
You are currently browsing the category archive for the ‘Real life’ category.
Earlier this week, Professors Jane Speight (ACBRD) and Frans Pouwer (Southern Denmark University) published a blog post on the ACBRD site, with their wrap up of EASD, specifically, the lack of psychosocial sessions at the conference. In the piece, Jane and Frans quite rightly say:
‘Psychology is not an optional extra. If diabetes care is the seat of a three-legged stool, then it is supported by three legs: psychology/education, treatment/technology and complications screening. It seems ironic that so much funding, resource and effort is put into strengthening and promoting the treatment/technology and complications ‘legs’, while the psychology/education ‘leg’ remains short and weak.’
EASD is the largest diabetes meeting on the calendar this year. It draws a truly international audience, with healthcare professionals and researchers from all disciplines. It is possible to speak with endocrinologists, diabetes educators, allied health professionals, general practitioners, psychologists, and researchers from all spheres of the diabetes care spectrum.
And yet, it is undeniable that the conference has a true clinical focus, almost forgetting that diabetes does not only impact specific parts of the body (so, so much about the ‘diabetic foot’!) but the whole person (absolutely not enough on the ‘diabetic mind’!).
I am not for a moment saying that the scientific and clinical elements of diabetes should be removed from a diabetes conference, or that they are not important. But I am saying that by demonstrating ONLY this aspect of diabetes, the picture presented is very, very incomplete.
I have written before that this is a frustration of mine at EASD, along with the continued lack of ‘patient representation’ on the conference program. It astounds me that there are no advocates on the official program, giving the ‘lived experience’ standpoint to what is being discussed. With hours and hours of sessions focusing on complications, how valuable it would be to have a PWD who is living with complications standing up there to give a little perspective to all the science. And a psychologist to speak about how complications affect far more than the part of the body that has become…well, complicated.
I urge the organisers and program committee to step up, and find a way to fill in the gaps and start to present a far fuller and more complete picture of diabetes.
While this would involve including more focus on the behavioural side of diabetes with the relevant professionals on the program, it must also mean including PWD into the program – in a meaningful way. If it is too much of a leap to include PWD alongside HCPs in the scientific program, introduce a Living with Diabetes Stream as the IDF has done in their last four World Congresses. It can be done. It can be done well. (And I say that with full disclosure that I am leading the stream at the 2019 Congress and was deputy lead for the 2017 Congress, and spoke at the 2015 Congress in the LWD stream.)
The thing is, it would actually be very, very simple to include PWD in the EASD program because we are already there. This year in Berlin marked the seventh EASD conference I have been fortunate to attend. I have always gone because of satellite events designed specifically for PWD. Initially, these were run by Johnson & Johnson, and more recently Roche, who has taken the ‘patient engagement’ to a new level, running events with up to seventy bloggers. That’s seventy people who have a story to share about their own diabetes experiences.
And I know that many of those seventy people would want to talk about all aspects of living with diabetes, including the psychosocial impacts.
As a leading annual diabetes meeting, EASD could be better. It ticks a lot of boxes. But it could, quite easily, tick a whole lot more by being far more wholistic in its approach. Focus more on the behavioural side of diabetes. And have PWD front and centre where we belong. After all, we’re the ones all this information and research is meant to be benefitting.
DISCLOSURE
Roche Diabetes Care (Global) covered my (economy) travel and accommodation costs to attend their #DiabetesMeetup Blogger event at #EASD2018 and present at their media event the day before EASD. Roche Diabetes Care also assisted with providing me press registration to attend all areas of the EASD meeting. As always, my agreement to attend their blogger day and participate in their media event does not include any commitment from me, or expectation from them, to write about the company, the events or their products.

With Jane Speight at EASD in Berlin.
I’ve been thinking a lot about motivation recently; specifically, how we remain motivated living with a lifelong health condition that places so many demands upon us. It’s something I also get asked about a lot by others with diabetes – often people newly diagnosed: ‘How do you stay so motivated.’
It’s all smoke and mirrors, because the truth of the matter is that most days, my motivation to ‘do diabetes’ is very low. In fact, I think that there is a spectrum of motivation where zero is ‘What diabetes?’ and ten is ‘I log everything…EVERYTHING…ask me how many carbs I ate yesterday and what my BGL was at 3.10pm and 5.55pm. Go on…do it. Because I can tell you. Do it. Ask me. And also, yes! I can tell you why my glucose levels spiked at 10.12am three months ago on a random Tuesday. Also, look at this: it shows how my glucose levels are impacted by the phases of the moon. In other news…here’s my last fifteen years of A1cs displayed pictorially, but I can also demonstrate them using interpretative dance if you would like me to. Would you? You would, right? Let me just find my Kate Bush playlist on my iPhone…’
Generally, I’m a solid 3.5. I don’t do graphs, I have a vague idea of what my CGM is telling me now-ish, and I can tell you my A1c to within about 0.5 per cent. I call this winning.
I have had periods – extended periods – where I am far closer to zero, which have not been great because that has added ‘not-doing-diabetes-guilt’ to the simple ‘not-doing-diabetes’ which basically equalled feeling crappy all around. And I’ve also been closer to ten – this, for me, was called ‘pregnancy’ – and I was borderline obsessive.
Someone recently asked me if I thought there was a secret to staying motivated. I don’t think there is, because surely, at least one oversharing blogger would have written about it by now.
But I do believe there are small factors that, when combined, do make it easier to remain, if not enthused, at least stirred to keep chugging along with diabetes.
Firstly, in range numbers beget in range numbers, and in range numbers make us want to check for more in range numbers more frequently. It’s undeniable that when we see numbers that don’t cause the response of rage, frustration, sadness, stress or anxiety, we are more inclined to check again. And again.
Technology that helps rather than hinders makes everyone feel better. Many think that it’s a given that new tech makes life easier, but unfortunately, that’s not always the truth, because often – at least to begin with – it requires more input from the user. Actually needing to do more, but not necessarily seeing results is not a recipe for remaining enthused!
Boring tasks are boring, so any way that we can eliminate them or reduce them helps. Making appointments to see our HCPs, finding time to visit a pathology centre for quarterly A1cs (and more) and keeping our diabetes supplies and meds current all take physical time as well as mental time. I have a pharmacist who is like my personal assistant when it comes to reminding me that it’s probably time to reorder insulin and NDSS products and prompts me when I need a new insulin prescription and I cannot tell you how much I love her. She sends me texts messages (totally unobtrusive) and I reply by text and then a day or two later pop in and she has everything ready for me. I can’t remember the last time I ran out of something, thanks to Mae!
But for me, if there was a silver bullet, it would be this: I am motivated because of today. Today, I have been able to do everything I have wanted to do and diabetes has not stopped me, even momentarily. And that makes me want to do it more.
I know that a large part of that is that I have the capacity, the will and the ability to do what I need to make this happen. I speak from a position of privilege, because I also know that the devices I am using – and am able to afford to use – certainly do help me with everything. They have helped to make my diabetes today doable, manageable, and as untroublesome as diabetes can be.
You can threaten me with what is going to happen in five, ten, twenty years’ time; you can tell me about all the disabling and debilitating complications that will happen if I don’t remain motivated and how they will impact on my life as a fifty, sixty and seventy year old.
But unless what you are saying is going to impact on me right here, right now, I can ignore it, and I can ignore the things that may help me reduce the risk of those things happening.
Perhaps that’s where public health messages about diabetes get it wrong. They tend to focus on longer term impacts. It’s not just teenagers who believe they are invincible. Despite a body that each and every day looks less like that of a sprightly youth, I think I am still young. I think all the things that are considered long-term issues are still years off. Being unmotivated doesn’t seem to matter when I don’t need to deal with those issues today.
But when diabetes does impact on my day now, then I notice. More hypos, more hypers, more interrupted sleep, more roller coaster numbers, more exhaustion, more feeling crappy. All of these things make day to day life more difficult. And I want to avoid them as much as I can.
I’m quite pleased with my solid 3.5. Sure, it could be better. Sure I could do more. But it’s consistent. And it’s achievable. Plus, quite frankly, everyone around me should be pleased with the absence of interpretive dance.

Click to get your own Casualty Girl bag.
After a wonderful couple of weeks of real holidays – sun in Italy, less sun in London – I headed to Berlin, saying good bye to my family as we headed in different directions. I was bound for meetings before EASD officially kicked off. And they were headed to Wales and canal boats with extended family. We could not have found ourselves in more different settings!
My first day in Berlin was dedicated to HypoRESOLVE, the Innovative Medicines Initiative (IMI) funded project looking to provide a better understanding of hypoglycaemia. I am on the Patient Advisory Committee (PAC) for this project, which kicked off back in May this year in Copenhagen.
The project is divided into eight work packages (WP) and it was WP 8 that convened the first meeting. I was there as part of the PAC, and also to provide the personal perspective on hypoglycaemia.
Back in May at the kick off meeting, I had given a talk called ‘The literal lows of my diabetes’, where I spoke about my own experiences of 20 years of diabetes and how hypoglycaemia had impacted on my everyday life. This was a very personal talk, where I spoke about the fear and anxieties of lows, my different hypo personalities and the terror that comes with impaired hypo awareness.
But for this new talk, I wanted to do something different. I didn’t want to highlight my own experiences, because I am but one person and it is important that the audience never feel that they have ‘done diabetes’ and understand the ‘patient view’ because they have listened to one person.
I wanted my focus to be on the disconnect between how hypoglycaemia is regarded in the clinical and research world as compared with the real-living-with-diabetes world.
So, I used the tools at hand, and the fact that there is a vocal and ready to help diabetes online community just a few clicks away and sent out this tweet:

It was apparent straight away, as the responses came flooding in, that the way hypos are described and classified in clinical and research terms is very, very different to the way those of actually experiencing lows see them.
Here is how hypos are categorised in the literature:
 Straight forward, neat, tidy, pigeon-holed.
Straight forward, neat, tidy, pigeon-holed.
And yet, when I asked PWD how they would describe hypos, here is what they came up with:
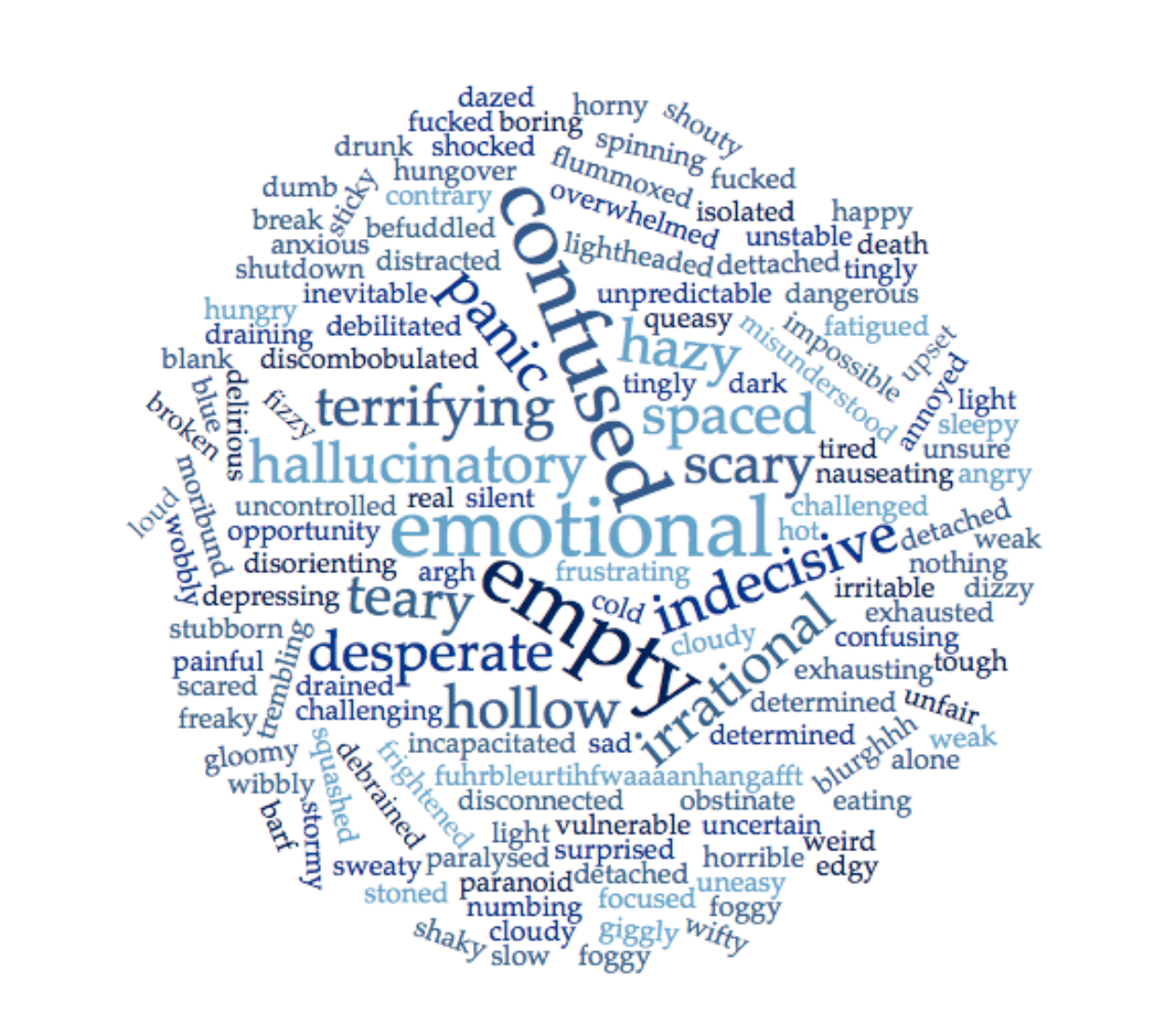
Some of the words were repeated multiple times, others appeared only once. Some of the words are the words I use to describe my own hypos, many I had not considered. Yet every single word made sense to me.
Hypoglycaemia, in the same way as diabetes, is not neat and tidy and it cannot be pigeon holed. I hope that my talk was able to illustrate that point.
And I hope I was able to highlight that using simple words and simple categorisations only service to limit and minimise just how significant and impactful hypoglycaemia truly is for those of us affected by diabetes.
You can keep an eye on the progress of HypoRESOLVE on Twitter, and via the website.
DISCLOSURE
The HypoRESOLVE project funded my travel from London to Berlin and provided me with one night’s accommodation. I am not receiving any payment for my involvement in the Patient Advisory Committee.
Previous disclosures about my attendance at EASD 2018, can be found on this post.
Yesterday, I caught up with a friend I’ve known for a number of years. Monique and I are diabetes twins, diagnosed within days of each other twenty years ago. (She suggested that we start to plan for a joint 21st next year – an idea that I immediately jumped on and have already been searching for a DJ, light show… and potentially a booze cruise. Aren’t you glad you suggested that, Mon?)
We don’t catch up enough, but when we do, I am always in awe of her. She is one of the most dynamic women I know. Years ago, she founded and ran HypoActive – a peer group for people with type 1 diabetes. She was a member of Team Type 1 (a cycling team made up exclusively of people with type1) and competed in the winning Race Across America team.
She has held a number of board positions, and has worked tirelessly to promote women in sport.
On top of all this she is raising two daughters to be the leaders of the future (her kid dressed as Emmeline Pankhurst for book week this year!).
While our interests (obviously) may not mirror each other, I am constantly astounded by her commitment to the causes she supports, because she does so with the sort of no-nonsense, tell-it-like-it-is attitude that made her a world-class cyclist.
One of the (many) things we spoke about yesterday was parenting kids and encouraging their independence. Unsurprisingly, Monique’s girls are keen bike riders and this is their preferred mode of transport around their neighbourhood. When Mon’s older daughter started to ride to school on her own, some other local parents weren’t quite so comfortable with the display of independence and made their dissatisfaction known. (You can read Monique’s account of this experience here.)
I spoke about how my kid gets to school (less inclined to get on a bike, more inclined to get on a tram and try to not get stepped on as she has her nose in a book and ignores everyone). I mentioned how I thought that when she started at her new school I’d be driving her most days, but she decided after day one that she wanted to get on the tram with her friends, letting me know loud and clear that her independence was not to be stifled by a mum wanting company on the morning commute.
Teaching our kids independence is a double edged sword for us parents. Of course we know intrinsically that it is important; but we also want to somehow coddle them and protect them from all the real and imaginary threats that are often far larger in our own minds than in reality.
But actually, the two aren’t necessarily at odds with each other. In fact, when we teach our kids independence and allow them freedom, we are actually making great efforts to keep them safe.
It’s not always easy to join those dots, but surely if we are confident with the way that we are parenting, and trust the rules, guidelines and instructions we put in place, we should be able to see how we’ve done everything we can to keep our kids out of harm’s way.
Sure – critics of this thinking may say that it’s not our kids we should be worried about, it’s others who may do them harm. But these worries should be part of the conversations we have in our endeavours to develop their independence.
If we trust ourselves and the job we’ve done, we should feel confident to step back and trust our kids to safely take on more and more responsibility, even if letting go and relinquishing some control can be difficult.
Monique and I then spoke about these same principles in terms of diabetes (and I’m sure healthcare in general) and how some HCPs struggle with losing control of how people with diabetes manage their own diabetes.
In the same way that we need to trust and have confidence our parenting, HCPs need to trust their education efforts, feeling confident that they have set out the principles of effective diabetes management, and providing PWD with the tools to adapt those principles to suit us and our diabetes in the way that works best.
The way we seek our independence in diabetes is to take what we are taught, and adapt it to work the right way for us – even if, sometimes, that is in direct contrast to the way our HCPs have instructed.
Perhaps that’s the real foundation of the whole idea of being ‘deliberately non-compliant’ in diabetes. Sure, we are going against what we have been told and are doing diabetes in ways that our HCPs might never recommend or even understand, but if the results we see are actually as good or even better than what is expected, then those initial teachings set us on the track for success!
My deliberate non-compliance – the very thing that the HCPs at ADATs last year prickled about – has resulted in my diabetes being the most ‘compliant’ it ever has…and, (even more importantly), me feeling better about diabetes than I ever have.
I am fully aware that a big part of my ability to go off label is because I was shown and taught the principles of diabetes by some great HCPs. To me, this is the perfect marriage of theory and practise. The theory I have been taught has allowed me to break the rules and create ways to practically manage my diabetes that work for me. Independently.

Dinner at our place, (a few years ago now). Kerri, me, Bastian, Kyle and Monique.
The hydrangeas on our front veranda are starting to shoot. Only three weeks ago, they were bare, and considering my almost perfect record of killing plants, I wondered if I’d pruned them into oblivion a few months ago. ‘Are these dead or just dormant?’ I asked, every time I walked out the front door, or stood there with the key in my hand waiting to go inside. I was almost ready to bring in the big guns (mum and mum-in-law) for advice and rescue.
Turns out they were just doing their cold-weather thing and waiting for some warmth, and now, every single day, there is more bright green foliage unfurling. In just a couple of months they’ll be weighed down by white pom pom flowers.
Over the back fence, the branches on the neighbours’ tree – the tree that heralds the seasons with such grandeur – are covered in cottony white blossom.
Because it’s spring. Finally. It’s really spring.
And I’m ready for it, and for the clutter and sludge that inevitably infiltrates my mind in the cooler months to have a good spring clean!
Diabetes takes up a lot of my headspace. Although, as I explained to friend across the seas the other day, it’s not my diabetes that is doing that. My diabetes is boring. I love my boring diabetes.
But ‘the world of diabetes’ is overwhelming me at the moment. It’s not the first time I’ve felt this way. It happens sporadically. Sometimes it’s because there is just so much going on, other times it’s because I just feel over it all. And then there are the times that my own diabetes combined with ‘work diabetes combined with ‘miscellaneous diabetes’ just gets too much.
And that’s where I’m at. I think that months holed up inside in front of the fire allow too much time to be overtaken by the minutiae of the diabetes world, and I start to take everything on board too much. So it builds up. And up and up, until I am where I am now.
I think perhaps this is my own version of SADS, but instead of seasonal affective depression I have ‘seasonally affected diabetes’. It happens each year – I can chart it alongside a weather, sunlight and heat chart.
So, I know there is light at the end of the tunnel. Melbourne is getting warmer. There are blue skies – the sorts of skies that greet me when I wake up in the morning, hang around all day and melt into beautiful sunsets in the evenings. And there is sunshine.
And with it comes some clarity to sort through the sludge, sweeping out some of the things taking up too much mental space, discarding what I should have let go of months ago.
I’m kickstarting ridding the discontent of winter by heading to warmer climes next week, initially for a holiday and then a conference. I’m hoping that in the two weeks before the conference starts will be spent outside, wandering cobblestone streets, enjoying lighter fare (and gelati) and basking in sunshine- real sunshine that will dance on my skin and penetrate all the way through to my bones.
By the time I get back home, Melbourne will be in full spring glory – the jacarandas will have started to flower, the blossoms on the tree over the fence will have scattered to the ground and given way to a covering of green leaves, dappling sunlight across the garden.
And hopefully, I’ll be lighter and clearer and spring-cleaned, with nothing more than my own (boring) diabetes.

My favourite local serving up my first iced latte of the season!
It’s Women’s Health Week here in Australia and once again, Jean Hailes for Women’s Health has been doing a stellar job of talking about women’s health issues that are rarely (if ever) spoken about in the public sphere. As usual, this year’s campaign is presented in a clear, no-nonsense way. Just as it should be.
Shining a light on women’s health issues is critical for a number of reasons. There is still too much stigma associated with women’s sexual and reproductive health, so finding a way to easily speak about the realities of women’s health just makes sense.
Not all women’s health issues necessarily seem relevant to diabetes. But, as ever, diabetes has a way of complicating things, so it makes sense that they are on the list of things covered when speaking with our HCPs.
I honestly can’t remember the last time my GP spoke with me about any sexual or reproductive health issues. Some women see gynaecologists regularly (I see mine every couple of years for a pap smear), but that may not be the case for most women. Surely conversations about contraception, periods and other things should be part of a regular check-up alongside other ‘tick the box’ issues such as blood pressure, cholesterol and weight.
I wish that I had seen an endo from the beginning who had spoken to me about women’s health stuff. I know that it wasn’t until I found the endo I see now – one who I sought out specifically for her expertise in women’s health and pregnancy – that issues such as contraception were even mentioned.
So, here is a (non-exhaustive) list of things that women with diabetes may want to consider chatting to their HCP about – and that HCPs may want to consider speaking with PWD about. (There are links at the end of the post for where to go for further information.)
Periods. To be honest until I was trying to get pregnant, I really didn’t think much about my period. I thought of my lack of regular periods (as in, I would get my period sporadically maybe four or five times a year) as a blessing, rather than something to be concerned about. Of course, once I was trying to get pregnant, I was desperate for a monthly period that I could set a clock to.
No HCP had ever spoken to me about how diabetes would impact on my period – or, probably more importantly, vice versa. I had no idea about how different times in my cycle might affect my glucose levels. In fact, I think it wasn’t until I started wearing CGM and could really see what was going on that I learnt how to manage my insulin doses at different times throughout the month. (And it also explained the two days each cycle I was so freaking low I pretty much took no insulin. Apparently that’s how MY body deals with ovulation..)
If I was diagnosed today, I would be asking a lot of questions about diabetes and menstrual cycles and the best way to adjust my management methods depending where I am in my cycle.
Sex. When I’ve written about diabetes, women and sex before, I’ve noted how at diagnosis no one spoke with me about how diabetes could impact on my sex life. It wasn’t until I started speaking to other women about it that I realised that this is an issue for a number of us.
We need to start talking about women with diabetes and sex in a non-threatening way that normalises the discussion. (Keep an eye out on the work that started with the Kath Barnard’s survey on this important issue.)
Contraception. No one mentioned contraception to me when I was diagnosed. I was twenty four, engaged to be married. Surely both the endo and CDE I saw the day I was diagnosed realised that I was having sex, or considering it after I was married. (I really, really hope that they didn’t think that they didn’t need to speak about it with me because we weren’t married yet…because it was only 20 years ago and there’s no place for puritan attitudes in healthcare. Plus, that ship had sailed. A long time before.)
At the time, I was on the pill, but there was no discussion about the best form of contraception for me relating to diabetes, (was there a better pill to be on?), and I didn’t know to ask. Surely, all women of child-bearing age should be asked regularly about contraception, especially as women with diabetes are so often told about the importance of avoiding unplanned pregnancies.
Pregnancy. Thankfully, these days finding information about diabetes and pregnancy is relatively simple. If you know where to look.
But twenty years ago, when I was diagnosed, the only thing I was told about diabetes and pregnancy (and I think it was only because I asked) was ‘You need to have all your kids by the time you’re thirty’. (Not sure if just scraping in three days before I turned 31 counts there. Probably not. Looks like this deliberately non-compliant palaver has been happening for a while….)
Talking pregnancy and diabetes needs to be done delicately, but it needs to happen. And, ideally, it needs to happen long before pregnancy is even being considered.
Back in 2003 when I was at Diabetes Vic, I coordinated the first diabetes and pregnancy info evening. Over 100 people were squashed into an overheated room in the basement of the old Royal Women’s Hospital. At the end of the night, I was walking around speaking with as many of the people who had come along as possible to see if they had found the evening useful. I walked up to one woman and thanked her for coming. ‘I hope that you found tonight helpful,’ I said to her. She nodded at me, and I noticed she was holding onto a copy of the ‘Can I Have a Healthy Baby?’ booklet that Diabetes Victoria had published with Realty Check and ADIPS the previous year. ‘My daughter has T1D,’ she said to me. ‘She’s only 8, so obviously this isn’t something that is relevant now. But I wanted to know so that when she asks questions I can answer them. I feel really reassured that she can have a baby if she wants one if it’s planned.’ I remember reaching out to her and hugging her (I have no boundaries). ‘Your daughter is so lucky to have you in her corner,’ I said to her. ‘Thank you for coming!’
Fertility. This isn’t the same as pregnancy. It’s not an easy subject – ever – but it is one that needs to be discussed openly and safely. I can honestly say that no healthcare professional has ever discussed fertility with me unless I have raised the issue.
My experiences around fertility have been complex, emotional and quite painful. It took me a while to get pregnant the first time. My irregular periods needed to be addressed (fortunately, that was easy enough with only Chlomid needed), but even once I was having monthly cycles, and apparently ovulating regularly, I could not get pregnant.
When finally did, I miscarried. Miscarriages are common. I know that. But it still sent my spiralling into a really difficult period which took a lot of time and effort to emerge from. I got pregnant and had a baby, and thought that from there, fertility issues would be a thing of the past.
But I think that because miscarriages are so common that sometimes it can be forgotten just how traumatic they can be. My first miscarriage ended my first pregnancy, and the two other miscarriages I had ended those ones. It’s clear that while I seem to be able to get pregnant, keeping those babies growing, safe and alive is not something my body does well. I wanted that explained to me – or at least for someone to speak with me about it.
Diabetes and fertility was never, ever discussed with me, except that I was reassured after each of my miscarriages that I could not blame diabetes for losing the baby. That was a double edged sword because I wanted to know what it was that was stopping me from being able to continue my pregnancies. I would have liked to be able to point at something. Because the alternative is that it’s just another thing my body can’t do properly.
PCOS. I was diagnosed with polycystic ovarian syndrome when I was about 26. I’d been referred to an OB/GYN by my endo because she wanted me to have a gynaecological check-up because we’d started seriously talking babies. My lack of regular periods was flagged as something that needed investigating and an internal ultrasound showed a number of small of cysts all over my ovaries. I had no other symptoms of PCOS, but that was enough for my OB/GYN to speak with me about potential fertility issues once we were ready to start trying for a baby. I had a laparoscopy and they were removed.
Both type 1 and type 2 diabetes can increase the risk of PCOS (more so type 2 diabetes) so this is definitely something to discuss with your healthcare team if you are in any way concerned.
Body image. I don’t even know where to begin with this because body image is such a huge, huge concern for so many women, and I really do believe that diabetes amplifies those concerns. Whether it is the physical signs of diabetes (tech that we wear on our bodies), the psychological side of being diagnosed with a life-long health condition or the emotional toil of having an allegedly invisible condition that we can’t help but see every day, living with diabetes significantly affects how we feel about our bodies.
This is one of the reasons that having a psychologist as part of our HCP team is important, because we need people who are able to ask the right questions and offer support and solutions for dealing with how we see our bodies.
Eating disorders. Diabetes and food; food and diabetes. It’s impossible to separate the two, and for some people, the relationship is complex and very, very difficult. Women with diabetes do have an increased risk of developing an eating disorder, and of course, there are diabetes-specific eating disorders. And, unfortunately, this is another issue that is not spoken about openly.
Menopause. At my last appointment with my endocrinologist, I raised something that I’d not raised yet. ‘What can you tell me about diabetes and menopause?’I asked her.
I’m not going through menopause – I’m not even peri-menopausal yet. But I don’t need a magic mirror into the future to see what lies ahead. And I like to be prepared.
So, there’s something you should know about how I came to see the endo I have been seeing for the last almost-17 years. I was searching for someone who could help with what I really needed, one of them being an expertise in T1D and pregnancy. She was absolutely the right endo for me then. And continues to be now, because recently, she has become an expert in menopause. (I know! It’s like she is a few years ahead of me in her areas of interest and expertise!)
If I’m honest, I’m a little stressed and worried about what menopause has in store for me when it comes to my diabetes, mostly because I know nothing about it. We’ll see how that plays out…
Self-care. Why do women find it so hard to prioritise our own care and take care of our own wellbeing? We do need to get better at fastening our own oxygen masks before making sure that everyone else on the plane has theirs in place.
This might be another reason to consider seeing a psychologist to ask for some tips for how to make sure that we remember to look after ourselves in a way that is healthy, consistent and achievable.
Pelvic floor. Diabetes, as the gift that keeps on giving, can mean our pelvic floor isn’t as strong as it could be. Just as nerves in other parts of our bodies can be affected by our diabetes, so can the ones in our pelvic floor.
(You’re doing your pelvic floor exercises right now, right? Yep. Me too.)

Looking for more info? Have some links…
Here’s the Jean Hailes for Women website for Women’s Health Week.
The rather awesome Mindy from There’s More to the Story has been writing about diabetes and sex over the last couple of months and her posts are a must read. I wish I’d had something like this to read when I was first diagnosed.
Some information about diabetes and PCOS. This article is about type 1 diabetes and PCOS. And this one is about PCOS and types 1 and 2 diabetes.
The NDSS Diabetes and Pregnancy website is an absolute goldmine of information about pregnancy and planning for pregnancy. There are different sections for women with type 1 and type 2 diabetes, HCPs and loved ones of women with diabetes.
The NDSS Type 1 Diabetes and Eating Disorders booklet can be found here.
Lots of valuable information for PWD and HCPs at the Diabetes and Eating Disorders Awareness website.
I am old enough and smart enough to understand the way women are meant to respond to the lies of advertising. We are constantly told – and meant to believe – we are not enough. Our bodies are not slim enough, our skin is not taut enough, our thighs are not firm enough, our hair is not shiny enough, our arms are not toned enough.
At my current age, I’m meant to be trying to erase the signs of ageing, willing wrinkles away with an assortment of lotions, potions and minor (and major!) cosmetic surgery, plus trying somehow to regain the body I had twenty years ago.
Thanks to a mother who pointed out the deception of advertising from when I was a young girl, refusing to allow us to buy into the spin, plus a healthy dose of political and feminist teachers at school, all combined with much reading as a teen of Naomi Wolf, Susie Orbach, Gloria Steinem and Betty Friedan, and then later on, Kaz Cooke’s Real Gorgeous, I manage to not be too overcome with my body image issues and feelings of inadequacy. Mostly
My body is forty-four years old. I’m okay with looking in the mirror and seeing a reflection that reminds of me that.
I see the lines around my eyes and am not too startled because I know they have formed thanks to many years of laughing so hard that I can barely breathe, cried so hard because of loss that has rocked me to my core, walked for miles through cities while the sun has shone brightly (and I didn’t reapply my sunscreen).
I’m okay with my body not looking the way it did when I was twenty. I quite love the evidence that I carried and delivered a healthy baby – there is a lot of evidence of that! My far-less-than taut stomach points to that as much as the scar along my lower abdomen from where she escaped.
Surgery would be the only way to return to the pertness destroyed after twenty months of breastfeeding. But quite frankly, I’m kinda proud of the signs from that, because initially it was such a challenge for me to learn to breastfeed, and then manage the subsequent hypos. There should be some proof of the effort that all took!
I can deal with my skin not glowing as it did when I was younger, and the signs of a late night being far more visible than when I was in my early twenties. Those days I could manage being out until the early hours, and then be up bright and early for work the next day with nothing more than a coffee and a slick of my signature red lipstick to deal with the lack of sleep.
And the occasional grey hairs that appear around my hairline are met with acceptance – and gratitude that I can vainly still pluck them out because they are so intermittent that it’s easy to do.
I once wrote that ageing is a privilege. Not only do I believe that, but each and every additional year I live with diabetes, I believe it even more.
I just wish that while I acknowledge the miracle that is my life today – because had I been diagnosed with diabetes a mere seventy-seven years earlier, I would not be alive today – I could be more comfortable and accepting with how I wear diabetes on my body and in my mind.
It makes no sense that I am still uncomfortable of the visible signs of diabetes on my body. But that is how I react most days. The devices I wear still make me wince at their sight. I try to avoid looking at the scars and marks and signs of those devices on my body – all over my stomach and hips. I notice myself more aggressively washing those parts of my skin, and wonder if I am trying to scrub away the signs of diabetes.
In the mornings when I get dressed, I hide my pump and RileyLink away as fast as I can, tucking them into my bra and throwing on something over the top so they are not in my line of vision as I stand at the mirror applying my makeup. I’m not ever going to be one of those people who wears her pump on her hip, proudly showing it to anyone who asks.
And even though my Dexcom is on my upper arm, I prefer the cooler months when I can hide it away from sight under layers of Melbourne black.
Today, I spoke with a mother of a teenager who wanted to know how she could convince her daughter to agree to wearing her pump again. ‘She hates how it looks on her,’the mum said to me. ‘When will she get over it and just realise it’s the best way for her to manage her diabetes?’And I didn’t know what to say because I am a woman in my mid-forties and I am not ‘over it’, seventeen and a half years after first attaching an insulin pump to my body.
The only thing I could say was that it can be a difficult thing for some people to accept – and that I too struggle with it. But that the compromise for me is that as much as I hate seeing diabetes on my body, I’ve accepted that the devices make me feel and manage my diabetes better with them there. But understanding that takes time. Maybe age helps too.
My ageing body is something I can wear with pride because it tells the story of my life and what my body has managed to do. Whereas my diabetes body points to parts of me that are broken. And can’t be put back together, no matter how hard I try, or how hard I try to convince myself otherwise.
Have you seen Body Posi Betes? It’s the brainchild of my darling friend Georgie Peters who is doing everything she can to promote body positivity in the diabetes space. You can join the Body Posi Betes Facebook page here and follow the Insta feed here. I’m going to binge through all the posts again right now, because truthfully, I need a bit of diabetes body positivity right now.

Usually hidden from (my) sight.

Click to be taken to Daisy Natives store.
I bought a new t-shirt the other day. I saw it on Instagram and decided that I just had to have it. I’m not sure if it was growing up in a mostly female household; or the six years I spent in an all-girls school; or perhaps it’s the friends I am fortunate enough to be around a lot; or maybe the fact that most of the people I work with are dynamic women; or raising a daughter in 2018. Whatever it is, girls supporting girls, and women supporting women is the approach I have always tried to take in both my personal and work lives.
I guess my thinking is that we need to look out for and support each other because we know that outcomes for girls and women around the world are not always that great. And also, when women build each other up, and support and encourage each other, we are unstoppable!
I was thinking about this last night as I followed a Twitter conversation that all started after a somewhat sensationalist article in a newspaper about a bloke (sportsperson?) who, as it turns out, seems to have some diabetes-related neuropathy. As people shared the article and spoke about it, there were a couple of comments from people with diabetes about this person – another person with diabetes – ‘not looking after himself properly’.
When I started reading, I almost pinched myself to make sure that I hadn’t been sucked into some sort of void, and been dragged back to another time. Because this conversation has happened before – countless times. (A search through Twitter and this post pointed me to just a couple of those times.)
Diabetes-related complications and stigma. Diabetes-related complications and language. They go hand in hand. And along for the ride is judgement.
The complexity between diabetes, and developing diabetes-related complications is far too much for my little brain to comprehend. But I do know that there are no guarantees in diabetes. And I know that blaming people for whatever path their diabetes travels is not helpful in any way.
When someone suggests that another person with diabetes is ‘not looking after themselves properly’ there is a lot packed into that. It may not be intended, but that comment is so loaded with blame and shame and judgement that it becomes agonisingly heavy and, quite frankly, terrible.
To suggest that someone’s diabetes-related complications are the result of them ‘not looking after themselves properly’ means that essentially what is being said is that the person intended for this to happen. That they ‘brought it on themselves’. That they deserve to now have to face a future of diabetes-related complications.
To that, I say bullshit!
And, somehow, it is even worse when a comment like that comes from another person with diabetes, because if anyone should understand how harmful judgement can be, surely it is others with diabetes.

Supporting each other doesn’t mean just patting each other on the back and saying ‘good job.’ It is far more than that. It is acknowledging that we are doing the best we can at that moment time with what we have. It’s accepting that there are myriad ways of managing diabetes, and that people should have the right and the ability to choose the way that is right for them – even if we don’t think it is right for us. It is encouraging others’ efforts, cheering their successes and standing alongside them when things are tough. It is being happy for other PWD when they are doing, or being invited to do, great things.
It is not saying ‘You are not doing enough’.
We would be quick to say that it’s not okay for a healthcare professional to suggest that we are not trying hard enough. We don’t accept it when the media make claims that people aren’t looking after ourselves properly. We push back and say it is not okay when those without diabetes suggest that we are not doing our very best.
And in exactly the same way, it is not okay for other PWD to criticise one of our own because, honestly, we should know better. We should be on the same side. We should be building each other up.
It is completely unreasonable to expect that people with diabetes are going to agree on everything, and actually, who would want that anyway? Diversity of opinions is as important as diversity of experience. We all have our own ideas and ways to live with diabetes and there will be times that we completely disagree. That is all fine, as long as it is done with respect.
But even with those differences – differences that we can celebrate – the commonality of messed up beta cells should be what brings us together to be on the same side.
I could be Pollyanna-ish about it all and say that we should just be kind to each other, and that may be a good place to start.
Living with diabetes is fucking hard. We never, ever get a break from it. No matter how manageable our diabetes seems or how cruisy things may be at a particular moment, it is still always there. It doesn’t matter if we are scaling mountains or running marathons. Or living our dreams or travelling the world. Or getting up in the morning and going to work or school. Diabetes does not take a break.
Diabetes doesn’t take a break. But we can give each other one. No blame. No shame. Just an acknowledgement that we are doing the best we can. PWD support PWD. That’s what makes us stronger. That what makes US unstoppable!

P.S. If you really don’t agree with what someone is doing with their diabetes, you can say nothing at all. You don’t have to be critical.
Last week, I spent a busy week at Australasian Diabetes Congress. I spent a lot of time with work colleagues, health professionals, the event organisers and researchers.
And I was fortunate because most of the time, I was around at least one of my peers. Between the #DAPeoplesVoice team, (Mel, Frank and David), other diabetes friends from home, (Ash, Kim, Gordon and Cheryl), and away (Grumps), there was always someone nearby who I could rely on to ‘get’ diabetes. (This is important always, but conferences have their own special challenges where diabetes mates are certainly appreciated to help keep some perspective!)
I have written countless times before about the power of peer support. I have also written that my peers have been the ones to have truly helped me through some of the most difficult diabetes situations I’ve faced – not necessarily with advice, but simply a knowing look, a nod of the head, or the words ‘me too’. Our peers help us make sense of what we are dealing with, provide us with endless support and help make us feel connected to others. And that’s important with a condition such as diabetes, because it is all too easy to feel that we are on our own.
Which is why I was so pleased to learn about ConnecT1ons, a new initiative from Diabetes Vic, which is looking to provide that support to another group within the diabetes world – parents of kids with diabetes.

It is undeniable that parents of children living with diabetes have their own brand of challenges. This was brought home to me again last week during the Diabetes and Schools Forum when parent of three children with type 1 diabetes, Shannon Macpherson, spoke about some of the difficulties she and her family have faced with her children in the school setting.
And again this morning, when I was speaking with a parent who is having a very tough time with her young, kindergarten-aged child. ‘Renza,’ she said to me, as she explained what was going on. ‘You have no idea. Having a child with diabetes is impossible because we cannot be with them when they probably need us the most.’ She’s right – I have no idea.
But other parents of children with diabetes would and do understand. And as they shared their empathy, they would also probably share some of the things they’ve done to help them through similar tricky situations.
Diabetes Victoria is looking to bring parents like this together for an event where they can meet other parents of children with diabetes. Plus, it’s a few days of respite from looking after their child with diabetes, while knowing their kid is safe (and having an absolute ball) at diabetes camp. What a brilliant idea all ‘round!
You can watch a video explaining the project here, and hear from Jade, the mum of a young boy with diabetes share some of her experiences – and how parents just like her will benefit from ConnecT1ions.
As is always the case, finding funds for initiatives like this is a struggle, so today, Diabetes Victoria launched a crown funding campaign and is seeking to raise $15,000 to run ConnecT1ons. If more is raised, they can run additional events. The crowd funding is only open for a week, so please do consider making a donation – and doing it now! Click here to be taken to the Pozible page.
Congratulations to Diabetes Victoria for acknowledging that parents of kids with diabetes are a specific group that need support amongst their own peers. Extra huge congrats to Kim Henshaw who has spearheaded this project as part of her role as Children and Families Coordinator.
Please do donate. I returned home last week after spending time with my peers feeling refreshed, energised and connected. Parents of kids with diabetes deserve to feel the same by spending time with each other.

Not a functioning beta cell amongst us.
Disclosure
None! I was sent information about ConnecT1ons from the Communications Manager at Diabetes Victoria last week, but she did not ask me to write about it. I don’t work for Diabetes Victoria (I left there back in Jan 2016) and have had nothing to do with this new initiative. But you have to admit it’s a good one. Hence, this post.
It takes effort to look at diabetes in a positive light. And sometimes, we need other people to shine that light for us. My husband changed a negative thought I had about an aspect of diabetes with one comment. And to this day, something that once filled me with sadness and dread, now makes me feel grateful and fortunate.
__________________________________________
Living well with diabetes. That’s how I like people to think of me. And how I like to think of myself.
But there are occasions – rarely, although sometimes more frequent – where I do feel living with a life-long health condition that is there every minute of every day start to creep over me and a sense of dread and worry plant themselves at the back of my mind. For me, this is part of diabetes burnout. It’s a feeling of being overwhelmed by what diabetes is right now but even more, what diabetes could be in the future. How will my faulty pancreas and my autoimmune problems play out in my life?
And is there any point worrying? At the moment, things seem to be tracking along well. Annual complications screenings tell me that I am doing okay and I’ve read some research that shows people with diabetes are living longer and longer.
So why the dread and anxiety and is there any point? And even more, is it possible to change the way that we think about diabetes?
When I was first diagnosed, the smell of insulin would fill me with dismay. The very scent would remind me of the horrid, scary photos the doctor showed me within the hours of being told I have type 1 diabetes. An invisible force would reshape me from the vibrant 24-year-old I was at the time to a withdrawn, sick, shell of the person I really was. For months I felt this way and every time I gave myself a shot, it was like I was slowly drowning.
But that all changed one day. I drew up two units to squirt through the air before jabbing myself and said ‘Urgh. I hate the smell of insulin. It’s everywhere – I feel like it’s what I smell of now.’ Aaron who was sitting next to me looked up and said simply and matter-of-factly, ‘I don’t hate it. It’s the smell that keeps you alive.’
And just like that, the smell of insulin went from being a death sentence to life saving. It never bothered me again. Keeping the perspective of diabetes in its rightful place is not easy and there will always be times that we feel like it is heading in the wrong direction. We just need to find ways – and people – to say things to help us get back on track.






