they are not simply a day or two of navel gazing and patting ourselves on the back for the work we do. We challenge ourselves and each other to do more, do better and reach more people. We plan for what we want to achieve and then hold ourselves accountable for what we have said we want to deliver.
The issues that we have in Australia and that I frequently write about right here are so often universal. Hearing friends from Europe say that the language of diabetes is an issue, or access to technology or medicines is prohibitive for some, reminds me that it is worth continuing to be in this space. When I hear about the frustrations experienced by others when it comes to consumer representation, I know that every time I say ‘nothing about me without me’ it is echoed around the world.
There are some amazing things going on, and over the coming weeks I’m going to write about some of the things I learnt about because I not only want to share this work, I also want to encourage others to get involved.

DISCLAIMER
The 2015 European Bloggers Summit was sponsored by Johnson & Johnson. I was invited by Johnson & Johnson to attend the event and did not receive any funds from Johnson & Johnson to cover travel or accommodation costs to Vienna or to attend the EASD conference. These costs were covered by my employer, Diabetes Australia – Vic.
Yesterday, I sat in meetings, listened to talks and attended press briefings. The EASD conference is shaping up to be a very busy one and I am doing my best to get to as many things as I can whilst still making sure I get to catch up with as many online community people as possible.
And thank goodness for those people; for the people I’ve seen in person at the conference and for being able to sit in for a very short while on this week’s OzDOC tweetchat.
These conferences are critically important for a number of reasons. They bring together the biggest and brightest people who are most admirably working to improve the lives of people living with diabetes. These are minds far smarted than mine – they are amazingly brilliant professionals. I admire them on many, many levels.
But too often I get the feeling that people with diabetes are lost in the messaging and completely forgotten. The language being used has us as passive ‘subjects’ (thank you to Professor Richard Holt (@RichardGHolt) for your tweet, by the way!), not involved in what’s going on. It’s kind of like these conferences are a magical land where diabetes is spoken about as a thing on its own, forgetting that it is always attached to actual real people living actual real lives in the actual real world.
One meeting I sat in today listed ‘key stakeholders’ involved in a new ‘patient’ education program. The glaring omission in this esteemed list was people with diabetes.
In another session, the speaker was complaining about the inability to get accurate data from device companies about ‘patient opinion’ of their products. There seemed to be a complete lack of thought that perhaps people using those devices might be able to provide the information being sought.
In both sessions, I thought about standing up and saying something, but you know what? Sometimes I get sick of the sound of my own voice saying the same things over and over.
This is not where I say that people with diabetes need a seat at the table of organising committees and advisory boards. Because I say that all the time.
No.
This is where I remember that it is up to us to cut through the noise, ignore the fanfare and the superfluous crap (of which there is much) and try to find the things that are actually going to make life with diabetes a little – just a little – bit easier. It’s there – it’s being spoken about and there are glossy brochures promoting it.
It’s just that the wrong people are being spoken to.
I got up close and personal with the new Abbott FreeStyle Libre system today, getting to see it in action on a representative from Abbott. Despite begging, pleading and promising to not tell anyone (except, of course, the pretend people who read this blog), I was unable to get any details about an Australian release date. Social media musings, however, suggest that we are looking at early next year. Watch this space!
Last week, there was a very interesting infographic doing the rounds on social media sites about where people donate as compared with the diseases that kill us.
It looks like this:
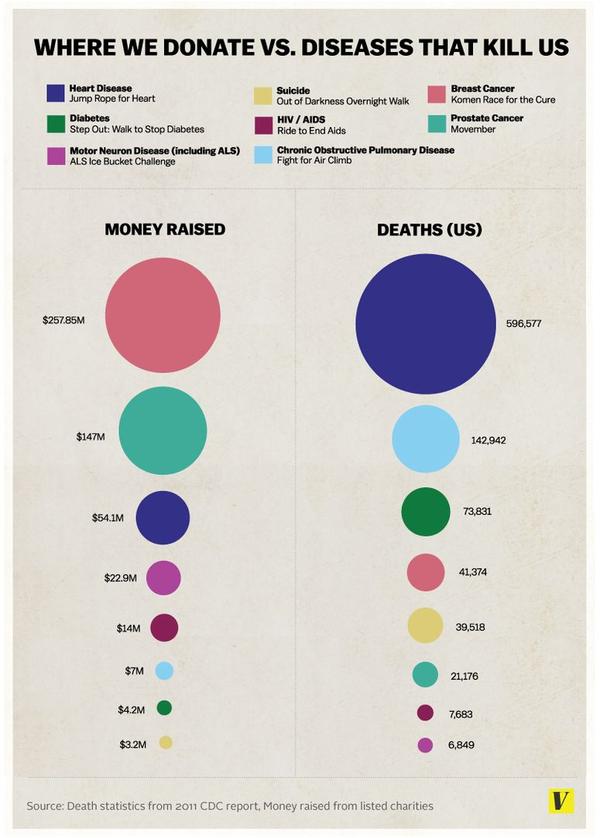
As you can see, diabetes is credited with causing the third most deaths, yet it accounts for relatively little money raised.
Firstly, this isn’t a game of ‘my health condition is worse than yours’. As someone most eloquently wrote on a Facebook status the other day: ‘all diseases suck’. Equally, every single condition is worthy of people’s donations. There simply isn’t enough money to go around to do the research, run the programs and assist people dealing with whatever health condition they have.
But I think unpacking why some conditions attract more donations than others is worthwhile.
Despite being responsible for many, many deaths and affecting millions of people both here in Australia and around the world, diabetes just doesn’t seem to be the ‘disease of choice’ when people reach into their wallets to make a donation.
Why is this? Why is diabetes not at the top of people’s minds when they want to do some good?
I’m just going to say this.
Diabetes isn’t sexy. It’s really not. It’s chronic; there’s no cure; and while there is the cute factor when we’re talking about little kids with type 1 diabetes, they grow up. And then it’s just boring adults with boring diabetes.
But there’s more than that.
The media does a great job of stigmatising this condition. Plus, there’s the ‘you did this to yourself’ misconception that means it’s okay to blame people for developing (type 2) diabetes in the first place and ‘…why the hell should I donate to you. Get off the couch and go for a walk’. Helpful. Really, really helpful.
Diabetes needs a makeover. Plain and simple. We need people in the general community to change the way that they currently think about diabetes so when it’s time for a little generosity, they consider making a donation to diabetes research or consumer organisations.
The neat little packages we seem to have about diabetes are misleading. Tying up type 1 with kids means that adults with type 1 have no voice at all. Blaming all people with type 2 diabetes for ‘doing this to themselves’ completely forgets the facts that genes play a significant role in developing type 2 diabetes. Calling diabetes ‘a touch of sugar’ ignores the seriousness of everyday life with diabetes. In fact, the very idea that this is all about eating sugar results in such misunderstanding about diabetes that people think the solution is as simple as not eating cake. The misconception that insulin is a cure ignores the multitude of factors that are involved with the daily management of this condition. And by thinking it is just about sticking needles into our bodies negates the distress and anxiety life with diabetes can bring.
I don’t know what the answer is. But I do know that what we’re doing at the moment isn’t working. Our messaging is wrong. How do we get it right?
As always, the internet is a trove of …well, cat pictures, naked photos of celebrities and silly cures for diabetes. But there is also some other stuff. You’ve just gotta look.
A Case for Action
As mentioned, I was in Canberra on Wednesday for the launch of a new Diabetes Australia report on insulin pump therapy. You can read Insulin Pump Therapy; A Case for Action here.
ADEA Video wrap-up
The people from online magazine Diabetes Educators Update have put together a short video wrap up of last week’s ADS-ADEA conference. It was nice to be asked about whether HCPs need to consider the consumer perspective.
Try to overlook the questionable language – (diabetes sufferers’???) – I’ll be sending them a copy of the DA Language Position Statement soon.
Use words wisely
While we’re talking language, this tweet from Kim at www.txtingmypancreas.com really resonated:

It’s why I don’t say I’m ‘battling’ diabetes. I’m living with it. We co-exist (not always happily). There is no fighting; there is just learning to get along.
On yer bike!
Have you been following Team BG doing the mHealth Grand Tour? They have been making their way from Barcelona to Vienna. On bikes. Because they’re slightly crazy. The photos are gorgeous and I have to admit I’m a little in awe of their sportiness. Go team! I’ll see you in Vienna.
Let it go ON!
We need to talk about Frozen because pretty much everyone else on the DOC has been. This week in the US, a documentary about the making of Frozen was screened. As it turns out executive producer John Lasseter based much of the character of Queen Elsa on his kid with type 1 diabetes. I love this character for so many reasons and now, I have another one. I’m not sure that we’ve had many ‘Let it Go’ free days in our house since we first saw the film, and now I don’t care if it’s played every single day for the rest of my life! Here’s what John Lassiter had to say:
Not our turn
‘We need an ice bucket challenge for diabetes’. I’ve heard this said so many times over the last few weeks from people affected by diabetes. It’s not a sentiment I share, because this particular social media-driven stunt doesn’t belong to us. Moira McCarthy has a daughter with type 1 diabetes and wrote this incredibly eloquent piece about how the diabetes community should be able to celebrate this for the ALS/MND community.
Moira wrote in the piece that her daughter with type 1 asked this question: “Why can’t our community be thankful another community is having success? Why isn’t that enough?”
Our turn will come. But for now, I think we should step back, support this community and this campaign however we see fit and be pleased for their success. (For the record, you can just donate – you don’t need to pour ice over your head; it’s bloody freezing still in Melbourne!).
MedX
The Medicine X (MedX) Conference for 2014 has kicked off at Stanford University. This conference is all about the future of medicine and healthcare and there is considerable consumer (patient) involvement. There are some familiar faces in the speakers’ gallery. Follow along on Twitter here.
Noodle
We have a new puppy. And she is the cutest thing ever!

Happy Friday! It’s Fathers’ Day on Sunday. This is for the three men for whom I get to celebrate this day.
Diabetes MILES Youth
Are you the parent of a child (aged 10 – 19 years) with diabetes? Then we need YOU! And your child with diabetes too.
You may remember that a few years ago now, the Diabetes MILES survey was conducted. Diabetes MILES looked at the psychological health of people living with diabetes, and the survey results continue to be collated and presented.
Now, a new study – Diabetes MILES Youth – is being conducted asking young people about what it’s like to live with diabetes, and how diabetes affects their wellbeing.
And because we all know that diabetes is a ‘family sport’, parents of kids with diabetes are also being asked to complete the survey.
The survey is only open until the end of September, so please take the time (about thirty minutes) to respond. (I know that you would get involved anyway, but as an added incentive, there’s an iPad to be won!)
Diabetes MILES and now Diabetes MILES Youth will actually show just how diabetes affects our lives on a day-to-day basis. The more we can talk about the psychosocial side of diabetes – the more evidence there is to show that diabetes affects our wellbeing – the more that diabetes stops being just a numbers game. (Although, in this case the number of people completing the survey is important, so get clicking!)
DISCLAIMER
Diabetes MILES Youth is part of the NDSS-funded Young People with Diabetes National Development Project of which I am the Project Manager. I’m writing about it here because I think it’s really important for as many people as possible to take part in this survey and have their voice heard.
The survey is being conducted by the Australian Centre for Behavioural Research in Diabetes.
If you’re on social media, you’ll be more than familiar with the ridiculous clickbait style articles that tell you about ‘things you should know’. These lists are often targeted to specific age groups (20 things all women in their twenties should know), gender (5 things men should do on a date) or include things to make you feel like you’re falling behind (23 things your daughter should know by the times she’s 13 years – subtext: and if she doesn’t, you’re a lousy parent).
The aim of these articles is to make the reader feel inadequate and feel that they are failing at things because they are 34 years old and haven’t worked out the 10 things every woman should know about orgasms.
I steer clear of any of these lists and simply don’t give in to the desire to click. So, here’s my list of 16 things every person with diabetes should know:
- Diabetes sucks.
- Diabetes can also be interesting and eye opening.
- Finding a healthcare professional who understands you and what you need will make navigating the system easier. And it’s perfectly okay if you want someone to ‘tell you what to do’ rather than someone who is more consultative. Horses for courses.
- Cinnamon doesn’t cure diabetes and anyone who says it does is a big lying liar. And possibly a bit simple.
- There is no unsuitable response to the question ‘should you be eating that’. Gentle violence is acceptable, as are tongue lashings, death stares and bursting into tears.
- Further to number 5 – yes, you can eat that.
- Cupcakes with sprinkles make as suitable a lunch for a person with diabetes as a person without diabetes.
- It’s perfectly okay to squeal when you see another person pulling out an insulin pump, giving themselves a shot of insulin, or checking their BGL. Even if you don’t know them.
- You do not need to explain your diabetes to anyone. That includes how you choose to manage it, how you feel about it, what you say about it. Your diabetes; your rules.
- I’ll just say that again: Your diabetes; your rules.
- There is no room for judgement. From anyone about anyone. (Except for people who wear leggings as pants. I’m all for judging them. And the Kardashians.)
- Unicorns are real – I rode mine to work this morning.
- Feeling sad or happy or down or ecstatic or miserable or pissed off about diabetes are all reasonable emotions – even within the same five minute period.
- It’s okay to grieve. Life with diabetes is different.
- There is no substitute for a friend with diabetes saying ‘I get it’.
- Lists about diabetes are stupid
Last month, I wrote a piece for Mamamia’s health and beauty sister site, The Glow. I wrote about how diabetes is sometimes referred to as an invisible illness because often there are no obvious, outward signs that say ‘I live with diabetes’.
This week, there’s been a lot of talk about another invisible illness – depression. I don’t even know where to begin writing about mental health. But I should be – we all should be. And we should be talking about it. A lot.
Not everyone is comfortable talking about their health conditions – whether it is diabetes, cancer, MS or depression. Perhaps there is more ‘acceptance’ of some conditions when compared with others. I know that when it comes to diabetes, the stigma and judgement can be exhausting. I expect that for those living with depression or other mental health conditions, the experience would be similar.
The invisibility of conditions like diabetes or depression is perhaps what terrifies me the most. Being able to conceal what is going on means not getting the support that may be needed. Not everyone knows how to ask for help. Not everyone wants to ask for help.
I am more than happy to talk about my experiences. Many others are too. And when I write about things that I am finding difficult, I feel enveloped with care, support and love. But what about those who don’t? What about those who are keeping things hidden from their loved ones and friends and colleagues?
Should we be more worried about the person who is getting up every morning, going to work and interacting with their colleagues, but has not shared their struggles? Last year, when I wrote about RUOK day, a very clever person (who may or may not be my sister) commented that it’s important to remember those who may appear ‘fine’. She’s right. We don’t think about those people enough.
I don’t have answers for any of this. The death of the magnificent Robin Williams has people talking. How do we keep the discussion going? How do we give people who need help the avenues to ask for it without feeling they will be judged? How do we stop people from taking their lives because they see no other way out? How do I say ‘how can I help’? How can I help?
“Depression is the most unpleasant thing I have ever experienced. . . . It is that absence of being able to envisage that you will ever be cheerful again. The absence of hope. That very deadened feeling, which is so very different from feeling sad. Sad hurts but it’s a healthy feeling. It is a necessary thing to feel. Depression is very different.”
-J.K. Rowling
It’s Friday and I could only think of this clip for this week.
‘You have brittle diabetes,’ the diabetes educator told me, regret in her voice.
Brittle. It’s such a sharp sounding word – all edges to cut yourself upon.
I first heard the term ‘brittle diabetes’ about three years after I was diagnosed. It was handed to me as a grave diagnosis within a diagnosis. Not just diabetes for me. I had brittle diabetes. I heard it, thought about it, said the words a few time together, jarring at the sound.
I was given this ‘diagnosis’ during a really rough period. My diabetes was all over the place thanks to a totally unrelated stomach issue. There were thoughts it may have been gastroparesis or, for a moment there, thanks to the significant weight loss I was experiencing, an eating disorder.
I became terrified to eat because every time I did, I was in extreme pain. At times I threw up everything I ate, other times I didn’t. My blood sugars were all over the place and the delightful insulin regimen which at the time involved Protophane was incredibly hopeless at doing anything other than send me plummeting low, or sky-rocketing high. It was a very tough few months.
I was seeing doctor after doctor after doctor. And all anyone could think about was my diabetes. My brittle diabetes. I was told: ‘This is what your diabetes is like. Sometimes there are no answers and we can do nothing to better manage things. This is it for you.’ There was an undertone of ‘get used to it, love’.
I wasn’t prepared to just accept it though. I wanted to have a baby and I knew that there was no way that I could even consider going down that path while my health was all over the place.
I finally sacked all the health professionals I was working with and sought out someone – something – else. I refused to believe that this was how I was going to be forever. I knew there were answers; I just didn’t know how to find them.
I found a new endo and when I walked in I told her that I had brittle diabetes. ‘I can’t be fixed, apparently. Give me everything you’ve got!’ I thought silently.
‘I don’t like that term,’ she told me gently. She wasn’t rude about it; she just explained that she thought we could work out why things weren’t going so well. And then, she went about finding answers. And we found them.
It took time and it took a lot of thinking outside of the square. It took putting diabetes to the side and not thinking that it was the only reason for all my health problems. Once I got sorted and my stomach was sorted and I spent some time talking things through, my diabetes was much easier to manage. I know that a big part of getting through was not only addressing the physical side of things. There were mental health issues I needed to address, mostly dealing with the grief I was experiencing about having to let go of my life before diabetes.
I too came to not like the term ‘brittle diabetes’. When I hear it now, I want to ask what else is going on. And I can’t help wonder where I would be now if I had just accepted that as my lot in diabetes.
Want more? Mike Hoskins wrote this interesting post on Diabetes Mine last year.
So much going on. So much to do. So much to plan. So many presentations to write.
So….naturally, I’m surfing!
BIONIC
I’m still really excited about the Bionic Pancreas. I know that when we hear of new research it’s often about mice, labs, five years’ time etc. So hearing and reading about the ‘real-life’ applications of this technology has been so very exciting. And hopeful. I interviewed someone who participated in the Melbourne trials (you can read about it in the next edition of Conquest). And for another beautiful, goose bump-inducing read about it, here’s what Kerri wrote at Six Until Me.
BLUE CIRLCE APP
A couple of months ago, the IDF launched a new photo app to help raise awareness of diabetes. You can add a blue circle to any photo and then share on social media. Here’s my latest masterpiece:
ZOE BOWIE SINGS
Earlier this year, I sat on a Google Hangout panel with Jamie Tripp Utitis who recently presented at the Doctors 2.0 and You conference in Paris about her beautiful new book ‘Zoe Bowie Sings, Despite All Sad Things’. Jamie wrote this book for kids with a parent with MS. Jamie writes an awesome blog of her life with MS. You can read it here.
WHERE ARE THE PEOPLE?
I threw a huge tantrum let out a huge sigh of defeat when this appeared in my (virtual and real) inbox today. It’s the promotion of a conference in Melbourne later this year about the future of primary care. One of the focuses is patient outcomes. Looking through the myriad speakers what do I find? Not. A. Single. Patient. In. Sight.
SCRIBBLES
Mike Lawson (who I was lucky enough to meet briefly at year’s ADA conference) recently started ‘Scribbling My Life Away’, a blog of his drawings. It’s not really, diabetes-related (although there is the occasional diabetes reference) but nonetheless very cool. (And, Mike, if you’re reading this, can you please do me a scribble of a jar of Nutella and a big spoon. I’d like to put it up in my office?)
SWEET PRETTY THINGS
Totally, completely and utterly not diabetes-related, but I can’t stop looking at the gorgeous artwork of Aussie Illustrator Kerri Hess. I am trying to work out how I could commission a life-size piece that would fit perfectly on a big blank wall in our bedroom.
MEOW
In other news, a cat café opened in Melbourne this week.
CRAZY BIKE RIDING TYPE 1 PEOPLE HEADING TO VIENNA
Last year a group of mad folk with type 1 diabetes rode from Brussels to Barcelona as part of the mHealth Grand Tour. Not content with this achievement, the group known as Team BG, will be doing it all again, kicking off in Barcelona and heading to the location of this year’s EASD conference, Vienna, where I intend to greet them and call them all crazy. I might then buy them a beer.
HAVE YOU REGISTERED YET?
A reminder that TODAY IS THE LAST DAY to get the early bird rate to attend the first ever ADS-ADEA Consumer Outreach program. Book now!
How often do you think about diabetes in a day? In an hour?
On those days that I think of diabetes about once an hour (when awake), I know that I’m doing okay. That may seem a lot, but it could be because I’m checking my BGL, bolusing for something I’m eating, doing a line change, thinking about eating something, making something to eat, about to drink a coffee with added sugar. It could be when I am getting dressed in the morning and remembering to reconnect my pump or pulling my pump out from my bra to check my CGM.
Sometimes they are passive thoughts, other times deliberate and actioned.
When this is my activity level, I know that I’m tracking okay.
But when I go for a few (say 4 or 5) hours or even a whole day without thinking about diabetes, I know I’m not tracking quite so well. On those days, I don’t check my BGLs, I don’t check what my CGM is telling me (maybe because I’ve not got a sensor in, maybe because I just can’t be bothered), I may not be eating particularly well or at all, so don’t bother bolusing. Sure, I passively thought about diabetes when I stepped out of the shower that morning and reconnected my pump, and perhaps I blind bolused for the sushi roll that made up lunch, but that could be my entire day of diabetes ‘chores’.
And equally, if I’m thinking about it more than once an hour, I know that something is not quite right. It could be that I’m high and trying to manage that by checking my BGL every 10 minutes hoping for a drop – even a teeny tiny drop – in numbers. At the same time, I’m anxiously trying to walk the tightrope that is enough insulin to bring me down from the hyper ledge, but not rage bolus and send me crashing. I’ll probably be starving, so I’ll be thinking about food and calculating carbs and making deals with myself as to what my BGL has to get to before I can eat.
Or, I could be low and trying to deal with the pounding heart rate that is a doof-doof reminder of my hypo-state. Probably over-eating, I’ll be checking my BGL every five minutes, looking for an upward trend in my numbers.
Either way – high or low – I’ll be thinking food, numbers, hoping for balance, worrying about over-treating, over-medicating.
It’s such a fine line.
Too much…
Too little…
Just right.






