
You are currently browsing the category archive for the ‘Health’ category.
This morning as I was buzzing around getting ready for work, I suddenly stopped. I realised something that had obviously been creeping up on me so incrementally that I had not noticed it before.
I looked around the bedroom and saw empty cannula packaging from the line change I had done when I got out of the shower and the empty sensor pack with the date written on it so I would remember when it was inserted. I went back through my CGM trace and pump history, noticing where I had bolused for a high BGL, set a temp rate for an impending low and calibrated at the appropriate times. I checked the history on my BGL meter and saw that I have been checking regularly and that the numbers were not as crazy as they have been.
I looked in my bag and saw a spare bottle of strips, my fully stocked ‘emergency’ kit, and a juice box and a small container full of glucose tabs ready in case I needed them.
When I got into work, my desk was prepared for all contingencies – more glucose tabs on the desk, a couple of spare cannulas in the top draw, as well as a few syringes. And a few single portion packs of Nutella.
I was – I am – managing my diabetes – well and without any stress at the moment. The burnout fog that had enveloped me for a long, long time seems to have lifted without me even noticing, and the diabetes tasks that form part of my day and had been so, so difficult to manage, have become routine. I do them without thinking. Checking my BGL and calibrating my CGM just happens. Bolusing for meals or my morning milky coffee is done before I take that first taste rather than half an hour later because my CGM is blaring at me that I am high.
Am I feeling motivated? I’m not sure that is the right word. I don’t have a desire to do these things. I am not so focused on diabetes that I think about it all the time.
But I am doing what I need to. Routinely. Just like brushing my teeth, combing my hair and putting on a necklace in the morning.
Perhaps that’s the thing about managing diabetes well. It’s the balance between getting the things done and not panicking about them. Or feeling so anxious and guilty because they are not getting done.
I don’t know the secret to this change. I do think that a big part of it is wearing my CGM all the time. Once I managed to hurdle feeling overwhelmed by the data and just accepted the numbers for what they are and acting accordingly, I feel much more driven to ‘do diabetes’. And perhaps as I see that things are not as dire as I often imagine them to be, I feel that I can just get on with things.
This is the roller coaster of diabetes. The ebbing and flowing of motivation and being in the headspace to get things done. I’m in a good place for now. I just have to work out how to stay here.

Emergency stash at the office (for lows or as required….)
It’s gloomy in Melbourne today. I have tights on for the first time in months and my hair is now frizzing thanks to the rain I was caught in as I ran next door for a coffee. (The silver lining in all of this is that there is fabulous coffee right next door to my new office. Also, extra silver lining is that I can see the weather out of my beautiful window. The not-so-silver-lining is that I am reminded that I am fool, because window = seeing rainy weather and yet I still forgot to take an umbrella…)
So here are some things that are keeping me either amused, happy, annoyed, interested, fascinated and heaps of other things too!
Roses spared and children saved
Today, the Spare A Rose Facebook page announced that 376 children would be benefitting from people’s generous donations this Valentine’s Day.
It’s not too late to make a donation, or even consider making a monthly donation throughout the year. AUD$6 each month equals a month of insulin for a kid who would otherwise not be able to afford it.
While this was the focus of our Valentine’s Day, there was still a lot of baking. Because I love a heart shaped cookie. Or giant brownie. And sprinkles.

Still the wrong name for this week
I think that the name misses the mark because it focuses on weight and not health. The overall aim of the week is to encourage people to cook more at home to achieve a healthy weight. Here’s just a little of the conversation with the DAA (after they read my post last year) on Twitter:

I think that this really does a disservice to the role of dietitians in healthcare. I am of a healthy weight, but have benefitted from the expertise of dietitians in the past.
The name of this week turns me off actually wanting to participate in any way, even though there are some terrific initiatives. What are your thoughts on this one?
In the genes
Why do some people develop diabetes-related complications and others don’t? We’re told that ‘control’ is the reason, but we also know that some people develop complications, despite years of what is considered ‘good control’ while others who struggle to reach targets don’t.
Things I wish I knew
I learn new things about diabetes each and every day. But how much easier it would have been while navigating this annoying bloody path to have known stuff earlier on. Diabetes UK has released a new book, 100 THINGS I WISH I’D KNOWN ABOUT LIVING WITH DIABETES, which includes information collected from over 1,000 people with diabetes with input from clinicians. The final 100 were selected by people with diabetes, (nice engagement there!), who chose the tips they thought most useful.
Oh – and while talking about Diabetes UK: Happy Birthday! They turn 82 years old this week.
New (to Australia) Tech
Looks like Australia is about to catch up to our friends in the EU who have had access to Freestyle Libre Flash Monitoring. The Flash website went live this week. More details – such as cost and release date – are yet to come, but you can register your interest. Have a look and register your interest.
And while we’re talking new tech in Australia, a couple of weeks ago, the Aussie launch details of the Dexcom G5 were announced. You can download the app (iOS only) which is already available from the App Store, although you won’t be able to use it until you are hooked up to a G5. The App has the ‘Share’ capability which means that you can (just as it says!) share your data with others.
Rock on
Last week, I was sitting at the front of our house, enjoying the sunshine and my day off, and listening to Live Fast, Diabetes, the new song from Adelaide punk/rock band, Grenadiers.
A very crotchety woman walked by, stopped as she heard the music, and scolded me with this nugget of wisdom: ‘You’re too old to be listening to that noise.’
Yeah, we know
Science: ‘Apparently BGLs are lower in warm weather.’
PWD: ‘Ah, yeah. We know. We’ve known for ages….’
Love it when evidence catches up!
And finally….
It’s Tuesday. Do the #OzDOC tweet chat! Tonight at 8.30pm AEDT.
For work, I signed up to a new healthcare app that would magically and algorithmically measure my health. Health apps frequently annoy the bejeezus out of me. You can tell the ones that have never met a real person and that the boffin who is developing the app lives a lonely life in a cave without regular contact with anything with heartbeat. (Shout out five million to my fave app, MySugr, because it is developed BY people with diabetes FOR people with diabetes so it, you know, works.)
Anyway, to sign up for this one, I had to fill in a few details about my health and wellbeing and then I got a final health score. It was pretty thorough. I added things like my most recent blood pressure, cholesterol reading, height, weight, food (which, despite ridiculously frequent mentions of cupcakes and doughnuts on this blog is mostly fresh, home-cooked and healthy), exercise (ha!) and health conditions. I ticked the ‘no’ box for every single one of those, except, of course, type 1 diabetes.
My overall score came back at 65%. I then was given a list of measures that I could take to increase my health, most of which I already do (other than exercising to which I am a conscientious objector).
I decided to test this little app and re-entered all my data with one little change. This time, I ticked the ‘no’ box for every single health condition.
The magic little algorithm spat out a new result. Suddenly, I was now 90% healthy. The suggestions to improve this number focused solely on doing more some exercise.
So, here’s the question. Am I significantly less healthy because I have type 1 diabetes?
My answer to that question is no. When I consider the level of attention I give to my health today as compared with before being diagnosed with diabetes, I would say that I am a lot more in tune and interested in my health now. I couldn’t tell you what my blood pressure or cholesterol was before I was diagnosed. Can now! I have regular check-ups and screening for things that probably would have slipped under the radar before.
And when I think about friends the same age as me – an age where we start to be reminded of the sorts of things about which we might want to speak with our doctor – I know that I definitely more on the ball than most of them.
Perhaps I have had to reshape what being healthy really means. Maybe pre-diagnosis I would have considered needing to medicate myself each and every day while monitoring my health closely would equal being unhealthy. But that’s not how I think. I think that I am healthy – and part of that is because I do those things. I am not ‘healthy even though I have diabetes.’ I am just … ‘healthy’.
Am I in denial? Have I rewritten what healthy means to accommodate my health condition?
Or is it true. I am healthy. And sure, I could be healthier, but that has to do with laziness and I don’t mean the laziness of my beta cells.

That time I exercised.
Last week, my body said ‘Stop’. Not in a friendly, ‘Hey, let’s sit down for a minute and maybe close our eyes and have a little nap’ way. No. This was a ‘You, you’re done. No more.’
There was no negotiating. No cajoling. My body just refused to body.
On Monday and Tuesday last week, I came into work and was back home by midday. (Staying home all day, both days would have been smarter.) My head felt like it was full of paraffin wax and I could barely concentrate. I had to stop on the landing halfway up the stairs up to my office to catch my breath. And when I finally made it to the top, I felt as though I had run a marathon. I dosed up on cold and flu meds to help with the low-grade fever and achy muscles. I felt pathetic. And frustrated and annoyed. And grumpy.
My BGLs were all over the place – high mostly, with the occasional crashing low after I rage-bolused because I was sick of the week being brought to me by the number 15.
On top of it all, I was trying to work with the kidlet to plan her birthday party which was last Saturday. In a moment of weakness (she knows how to pick it!) we agreed to a sleepover party and sent out invitations inviting the little munchkins to head over on Saturday afternoon and settle in for the night. And then, after sending out the invitations, did nothing until the day before the party. We started planning at 5.30 on Friday evening, exactly 24 hours before a drove of excited tweens would be descending on our house.
This is November exhaustion. It happens every year and every year I forget about it until I am in the middle of it. Most years, my body throws a tanty similar to the one it threw last week. Inevitably, there is a day or two where I just have to stop, take stock and recover. And more than that, I need to refocus on the health choices I am making and try to make better ones.
Because when I started to feel exhausted and poorly, I stopped making sensible diabetes decisions. Not enough BGL checks to really know what they hell was going on with the mild infection my body was trying to fight off; too lazy to reconnect a sensor after I ripped one out squeezing into my dress for the Research Australia Awards Dinner on Wednesday night; lousy food choices because I just wanted to grab whatever was easy and nearby, rather than planning and cooking foods that would nourish me while I was feeling below par; and not spending every spare minute asleep or resting, instead trying to catch up on all the things that had slipped while we were in the midst of World Diabetes Day festivities.
The thing is that what I perceive to be the easy way out ends up meaning that it takes longer for me to feel better. So, a week later, I am still feeling significantly worse than 100%.
This morning, I took stock. I am getting on a plane to Vancouver next Saturday for a very busy week of the World Diabetes Congress and realised that I really need to be better by then. I set alarms for regular BGL checks, I’ll put in a new sensor tonight when I get home and I’ve planned meals for the week. I hate that it takes a downward slide before I am jolted into doing what is best for me. But it just goes to show – yet again – that when the going gets tough, my health is the first thing to take a backseat. Until it can’t any longer.
Today, Australia has a new National Diabetes Strategy. I would be lying to you if I said that I had read every single word of the document (but, hey, knock yourself out and have a read here). I have had a skim. Now, every part of this Strategy is important – of course it is – but today I want to highlight type 1 diabetes in the document.
A lot of the Strategy crosses the boundaries of all types of diabetes, for example in the priority groups such as ATSI peoples, CALD communities, and those living in rural and remote areas. Attention to complications screening, recommending mental health screening at diagnosis as well as including regular monitoring in the Annual Cycle of Care, including diabetes-specific education and training to hospital staff. Services for women with pre-existing (types 1 and 2) diabetes planning and during pregnancy are considered with particular emphasis on pre-pregnancy planning and access to expert education.
While this is understandable – and there are many similarities in the way that these issues are addressed – there does need to be attention to the complexities type 1 diabetes brings. (Equally, the complexities of type 2 need to be tackled!)
But how is type 1 addressed?
Firstly, yay for a concise and accurate definition of type 1 diabetes. In fact, these 50 or so words could be used by any media outlet next time they need to define the condition! Also, well done to Sussan Ley (and her advisors) at this morning’s media briefing for giving such an articulate and well-informed summary of the diabetes situation in Australia.
 Very pleasingly, early diagnosis of diabetes is one of the key goals (Goal 2), and type 1 diabetes is given its own treatment, including potential areas for action and measures of this progress. The Strategy acknowledges that 20 % of people newly diagnosed with type 1 diabetes present to hospital in DKA. This needs to change. Better awareness and recognition of type 1 symptoms to improve early detection are flagged as potential action areas.
Very pleasingly, early diagnosis of diabetes is one of the key goals (Goal 2), and type 1 diabetes is given its own treatment, including potential areas for action and measures of this progress. The Strategy acknowledges that 20 % of people newly diagnosed with type 1 diabetes present to hospital in DKA. This needs to change. Better awareness and recognition of type 1 symptoms to improve early detection are flagged as potential action areas.
Type 1 diabetes in the school setting is mentioned, specifically looking at better supporting families, and children to participate fully and safely at school.
In the piece about transition from adolescent to adult healthcare settings, access to psychological services is emphasised.
Could there be more? Well, of course there could. Diabetes is such a huge issue; there can always be more. So, what would I like to see that hasn’t made the cut?
Well, I would have loved there to be something about diabetes technology, specifically around pathways for approval and access of emerging technologies, as well as sorting out issues with access to currently-available tech.
I would have loved for the early diagnosis topic to be broken down a little more. It’s an issue at all stages, but poses a particularly significant challenge for adults with type 1 who are often misdiagnosed based on their age. It can take a lot of time – and a long period of poor health – before they are correctly diagnosed and treated as necessary.
More attention to structured education programs (such as DAFNE and DESMOND) and their value. And how new programs, such as the valuable POSH program (addressing impaired hypo awareness), could be funded.
Breaking down the section on healthcare access for Australians in rural and remote areas and focus on particular problems faced by those with type 1 in those areas. Specialist diabetes care in these areas is minimal; type 1 specialist care is even harder to find
The same could be said when addressing the management and treatment of type 1 in hospital and aged care setting. Type 1-specific education is essential so we stop hearing people getting lousy treatment.
Of course, this is a high level document and the detail is simply not in there. No dollars have been allocated to the strategy. The devil is in the detail – and we just have to see how that plays out.
Finally, I’m not surprised to say that already the naysayers are out complaining about the Strategy. It’s the usual thing with the usual suspects complaining amongst each other and not offering any suggestions or looking at the positives. I wonder how many of the people complaining actively participated in the consultation stages of the development of the Strategy. I am just stating this here because really, it’s tiresome hearing the same complaints about the same issues. I have some concerns too but I am also willing to acknowledge this as a progress and a step in the right direction.
Happy World Diabetes Day to everyone for tomorrow. Shine a (blue) light on diabetes.

Tomorrow is Drop the Jargon day here in Australia. According to the campaign website, the aim of the day is … for professionals in Australian health, community services and local government to challenge themselves to use plain language.
People working in the health space are being urged to take a pledge to assist Australians who have low literacy make sense of health information and help them navigate our health system. Six out of ten people in Australia have low health literacy, so there is a real need to make sure our messages and information are presented in a way understandable to everyone.
The pledge asks people to:
- Use plain language in all communication
- Not use acronyms
- Explain medical and other technical terminology
- Check that information has been understood by your clients
- Work with a professional interpreter when necessary
- Politely point out when your colleagues use jargon
Diabetes is a condition rife with jargon. I’ve said before: it is like another language. I am as guilty as anyone when it comes to popping in acronyms, technical terminology and assuming everyone knows what I am talking about.
The website includes a link to a handy Plain Language Thesaurus to assist with finding simpler, clearly and less ‘jango-istic’ words when writing health information.
When considering writing in this manner, a lot of sensitivities and intricacies about different conditions are lost. For example, the thesaurus suggests replacing ‘diabetes’ with ‘elevated sugar in the blood’. (Amusingly, the same document suggests – just a page or two down – to replace ‘elevate’ with ‘raise, lift, make higher’.) Obviously, this doesn’t provide a particularly rounded definition or explanation of diabetes, and those of us who ‘get’ this space and understand the words we use when talking about it could criticise the ‘dumbing down’ of what diabetes is all about.
But think about it. If you were new to the diabetes game – just diagnosed or a family member was just diagnosed – and your health literacy was considered low, then this is probably a good starting point. It is certainly better than ‘a touch of sugar’, which are the words used by some healthcare professionals STILL when telling people what diabetes is.
I guess the dilemma for me – as someone who does a lot of writing about diabetes – is that I know that there are some people who want and need more information. Frequently, I write for people whose health literacy is of a higher standard, and there is a need to write at an appropriate level for this target group too. They want – and are able – to read technical and quite difficult jargon.
But I can never ever assume that is the case for everyone. When writing for this blog, I use language very much the way I speak – whatever comes into my head, thoughts going at a million miles an hour, lots of jargon and, if my hands weren’t flying across the keyboard, they would be flying around the air. It’s not really great for people whose health literacy is not high.
However, when writing for work, I am far more conscious of not doing those things. But I suspect, I am not conscious enough. Which is why I will be taking the pledge, and why I think this is a terrific initiative for those of us working in the health space.

This week is Jean Hailes for Women’s Health Women’s Health Week. (Yes, there’s a lot of women and health in that sentence, but given it’s the focus of the week, let’s work with it.)
I quite love the theme of the week which is Let’s Talk. The idea is that we get rid of the elephants in the room and talk about health issues that we sometimes find tough to discuss. It’s a great concept! Having people opening up – or at least being able to access information – about health issues that are sometimes not discussed is really important. Plus, there are gorgeous pink elephants all over the promotional materials and that can only be considered a good thing!
Now clearly, I don’t have an issue speaking about health issues. I very openly talk about my experiences living with diabetes. I have willingly and candidly spoken about fertility issues and miscarriage. I have also discussed the body image concerns that I have lived with for most of my life. Mental health is frequently discussed on my blog – usually in relation to diabetes.
But while I am happy to bang on about any health concern that I may be dealing with, that isn’t the case for everyone. That’s why this week is an important one.
And it is why we need people who are happy to share their stories out there. We need people to be discussing the things that are a little ‘underground’ or that make people squirm a little.
 Each day of the week has had a different focus. On Monday, the results of an online survey were released. The survey combined responses from 3,300 women aged between 18 and 87 years, and healthcare professionals including nurses, GPs and HCPs.
Each day of the week has had a different focus. On Monday, the results of an online survey were released. The survey combined responses from 3,300 women aged between 18 and 87 years, and healthcare professionals including nurses, GPs and HCPs.
Yesterday, the attention was directed towards natural therapies, looking at the safety and effectiveness of natural medications and treatments. There was great advice about questions to ask (yourself and your HCPs) before taking any natural therapies.
Today, it’s all about what is not being talked about. Starting with the difficult topic of domestic violence, the website provides advice about the issue and lists placed to go to for help. While there has been quite a bit of attention in the media given to domestic violence this year, the statistics are horrendous and we need to be doing more.
Also on the agenda for today is mental health and there are links to some valuable information about depression, anxiety and emotional health.
The rest of the week is about managing our health and healthy living.
I understand that not everyone is happy to share their story. And that is fine. But even those who prefer to stay silent and keep any health concerns to themselves still may look for information and advice. And shining a light on some of the less talked about health problems faced by Australian women with a bright and bold campaign does just that.
So. Let’s talk!
Every Sunday, in the Life magazine of The Age newspaper, is a column where people (usually B to Z grade celebrities) are asked about what they eat on a given day.
They all seem to follow the same boring, unadventurous, ‘this-is-what-a-dietitian-wants-to-hear’ diet. Usually, they start their day with lemon water (to help kick start their metabolism or help with their bodies pH or boost their antioxidant intake or cleanse their liver – it depends which pseudo-science crap they have been reading up on that week), which I am reliably informed (by, you know, qualified practitioners) does nothing other than potentially erode tooth enamel.
Mostly, the foods consumed by those lying about reporting what they ate include a lot of kale, brown rice, kale, grilled salmon, kale, green tea, kale, organic vegies, and kale. Because, kale.
It was in such an article that I first heard of Pete Evans with his ridiculous claims of activating his nuts.
The dietitian – the very sensible and very lovely Dr Joanna MacMillan – then usually comments that even though the person had lied reported eating well, they should try to incorporate more grains/leafy green vegies/lean meat/low fat dairy etc. in their diet to ensure they are following evidence-based dietary guidelines. There is (thankfully) often a ‘stop believing the crap you are reading’ message in there – and a reminder to stop eroding their tooth enamel first thing in the morning.
So, I thought I would write down everything I consumed on a recent day. And then translate it into the language used in these articles.
Breakfast
Caffe latte
Single origin organic coffee grown by virgins on an Ethiopian hillside, reverse-osmosis filtered organic water, organic milk from cows grazing on organic kale while piped music is played to them, fair-trade, organic, raw sugar grown under the organic sun and picked by night under an organic full moon.
Avocado toast
Two slices of artisan organic sourdough bread, evenly toasted by hand with a blow torch using organic butane, spread with organic avocado picked that morning, speckled with organic black sea salt from the organic Black sea.
Lunch
750ml pineapple juice (I had just mowed the lawn and was hypo. Really hypo.)
Pure filtered organic pineapple nectar, extracted by hand from an organic pineapple, naturally sweetened by smiling pineapple nectar extractor pixies.
Afternoon tea
Caffe latte
As above, but this time sweetened with organic agave syrup from Mexico.
Dinner
Homemade pasties.
Ratatouille of organically-grown baby vegetables including organic peas, organic potatoes, organic green beans, organic corn, organic onion, organic celery, organic spinach, organic zucchini, organic eggplant, organic garlic, organic turnip with organic micro-herbs wrapped in organic butter-pastry, gently baked until organically golden brown.
Salad of avocado, spinach leaves, sesame seeds and dressing
Avocado as above, organic baby spinach leaves picked just before becoming teenage spinach leaves, sprinkled with organic sesame seeds drizzled with a dressing of organic EVOO and organic balsamic vinegar.
Dessert
Three gluten free chocolate chip cookies (gluten free because the only flour-like product in my house at the time I had a sudden urge to bake was almond meal. Strictly NOT for any health benefits.)
Trio of gluten-removed organic dark chocolate shard biscotti made with gluten-free organic almonds, crushed by hand, baked into organic orbs of goodness.
Basically, my diet that day involved a couple of coffees, three quarters of a litre of pineapple juice, two slices of bread with avocado, a couple of pasties and three chocolate chip cookies. Not great at all. But honest.
And it was a good day, a healthy day. Because with everything I ate, I bolused insulin for it (not the pineapple juice – that hypo was terrible!). I ate what I chose to eat and then did what I needed to do to manage my diabetes. I took insulin. Or rather, sub-cutaneously infused organic insulin made by the delicate hands of Celtic insulin faeries.
National Diabetes Week is an important week for people living with diabetes in Australia. It is an opportunity to have all types of diabetes given attention and focus in the media and to talk about the significant health issue it is – for people living with diabetes, their families, and health systems.
And sometimes, messed up in the campaigns and the social media onslaught, we get sidelined by arguments and heated discussions, and we start to forget one of the real reasons this week is important: how diabetes affects those of us actually living with the condition.
Today, I helped launch a new report. The Diabetes MILES Youth survey was conducted last year and the results have now been published. The survey aimed to examine the impact of diabetes on young people living with diabetes and their families.
The report (which can be found here) shows that a quarter of young people living with type 1 diabetes experience moderate to severe depressive or anxiety symptoms. This image shows the top problem areas for girls and boys.
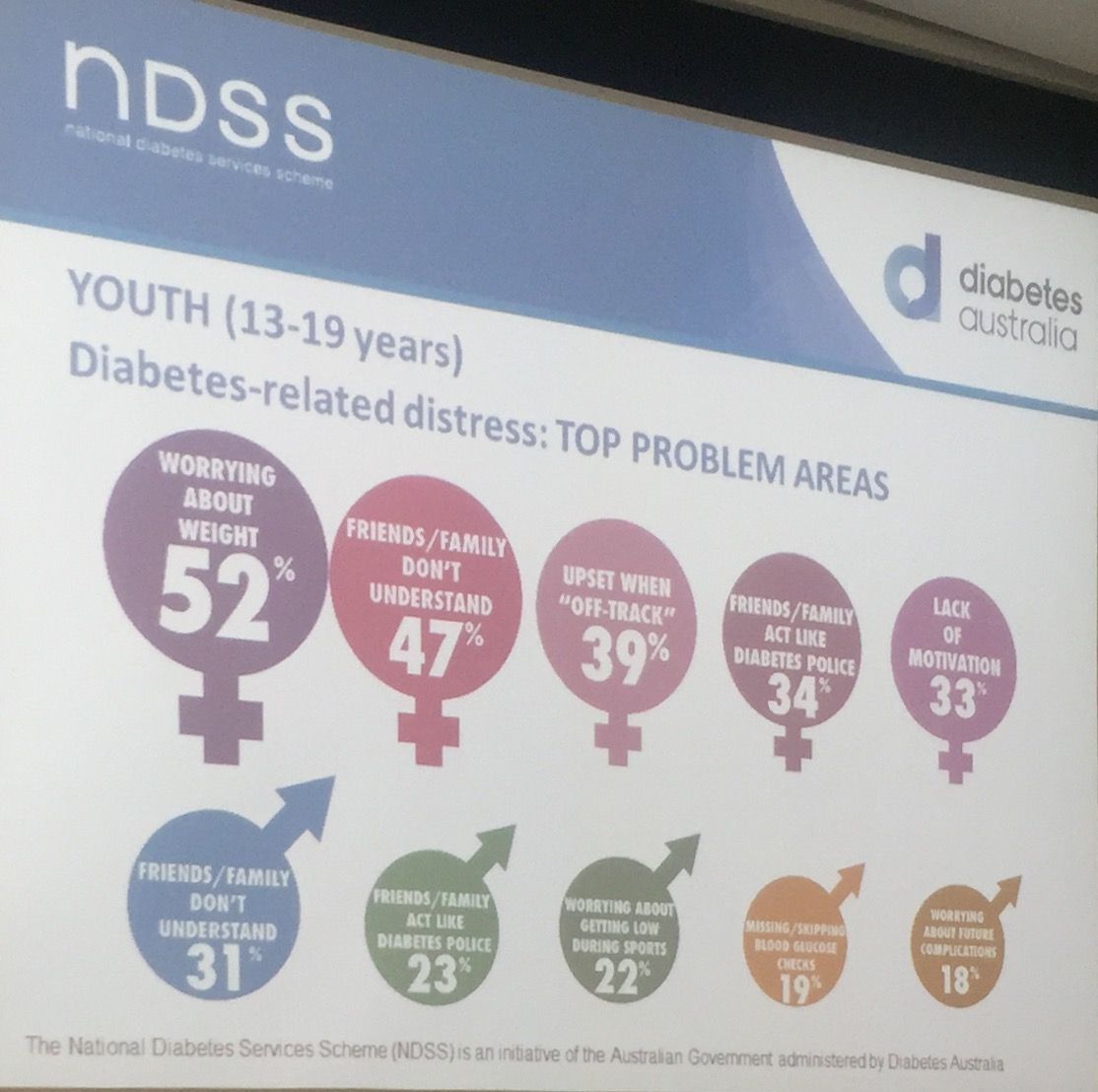
Today’s launch was incredibly powerful. Of course, we heard the statistics and heard how significant the problem is (a third of parents of children with diabetes reported impaired emotional well-being). And we heard about why this sort of work is important. But for me, and I suspect most people in attendance this morning, the most powerful moments were when we heard from Ryan Lange and Freya Wickenden, two young people living with diabetes. Both spoke beautifully about the role diabetes plays in their lives. Freya’s mum, Dallas, also spoke and shared some insights into parenting a child with diabetes.

As I said in my presentation at the launch – I can speak about this for hours and hours. I am a passionate advocate for all people with diabetes, but the vulnerability we see so often in young people with diabetes has meant that this has become a focus area of my work. But my words are insignificant and unimportant. It’s the words from young people living with diabetes that are central to understand what they are facing. Here is just some of what they told us.
The Diabetes MILES Youth report – was funded by the National Diabetes Services Scheme, and initiative of the Australian Government administered by Diabetes Australia. The study was conducted in collaboration with Australia Centre for Behavioural Research in Diabetes. The Diabetes MILES Youth project is part of the Young People with Diabetes National Diabetes Program for which I am Program Manager.






