
You are currently browsing the category archive for the ‘Diabetes’ category.
One of the highlight sessions I sat in on at ADA was Dr William Polonsky. Bill is the Co-Founder and President of the Behavioural Diabetes Institute, which you can read all about here. He also wrote the book Diabetes Burnout which is on the shelves of many, many people living with diabetes. I refer to it ALL THE TIME, and my copy has become incredibly dog-eared and annotated in recent times. And there was a period of about 6 months where I carried it around with me like a security blanket. (If you don’t have it, you can order it here.)
I’ve seen Bill speak at other conferences I’ve attended – he is one of the speakers I always make a point to hear because he absolutely ‘gets’ diabetes. His talks are always informative, amusing and offer great take-home messages for the mainly-healthcare professional audience. And he is gentle, kind and completely and utterly non-judgemental.
Yes – I am a complete and utter fan girl! But I did manage to keep myself together when I spoke with him a couple of times at the conference. And only slightly squealed when I heard he would be coming to Australia later this year. (Watch this space!)
His session at this year ADA had the title ‘Caring for the patient who doesn’t seem to care’ and right off the bat, Dr Polonsky highlighted the word ‘seem’ in the title.
He started by asking the audience how many of them had, in the past year, seen a patient who didn’t seem to care about their diabetes. Just about every hand in the room went up. Of course they did. Because for many – most? all? – of us living with diabetes, there are times when it all gets too much and we seem to not care.
But then he reminded everyone that even those who seem to not care about their diabetes want to live long, happy, healthy lives.
I don’t know anyone with diabetes – feeling good or not so good about their management – who isn’t hoping to be healthy. No one wakes up in the morning and says they want to have a crappy diabetes day. No one says ‘Diabetes is too much for me at the moment. I hope I have a really bad hypo.’ No one.
In times of burnout, where I absolutely know it looks like I couldn’t give a toss about my health, I wish so hard that I could find ways to break through the exhaustion and lack of motivation and find a way – any way – to do better at managing my diabetes.
Other take home messages from Bill’s talk included the importance of talking about diabetes with a sense of urgency – however without threats. I loved how he suggested a reframing of the oft-quoted ‘diabetes is the leading cause of <insert complication>’, reminding us all of the following:
Dr Polonsky’s take home messages from this talk were many. He provided some strategies for what might work – and some that should be avoided.
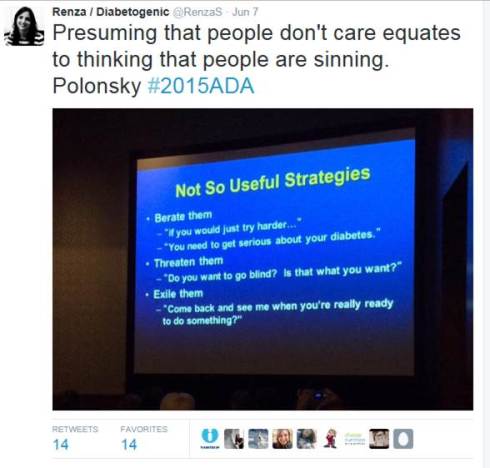
I listen to talks like this and think they sound so logical and sensible, and wonder why it even needs to be said. But of course it does. Because sometimes – all too frequently – there is this idea that not managing diabetes as expected is a deliberate choice. Or that not getting the results that we all ‘should’ be getting is the fault of the person living with diabetes. Thank you to Dr Polonsky – and others like him, including Martha Furnell, Jill Weissberg-Benchell and our very own Professor Jane Speight – for understanding that there is no fault here. Just a need for better understanding and support.

Being a total fan girl here! Dr Polonsky is my hero.
‘Are you here for work?‘ It was just after 7am in LA, and the border security officer looked tired. He studied my passport, holding it up, comparing the photo with the even-more tired-looking, and rather dishevelled, person standing in front of him.
‘Yes. For a conference in Boston.‘ I said, trying to smooth my hair.
‘Oh, the diabetes one?’
‘Yes. That’s right.’ I said. My flight from Melbourne was full of people attending the ADA conference. I know this because I knew half of them. Plus I kept hearing snippets of conversation with ‘diabetes’ being thrown around.
‘My mum (mom!) has diabetes. Type 1. She should go.‘ He said. He flipped through my passport. ‘How long are you here for?’
‘Only for the conference and then three days in New York. I’ll be home in nine days.’
‘That’s not long after travelling so far,’ he said to me.
I smiled. ‘You’re so right. But I’ve left my family home this time. So I don’t really mind only being away for a short time.’
‘Enjoy the conference.’ He stamped my passport and was about to hand it back to me when he looked at me again. ‘Do you have diabetes?’
‘Yes. I do,’ I said. ‘I have type 1. Like your mum.’
‘Do you use a pump?‘ he asked.
‘Yes. And I’m wearing a CGM as well.’
‘My mom needs to talk to you,’ he said. ‘You look healthy. Keep it up.’ He passed me my papers.
‘Thanks. I hope your mum is okay,’ I said, noticing the concerned look on his face – one frequently worn by loved ones of people with diabetes. He nodded and I walked off, heading towards the baggage carousel.

A typical, frantic, ‘I’m so disorganised’ few hours before getting to the airport. But I have insulin. And I have a CGM fastened to my stomach and an insulin pump tucked in my bra. There are pump supplies in my carry on. Anything else I’ve forgotten can be found easily at the other end.
Don’t forget to follow #2015ADA!
Tomorrow, I am flying to Boston to attend the American Diabetes Association 75th Scientific Sessions. (Play along from home by following #2015ADA!)
There will be a strong consumer (reminder to self – use ‘patient’) contingent, which is always terrific. I get to catch up with old friends from the DOC and hear what they have been up to. I learn about new consumer patient-led advocacy efforts that manage to cut through in a way that only people living with diabetes can. I am reminded that conferences ARE the place for people living with the health condition that is being spoken about at that conference.
I attend conferences with my eyes wide open and leave with great excitement. I see new technologies yet to be released here, or still in development. I hear from people on trials of new drugs and devices. And I see the potential and possibilities for making diabetes easier, more streamlined, more user-focused and feel inspired and hopeful. This is good.
But, I am approaching this conference with a slightly different attitude. With some of the recently announced changes to diabetes supplies in Australia (as I wrote about here and here), I really want to speak with some of my US DOC friends about what it means to be reliant on a health system that limits choice. We have never really had that to date.
Whilst we may not have access to every pump or meter on the market, the consumables for the devices that are here have been available to all. Distribution has been overseen by Diabetes Australia (please read the disclaimer in this post!!) – an organisation representing people with diabetes, not big business or shareholders.
Last night, I attended a dinner at Parliament House in Canberra for the Parliamentary Friends of Diabetes Group. It was a grand occasion, attended by many influential politicians. Health Minister, Sussan Ley made this comment:

This is, indeed a noble pursuit.
Diabetes Australia President, Judi Moylan stated:

I would ask that in amidst all of those politically-charged reviews, reports and cost-cutting measures that seem to be the focus of diabetes in Australia at the moment, the human aspect is identified. It is hard to find amongst all the facts and figures.
But it is absolutely critical for our leaders to consider if they want to do best by people living with diabetes. Extraordinary leaders would search for it, find it – and make sure they listen to it. And remember that those extraordinary leaders include people living with diabetes.
If you have diabetes and live in Australia, it is highly likely that at some point you would have received some information, support and/or education from Diabetes Australia.
These services range from the provision of information via websites, blogs, magazines, information sessions and webinars. They also involve activities such as camps for children with type 1 diabetes, peer support groups, targeted information sessions which look at issues including men’s health, women’s health (including the very important topic of pre-conception planning and care), programs for young people with diabetes, programs for older people with diabetes, including those in nursing homes, working with culturally and linguistically diverse groups, delivering programs to Aboriginal and Torres Strait Islander communities and the training of health professional training.
More? Well, there is also a huge body of advocacy work – both at an individual and policy level – that takes place, as well as representation on expert panels and working groups.
Yesterday, it was announced that the Government has signed the 6th Community Pharmacy Agreement (6CPA). This agreement covers the supply of PBS medicines and, more broadly, pharmacy remuneration for dispensing subsidised medicines.
A significant change in 6CPA from previous agreements is that from July 2016, NDSS products will be distributed through the pharmacy wholesaler distribution network. This is where it starts to affect people living with diabetes.
Basically, the NDSS is broken into two parts. There is the product supply and delivery component and then the support services component. The latter is where all those things I listed earlier in this post fall.
Okay – let me get the disclaimer palaver out of the way. I work for Diabetes Victoria (formerly Diabetes Australia – Vic). I also have a national role where I work for Diabetes Australia. I am a long standing member of the Diabetes Australia family – something of which I am incredibly proud. My work involves providing information and support services to people living with diabetes in Victoria, and managing a national project about young people and diabetes. I am a spokesperson for the organisation – especially about diabetes technology and social media. I do all these things backed by a team of health professional and consumer experts.
Right – with that out of the way, I will also say that I have no more information than what is available in the public domain, so this is not an opportunity for me to be sneaky in trying to get people talking about this to promote Diabetes Australia’s work. That’s not what this is about. This is about what it means to people with diabetes living in Australia. Because I am one of those people.
The 6CPA clearly outlines that product supply and delivery (that is, all the consumables we use to help manage our diabetes) will now be distributed through the pharmacy network. As a person with diabetes, I am confident that this means that the supply of these products is protected (along with the subsidised prices) and that I won’t be expected to pay more for my strips or pump supplies.
But what about ongoing education and support services? Diabetes Australia has a long history of providing evidence-based information. In recent years, there has been a very strong focus on patient-centred care, and most programs now have some sort of consumer input. Engaging people living with diabetes is considered just as important as engagement with healthcare professionals. I know this is true – I am frequently asked to either be a consumer rep, or (perhaps most pleasingly) assist with finding someone to be a consumer rep.
The provision of diabetes information needs to be done by people who ‘get’ diabetes. I am a really strong believer of this. I believe it to be true of all health conditions – there need to be experts (and that doesn’t only include clinical experts) at the helm. And there needs to be a strong link to the community.
These services Diabetes Australia provides change lives – I hear that every time I speak with a parent whose kid has been to a camp. I heard that – repeatedly – on Saturday at the Diabetes Expo where I was emcee. I hope this carries on.
I got to Saturday evening and felt like I needed to collapse! I was more than a little diabetes-ed out. The end of last week and the beginning of the weekend were huge – attendance at a health professional event on Friday, the Diabetes Expo on Saturday and, of course, the gift that keeps on giving, the television thing on Thursday.
When diabetes is so front-and-centre, it is really tough to think clearly and about all the information that has been shoved into my itty-bitty mind. Stopping and searching around for some things I have learnt and taken away can be difficult. Which is why Twitter is good!
Here is what I learnt over the last few days.
People want information about diabetes. There is still so much misinformation out there that people living with diabetes sometimes have a hard time cutting through the noise and working out what is valuable info and what is made-up-psuedo-science-crap-from-some-idiot-trying-to-sell-you-magic-beans-to-cureall. So it’s good to have sensible people saying sensible things! (Hashtag – Evidence)

 And I also learnt that diabetes is still seen and considered by too many as a clinical condition and there is not enough attention given to the emotional impacts of living with it.
And I also learnt that diabetes is still seen and considered by too many as a clinical condition and there is not enough attention given to the emotional impacts of living with it.

Thankfully though, I was reminded that there are people out there who can help with this!

I learnt that Twitter trolls will latch onto hashtags that are getting some attention and try to infiltrate it with their nonsense. These trolls should be ignored. Except, of course, I didn’t. (However, I will not share your Twitter handle here!)

And these nutters will try to discredit you by challenging your Nutella addiction. Fools!

I was reminded why the Herald Sun is not the place to go for credible diabetes information.
And promised baklava from one of Australia’s leading researchers in diabetes. Thanks Sof!
I learnt that it’s surprising who watches morning magazine television shows. Like the uber-cool waiter at Marios who announced loudly as we walked into the café yesterday, ‘I saw you on TV’!
I remembered that people walk away from these sorts of events feeling positive and rejuvenated and connected. Which makes them worth it in a million different kinds of ways.


And I learnt that after a hugely successful few days of work activities that hanging out with my family, listening to Carol King and drinking coffee in my favourite café and then watching the Eurovision song contest final will make me feel energised and ready to face the new week.
Hello Monday!
I know it’s not Friday, so here is something for your MONDAY listening pleasure!
Yesterday, as I sat in the waiting room to see my endo, I couldn’t help but feel that I was walking into a wasted appointment. I had seen her about six weeks earlier and left with promises to myself of being more engaged with my diabetes care. I promised I would have my blood work done. I thought about goals and how I could work to achieve them.
And yet, there I was, waiting to go in and wondering what the hell I had to say to her. There would be no discussion of lab results. I haven’t gone to pathology to have the checks done. There wouldn’t be any pulling out of data for me to show her – I hadn’t been logging anything. I was pretty much in the same state of mind about my diabetes as I had been last time I sat waiting to go in to see her.
I was wasting her time and I felt really bad about it. Not that she would ever tell me that. In fact, not that she would even be thinking that. But it’s how I felt. I have such respect for this endocrinologist, and I felt that in some ways I was actually being disrespectful in showing up so unprepared.
There were no tears yesterday. But there was an honest and open admission from me that I need help. I have tried everything I know to try and pull myself out of the motivation slump I have been in for so long. There are been periods where things seem to be better and I am able to make more of an effort, but they are fleeting and before long, I am back to feeling burnt out.
Let me be clear – I am not completely ignoring my diabetes. I am bolusing insulin at all the appropriate times; I check my blood sugar, albeit nowhere near as much as I know I need to – or that I would like to; I have started seeing my endo again. I eat well. At no time has diabetes completely fallen off the radar. But it certainly has deviated from being as much of a focus as I would like.
It’s not the mechanics of diabetes that is the problem. It is the trouble-shooting and problem solving and thinking about diabetes in a way that makes me feel confident that I am dealing with my health and wellbeing as much as my blood sugars. But I’m not doing that. I’m in a fog of burnout from which I now know I am unable to emerge without some real help.
I can pinpoint the source of the burnout; I can trace its progression; I can see why it happened. I understand all of that. I understand that dealing with the loss of our baby following a miscarriage and all the things that happened around it were often all I could deal with – both at the time and for periods since then too. But even though I have words to explain how this has happened, I don’t have actions to get me out of it.
I’ve tried. I’ve tried everything I could think of – all the techniques that have worked in the past. But I suspect that the combination of grief and the longevity of this burnout have resulted in me simply not being able to fix it alone. I need help.
I also believe that tied up in all of this is the way that I am feeling about my body and its failings. Because I do feel I have failed. Or at least my body failed me – again – when I miscarried. I really did think that I was ‘over’ it and was moving on, but not a day goes by where I don’t, in some way, feel sad and broken about it. I don’t know how to stop feeling this way. Again, I need help.
So, I asked for a referral to someone who can help me work though things – someone to help with strategies. I have been in therapy before; I know that it will help. It’s not a quick fix – I know that too.
I am trying to be all Pollyanna-ish about this and make grand ‘the first step is the hardest’ statements. And I am being positive and saying that it is certainly a step in the right direction. It’s going to take time. It’s going to take effort. Perhaps I am ready for that now. I know I certainly haven’t been to date. But maybe – hopefully – I am now.
Today, diabetes can bite me. I changed out a perfectly good – and working perfectly – cannula this morning because it had been in for four days and I sometimes follow some diabetes rules.
Fresh out of the shower, I stabbed in my line and knew straight away something wasn’t right. I am more than used to (and expect) the little sting that comes with the introducer needle piercing my skin. But this one really hurt. And then when I primed one unit of insulin into the empty cannula it hurt. Really hurt.
So, I ripped it out. Which was a good idea! I present exhibit A:

This resulted in swear words galore because I am classy and a lady. I pulled another infusion set from the cupboard, ripped it open and shoved it in my skin. And again – ouch! I didn’t even bother to prime it – I just ripped it from my skin. Which again, proved a good idea. I present exhibit B:

Ripping this one out was fun. It bled. Down my leg and onto the floor. So I swore again (more classy, more lady) and cursed the diabetes gods and possibly stamped my foot. Actually, I definitely stamped my foot. And threw the useless thing across the room at which point the puppy thought it had a new play toy.
The next cannula went it without a hitch and is behaving itself. Third time lucky.
So, what did I learn from today’s exercise? Not much. Probably that I shouldn’t follow diabetes rules and should have left the four-day-old-slightly-manky-but-working-perfectly cannula in. Because nothing good comes from following rules. Yep. That’s what I’m taking away from this. Also, I need a cupcake.
Go away. There is nothing to see here today.
Instead, enter #IWishPeopleKnewThatDiabetes into your search engine and spend the day reading about the things we all want everyone to know about diabetes.
This is the initiative of Kelly Kunik from Diabetesaliciousness. But don’t read her blog today either. You can do that tomorrow.
Today it’s all about this hashtag: #IWishPeopleKnewThatDiabetes
Go!

I could never ever work in advertising. A combination of cynicism and disbelief at anything I ever see in an ad would make me a difficult employee!
There is a very real gap between the truth of diabetes and what we see in advertisements for diabetes products. I frequently find myself shaking my head in disbelief at the way diabetes is portrayed.
This is what a stomach using an insulin pump looks like. That is my stomach (apologies if you are eating, drinking or just looking). Those dots are the ghosts of infusion sets past in various stages of healing. There is also probably some tape residue stubbornly stuck to my skin. Pretty (gross), isn’t it?

#NoFilter. Obviously
This is what a stomach in a pump ad looks like. Magically, any hint of previous infusion sites have disappeared.

This morning, here is what my meter announced my BGL to be. (Hashtag: fuckoff)

This is what the reading on pretty much every box and poster of BGL meters looks like. (Hashtag: bullshit)
 CGM graphs in real life look like the trajectory of rollercoasters with mountainous highs and cavernous lows, while the slick promotional materials show straight lines, nicely fitting in between the upper and lower alarm limits.
CGM graphs in real life look like the trajectory of rollercoasters with mountainous highs and cavernous lows, while the slick promotional materials show straight lines, nicely fitting in between the upper and lower alarm limits.
People in advertisements for diabetes paraphernalia are always outdoors, happy and rolling down hills, big smiles plastered on their faces. They wake up looking well-rested.
Real people with diabetes may spend time smiling and happy (I love rolling down hills – especially at this time of the year and getting all covered in Autumn leaves), but I’m putting it out there and saying that their glee is not because they have just done a BGL check. Unless the result is 5.5mmol/l. Each and every time. (See about meter photo. There was no smiling at that!)
I get it. No one wants to see my stomach on an ad for insulin pump therapy – that’s not selling units of product! But surely there needs to be a middle ground somewhere. I would like there to be an occasional BGL reading of over 15mmol/l on a poster for a meter. Because it happens. It’s not the end of the world and it doesn’t mean the meter is crap. And a stomach with a few pock marks from old infusion sets doesn’t reflect the quality of the infusion set. It reflects reality.
Diabetes isn’t pretty. It’s an ugly, scary and pretty un-fun thing to live with a lot of the time. That doesn’t mean that I spend most of my time in a ‘pity me’ funk, but I do admit – quite honestly – that it is shit at times. How about we aim for a bit of honesty and truth in diabetes advertising? Telling it like it is doesn’t mean we are weak or showing defeat. It’s just being authentic.







{kind=link}