
You are currently browsing the category archive for the ‘Diabetes’ category.
Over the weekend, an embargoed press release arrived in my inbox with a few different pieces of research that would be presented in coming days at EASD.
Being registered as press for diabetes conferences means getting an advance peek into some of the big stories that are likely to generate a lot of interest and discussion. This email offered three or four pieces of research, but it was the first one listed in the subject heading that made me catch my breath and hesitate on the button to read the email beyond the header,
Shorter. Life. Expectancy.
The three words ran through my mind over and over before I steeled myself enough to open the email and read the release, then the abstract and finally the full article. As confronting as the email header was, there was nothing in there that I didn’t expect, and nothing really that surprised me. It’s not new news. I remember being told early into my diagnosis that I could expect to live 15 years less because of diabetes; something I casually announced to my sister one night when we were out for dinner. Through tears, she made me promise to never say that again, and I just hope she’s not reading this right now.
But even though there was nothing in there that made me feel especially concerned, I did bristle at the conclusion of the article, in particular this:
‘Linking poor glycaemic control to expected mortality … may incentivise … people with diabetes and poor control to increase their efforts to achieve targets.’
I’m ignoring the language here, because even more problematic than the specific words in here is the sentiment which I read as ‘scare people and threaten them with early death to try harder’. Unsurprisingly, I find that horrendous. Equally horrendous is the assumption that people are not already trying as hard as they possibly can. It’s not possible to increase efforts if someone is already putting in the maximum.
Over the last twenty-two years, my diabetes management has sat at pretty much every single data point along the ‘glycaemic control’ spectrum, from A1Cs in the 4s and 5s all the way up to the mid-teens. There is no way that being told that I was going to die earlier would have made me pull up my socks to do better. In fact, it’s likely that if anyone had, at any point (but especially when I was sitting way above target), told me that I was sending myself to an early grave, all that would have done was send me further into the depressive burnout hole I was already cowering in.
It’s tough going knowing that the health condition that I’m doing everything in my power to manage as best as I possibly can is going to contribute to cutting my life short; that despite those efforts, I am likely to see fewer years of my daughter’s life and be outlived by most of my friends. Placing any of the blame for that on me for that makes me feel even worse.
I’m not here to argue with the article – it was an analysis of an audit of data out of England. I’m not here to say that this sort of information shouldn’t be shared, because of course it should be. Understanding outcomes, what drives them, interventions that can help and any other factor that provides better results for people with diabetes is a brilliant thing. These sorts of results could be used to highlight when and how to intensify and prioritise treatment options.
I do, however, question the way that the information will be used. Also, from the article:
‘Communication of life years lost from now to patients at the time of consultation with healthcare professionals and through messages publicised by advocacy groups … and … national/international patient facing organisations will be of great help in terms of disseminations of the conclusions of this study.’
I would be really dismayed if I saw any diabetes organisation using this information in a comms campaign, as I fear it could add concern and trauma to people living with diabetes. I worry about how it could be interpreted by well-meaning loved ones to say, ‘If you don’t start looking after yourself, you’re going to die,’ or something similar.
For the record, one of the other studies highlighted in the email was about hot baths and diabetes. The lowdown on that is having regular hot baths may improve cardiovascular risk factors in people with type 2 diabetes. I’m going to do an n=1 study to see if that also helps people with diabetes.
This week, it’s EASD. It’s is the first year since 2012 that I have not been in Europe for the meeting. EASD was the first large diabetes professional meeting I had ever been to, and I remember being struck at that very first one in Berlin by the stark absence of people with diabetes on the program and involved in the actual meeting.
My, how things have changed.
Except, of course, they haven’t. Sure, these days you will see growing numbers of PWD wandering the conference centre and attending sessions, but that really is only because we created opportunities for PWD to attend. And once we found a way to get there, we then made sure that we were visible in different ways such as leading social media charges and holding events open to all attendees.
There has been some very well placed and relevant conversation on twitter about the lack of diversity in the EASD organising committee. Too few women; too many white faces. But when we talk about inclusion, surely, surely we need to look at other groups that are significantly and obviously absent. Where are the advocates on there? Where are the BIPOC with diabetes? Where are people living with both diabetes and disabilities? Where is there representation from the diabetes LBGTIQ community? All of these factors impact on diabetes management, so wanting to see presentations that address them makes sense. And where is the lived experience on the program to underline, and provide real relevance, to the work that is being presented by HCPs, researchers and academics?
You bet there should be more women and more BIPOC on the organising committee for EASD. But if those on the committee, those doing the research, those HCPS seeing PWD truly want to beat the ‘person-centred’ drum, PWD need to be part of the group of people putting the conference together, and then strongly represented on the stage too.
#NothingAboutUsWithoutUs seems to STILL be missing from this whole meeting – from the organisation right through to the actual delivery of information. (I suspect that there may be some PWD on the program who are HCPs. While that is terrific, it is very different from having advocates who are not HCPs up on stage.)
So, this week, if you can, please support initiatives that do highlight the people who are actually living with diabetes. Please check and double check the times. I’ve tried to work out the AEST start time for all of the events, but don’t take my word for it! (Disclosure statement at the end of this article.)
#docday° & #dedoc° voices
This is the eleventh (I think??) #docday° event and I am so proud to say that I have been involved in every single one of these events. The first one was held in the back room of an overheated and overcrowded café in Stockholm five years ago. It feels like yesterday, and a lifetime ago all at once. Organiser, Bastian Hauck, asked me to say a few words, and this is what I wrote in a blog post about the event:
‘I highlighted for me what is the most important thing when we are talking about the DOC: No one owns this community. No one is more important or more relevant or more powerful. Sure, some of us are very fortunate that we get to actually meet IRL and attend conferences, but we do it as part of our jobs – whether it be like me (through my work at a diabetes organisation mixed with my online work) or through independent consulting or other work. But regardless if you are in the room or following along on Twitter, everyone has the same right to be here and to be part of it.’
We have livestreamed #docday° events in recent years, and I have written about most of them, and done all I could to encourage as many people as possible to come along and join in. This year, it will once again be livestreamed from the #dedoc° Facebook page from Tuesday (today) 12pm CET tonight, which is 8pm AEDT.
Also, make sure you keep an eye out for all the terrific advocates who received a scholarship to attend EASD via the #dedoc° voices program. They are sharing what they are seeing at the meeting on a variety of social platforms.

SOLVABLE PROBLEMS IN DIABETES
A few hours later, diaTribe will be continuing the Solvable Problems in Diabetes events which have been regular satellite events at European diabetes meetings in recent years. During COVID times, these events have been kicked off with a community focus event, showcasing diabetes advocates, which is a brilliant (and necessary) addition to the HCP discussion that follows. I’m a huge fan of diaTribe, and have been for a long time, but it has been the addition of Cherise Shockley to their team as Community Manager that has seen a wonderful increase in representation of PWD in their activities. But, of course it has. Cherise is all about community and the way she has been able to weave her magic to make diaTribe even more relevant to PWD – and more representative – is what she does best. You’ll need to register for this event (it’s free) here, and it kicks off at Tuesday 11.30am ET, which is (gulp) Wednesday 1.30am AEDT.

SEPTEMBER SESSIONS
While not part of EASD, Beyond Type 1 is hosting the next in their Summer Sessions and this week it’s focusing on racial and ethnic disparities in diabetes care. There is an absolutely stellar line up in this webinar. Please do follow along if you can – this event will also be via Facebook Live over at Beyond Type 1, and is on Wednesday 8pm ET, which is Thursday 10am AEST.

DISCLOSURES
- I am ad advisor to the #dedoc° voices program. I do not receive any payment for this role.
- I am speaking at the Solvable Problems in Diabetes Community Focus Sessions. I am not receiving any payment for my involvement. I am a regular contributor to diaTribe, and I am paid for commissioned articles.
- I am on the Leadership Council for Beyond Type 1. I do not receive any payment for this role.
For more information (all Australian sites):

Diabetes conferences and scientific meetings in 2020 have looked very different than in previous years. It looked as though we were off to a flying start with a successful ATTD in Spain back in February. But not long after all the attendees returned to their corners of the globe, the world turned upside down and decided that, along with everything else, in-person meetings were done.
Major professional conferences such as those run by ADA, DUK, EASD, ISPAD, ADS & ADEA and IDF have all either happened, or will be happening, virtually, with a Zoom (or other) platform being where we meet, rather than a massive conference centre in a major city.
As ever, I search for a silver lining and if there is one it is this: the pivot to virtual conferences means that some of the main barriers in the way preventing PWD attending diabetes conferences are somewhat reduced. With travel, accommodation and a lot of the other expenses out of the way, it may be easier for advocates who would like to attend to find their way in. Let’s look at that as the disruption we needed to have to get PWD flocking to meetings in droves.
There is still the matter of registration passes, and we know that is not always the easiest thing to overcome. The registration fee is significant, and some conferences only allow HCPs and researchers in. Usually, press passes provide a way to get passed security, but they require letters of assignment (sometimes from diabetes organisations who ask PWD to act as ‘on the ground’ reporters), or other criteria be met. And, of course, there are invitations to attend satellite events extended from device and drug companies to some advocates. While there is often criticism at these methods, they have meant that there are PWD at conferences, many of whom provide information back to the community.
At ATTD, there was a new way in. Advocacy group #dedoc° launched a new program, #dedoc° voices, which you can read all about here. For the pilot of the program in Madrid, the diabetes advocates whose applications were successful had access to all parts of the meeting.
#dedoc° voices is happening again for EASD (coming up next month), and it’s not too late to apply. And as an added bonus, successful applicants will also receive registration to the ISPAD conference in October. ISPAD is the International Society for Pediatric and Adolescent Diabetes, so if you are a parent of a kid with diabetes involved in advocacy and peer support, you may be super keen to attend this one.
To apply, go here. #dedoc° voices is open to PWD now, so if you have always wanted to attend a major diabetes conference, there is nothing stopping you from applying, right now. Any one from anywhere around the world can apply – the only consideration is how you’ll manage time zone horrors if you don’t live in the same zone as the conference. (But please don’t come crying to me about that – I’ve spent the last six months settling in for hour long meetings hosted out of Europe of the US which begin long after sunset and involve perky people just waking up while I yawn and struggle not to fall asleep in my Zoom square!)
What are you waiting for? Apply now and come be a part of one of the biggest diabetes meetings in the world. I promise there will be lots of other PWD there for you to (virtually) meet up, and share ideas with. Come say hi!
Disclosure
I am an advisor to the #dedoc° voices program. I do not receive any payment for this role. 
This was one of the first things I saw when I opened my email this morning: the lead article in the latest edition of The Limbic – ‘Subsidised CGM has not improved outcomes in Australian children with T1D’.
I’m relying on the The Limbic’s commentary as the study is not open access (I have requested a copy from one of the authors), and according to the report, the focus of the study was improvements in A1C and reductions in severe hypoglycaemia.
It will come as no surprise to anyone who has read anything I have written about technology or heard me give one of my many, many talks on user experience that I found this report problematic. Screaming that a well-funded and hard-fought for program, providing much needed diabetes technology to children (and adults) is ‘underwhelming’ does not sit well with me at all, especially when the main way the program’s success has been evaluated is a highly flawed clinical measurement.
When I look at the benefits I list when it comes to using any sort of diabetes tech – or other diabetes management, whether that be a drug, an education program or even peer support – changes to my A1C is far down on the list. I understand that for some people, this is certainly a measure of success, but it is not even close to one of the first things I would consider.
My history of using diabetes technology is long and elaborate. Perhaps one of the best examples of just why A1C gives a very incomplete picture of how I measure success is my initial foray into using an insulin pump. It was almost 20 years ago, and I was only three years into living with diabetes. That story is one that could be used as an example of ‘How NOT to do pump therapy’.
I was educated (and I use that term very loosely) by a rep from the pump company. She talked at me for three hours, pressed buttons, loaded some numbers into the device and then stepped out so a dietitian could teach me all I needed to know about carb counting. She was in the room for forty-five minutes. (For context, this was my introduction to carb counting, because my first dietitian encounters were only about low GI, with a general direction of ‘Eat as much as you want of it as long as it is low GI’).
I was released from the hospital with this new device strapped to me, step by step instructions for how to do a cannula change in three days’ time, and absolutely no idea what I was doing.
But here’s what happened: I could sleep in again. I didn’t need to eat unless I really wanted to; eating by the clock became a thing of the past! I could eat brunch out with friends again, without having already had breakfast at 7am. I ate more of the foods I wanted to and stopped stressing out each time I sat down for a meal. I felt more relaxed. My life felt just a little bit more mine, rather than dictated to my a most unwelcome health condition. And sleep! Did I mention sleeping in?
My A1C was the highest it ever was. By all clinical measures, I was absolutely messing this up. But by my measures – which were based on how I was feeling, how emotionally robust I was, how burnt out I felt, how late I could sleep in on the weekend (I see a theme) – I was ticking every single box.
My endocrinologist told me that I was wasting my money (and his time) being on a pump, and nothing I could do to explain that for the first time in three years I felt like myself. Sure, I knew that I had work to do on my A1C, but I finally felt emotionally resilient enough to do that. He just shook his head and sent me on my way…and was promptly sacked.
(Luckily for me, the story ends well because about eight months later, I came across a woman called Cheryl Steele. Suddenly I could use a pump properly. My A1C came down; my quality of life remained elevated.)
My story is not uncommon. I have spoken with dozens and dozens of people who have benefited from the CGM initiate and overwhelmingly, the stories I hear are people who are grateful for the tech for what it has offered them. Interestingly, we rarely talk about those measures that HCPs and researchers seem to think are the best way to gauge the success of any sort of intervention. They talk about those same things I mentioned earlier. When the CGM initiative was first launched, parents of kids with diabetes told me they had slept for more than three hours at a time at night for the first time in years. They told me how they stopped fearing hypoglycaemia so much, because they were being alerted if their kids glucose levels were trending downwards. They told me that their kids were having sleepovers and heading off to school camp for the first time.
A1C? Maybe we would mention that somewhere down the track, but that wasn’t what got us the most excited. That wasn’t the bit we spoke about when we uttered the words ‘life changing’.
Obviously, research is important. Data is essential. It was data that provided the strong case for Diabetes Australia, JDRF, ADS, ADEA and APEG to advocate for CGM funding as part of the NDSS. But the case that was put forward also included research that looked at QoL, because the organisations know that this matters.
Research that focuses on A1C is always going to be problematic in a health condition that will never only be about that number. It’s problematic for a number of reasons – not just because it gets my shackles up before I’ve had my morning coffee. We know the pot of money that goes to supporting and funding initiatives, such as the one in this study, is very limited. Funding authorities don’t have the nuanced understanding of all the different interventions that need funding, so if a study like this comes across their desk, it could raise red flags.
I am not for a moment saying that this sort of research should not be conducted or that negative results should be buried. What I am saying is that any results need to be flagged as only ever presenting part of the issue as a whole.
I am looking forward to reading the whole study – and truly, I’m hoping that this blustering post is all a waste of time because somewhere in there, I will get to see that the researchers spent a fair bit of effort evaluation QoL as well. I’m hoping that the trumpeting heading from The Limbic is nothing more than their typical sensationalism.
My fear, however, is that there won’t be more, and that once again, PWD will have been reduced to nothing more than a flawed metric that shows only one corner of the picture of our lives with diabetes.
I’ll finish with one final thought. I advocate for PWD’s involvement in every single step of diabetes research (not just as participants of studies), and one of the reasons I do that is because when we are at the table when studies are being first mapped out, we are given the chance to remind those conducting the work that the answers they are seeking are coming from people. Real people who will always be far more than their diabetes. And somehow, that needs to be reflected in the study they are doing. It can be done. Unfortunately, this seems to have missed the mark.
At the best of times, I’ll celebrate any kind of anniversary, but it seemed even more important to acknowledge my ‘loopiversary’ this year in what can really only be termed as the most fucked of times. Last week, I clicked over three years of looping, a decision that remains the smartest and most sensible I have ever made when it comes to my own diabetes management.
In reflecting just how Loop has affected my diabetes over the last three years, I’ve learnt a few things and here are some of them:
- The words I wrote in this post not long after I’d started looping are still true today: ‘…this technology has revolutionised every aspect of my diabetes, from the way I sleep, eat and live. I finish [the year] far less burdened by diabetes than I was at the beginning of the year.’
- The #WeAreNotWaiting community is but one part of the DOC, but it has provided the way forward for a lot of PWD to be able to manage their diabetes in ways we never thought possible.
- Even before I began to Loop, the kindness and generosity of people in that community was clear. I took this photo of Dana and Melissa, two women I am now lucky to count amongst my dearest friends, at an event at ADA, just after they had given me a morale boosting pep talk, promising that not only could I build loop for myself, but they would be there to answer any questions I may have. I bet they’re sorry they made that offer!

- Loop’s benefits are far, far beyond just diabetes. Sure, my diabetes is easier to manage, and any clinical measurement will show how much ‘better’ I am doing , but the fact that diabetes intrudes so much less in my life is, for me, the real advantage of using it.
- That, and sleep!
- I get ridiculously excited when other people make the leap to looping! I have watched friends’ loops turn green for the very first time and have wanted to cry with joy because only now will they understand what I’ve been ranting about. And experience the same benefits I keep bleating on about.

- It’s not for everyone. (But then, no one said it was.)
- You get out what you put in. The more effort and time and analysis you put into any aspect of diabetes will yield results. But with Loop, even minimal effort (I call the way I do loop ‘Loop lite’) means far better diabetes management than I could ever achieve without it.
- It took an out of the box solution to do, and excel at, what every piece of commercial diabetes tech promises to do on the box – and almost always falls short.
- It’s amazing how quickly I adapted to walking around all the time with another but of diabetes tech. My trusty pink RL has just been added to the phone/pump/keys/ wallet (and, of course, mask) checklist that runs through my head before I leave the house.
- Travelling with an external pancreas (even one with extra bits) is no big deal.

- I was by no means an early adopter of DIY tech, but I was way ahead pretty much any HCPs (except, of course, those living with diabetes). The first talk I gave about Loop still scars me. But it is pleasing to see that HCPs are becoming much more aware and accepting of the tech, and willing to support PWD who make the choice to use it.
- The lack of understanding about just what this tech does is astonishing. I surprised to still see people claiming that it is dangerous because users are ‘hacking’ devices. Language matters and you bet that this sort of terminology makes us sound like cowboys rather than having been thoughtful and considered before going down the DIY path.
- The lengths detractors (usually HCPs and industry) will go to when trying to discredit DIYAPS shouldn’t, but does, surprise me. The repeated claims that it is not safe and that people using the tech (for themselves or their kids) are being reckless still get my shackles up.
- Perhaps worst of all are those that claim to be on the side of those using tech, but under the guise of playing ‘devil’s advocate’ do more damage than those who outwardly refuse to support the use of the technology.
- The irony of being considered deliberately non-compliant when my diabetes is the most compliant it ever has been hurts my pea-sized brain. regularly.

- There is data out there showing the benefits and safety of looping. Hours and hours and hours of it.
- My privilege is on show each and every single time I look at the Loop app on my phone. I am aware every day that the benefits of this sort of technology are not available to most people and that is simply not good enough.
- Despite all the positives, diabetes is still there. And that means that diabetes burnout is still real. But now, I feel guilty when feeling burnt out because honestly, what do I have to complain about?
But perhaps the most startling thing I learnt on this: The most variable – and dangerous – aspect of my diabetes management has always been … me! Loop takes away a lot of what I need to do – and a lot of the mistakes I could, and frequently did, make. Loop for me is safer and so, so much smarter and better at diabetes than I could ever hope to be. I suspect that as better commercial hybrid closed loop systems come onto the market, those who have been wary to try a DIY solution will understand why some people chose to not wait.
And finally, perfect numbers are never going to happen with diabetes. But that’s not the goal, really is it? For me, it’s about diabetes demanding and being given as little physical and emotional time and space in my life. With Loop, sure numbers are better – but not perfect – and I do a lot less to make them that way. It took a system that did more for me, keeps me in range for most of my day, and has reduced the daily impact of diabetes in my life to truly understand that numbers don’t matter.
Spend enough time trawling through social media posts with a #DOC somewhere in the hashtag, and it is inevitable that you will see photos of people’s CGM graphs. Often, it’s PWD getting excited at their flat line graphs because they have managed to stay within range for a certain period of time. Or perhaps it’s to show shock and utter disbelief at loop systems doing all the work. It can be because we won’t to show how we have managed to nail the timing and amount of a bolus, and that usually-difficult to manage food nemesis (hello, rice!), completely avoiding a spike. Or, it could be just because we feel like sharing.
I don’t share my graphs a heap these days, but have in the past. It’s a personal decision as to whether we want to share their data online, and if you do, knock yourself out. Your data, your rules! I understand why some feel that it can be considered not especially helpful for others, setting us up to feel we are failing if we compare. But the conversation sharing can generate is really useful for a lot of people.
Every now and then, a non-PWD will share their libre or CGM trace to show that even those with a perfectly working pancreases are subject to glucose fluctuations. This is done with the intention of support and encouragement and to show that flat lines really are unrealistic. While I’m sure that those sharing glucose graphs of people without diabetes is never done with any malice – in fact, completely the opposite – I believe it is nonetheless problematic, and misses the point.
I get it. It’s a noble goal to try to make PWD feel less negative when we are unable to manage a perfectly flat line at 4.0mmol/l for hours on end. And to also understand that’s not how the body actually works, even when everything is doing what it should be doing.
But it is totally redundant. And downright annoying. And also, completely inconsiderate.
I live with diabetes and am fixated on trying to limit the variation of my glucose levels because I have to. PWD are told that keeping those numbers between 4mmol/l and 8 mmol/l is the goal. And we’re told that when we go outside of those numbers – especially when we go beyond the upper limit, all manner of nasty things will happen to us. That’s what was told to me the day I was diagnosed with diabetes, and repeatedly what I have seen since.
Showing me your graph that just happens without any effort on your part is not reassuring. It’s pointless. And somewhat heartless. When your level goes up to 12 because you ate a family block of chocolate, it comes back in-range fairly quickly. And not because you had to do any fancy-pants calculations, or micro (or rage) boluses.
When I eat a block of chocolate, whatever happens next is pretty much 100% due to my efforts. I have done some fancy pants calculations. I have had to bolus – maybe once, most likely a number of times – to get my glucose level back in range. And then I sit there and hope that I haven’t over bolused…
Oh – and when you show me that your glucose levels dipped into the low range or sat there for a while, it doesn’t reassure me or make me feel ‘normal’. Because the difference is that when that happens to me, I am doing all I can to make sure that I am okay, that I don’t pass out, that I don’t overtreat (again!), and that I am safe. And then I get to recover from a hypo hangover – something you are fortunate to never experience.
To be honest, I actually find it completely ironic when it is HCPs sharing their data to make me feel better, and a little thoughtless because the reason that I am in constant pursuit of these straight, tightly-in range lines is because it is HCPs that told me in the first place that is where I must stay to ‘prevent’ all.the.nasty.things.
And finally, when this happens, it centres people without diabetes in a conversation that should very much have the spotlight firmly shone on us. Your glucose level data, and the patterns they make are not like ours. They do not represent the blood, sweat and tears, the emotional turmoil, the frustration, the fear that that is somehow reflected in our data.
Perhaps rather than sharing non-PWD data, instead acknowledge just how difficult it is to do diabetes, and commend people with diabetes for showing up, day after day, to do the best we can – regardless the shape of our CGM graph.
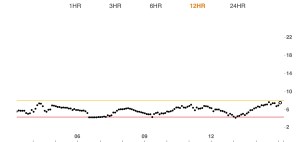
A real-life PWD CGM graph. Mine, from about 10 minutes ago.
This blog has been quiet for the last couple of weeks because, honestly, there is nothing that I had to say that was of any value. Instead, I’ve been listening, learning, talking with friends and family, crying with friends, having difficult conversations with people. And feeling uncomfortable. I’m learning to not fight that discomfort, but instead examine it and work out how I can be involved in change.
Today, I’m dipping a toe back in slowly, and sharing this from New Yorker Cartoons (maybe this blog really is going to become nothing more than an appreciation page of New Yorker Cartoons and Effin’ Birds). This cartoon spoke to me. Because: tone policing.

Recent New Yorker Cartoon by Jason Adam Katzenstein. (Click for source)
I write about being tone policed in the healthcare space, and that is what I am writing about today. It’s happened for as long as I’ve spoken up about my experiences of diabetes and my thoughts and ideas about healthcare. I’ve been called aggressive so many times by HCPs who have not liked it when a mere ‘patient’ has suggested that they are being damaging to people with diabetes in the words they are using to talk to and about us.
The bolshie nuns who taught me at secondary school taught me that when women are accused of being aggressive (or strident), it is usually because we are being assertive. I’ve come to learn that it’s not just women. It’s anyone who has, for too long, been expected to just take what is dished up – and to accept it with gratitude.
Being assertive, being aggressive, being challenging and saying enough is enough should not result in being told to tone down. Or to be excluded from discussions unless we agree to be more moderate. Or more respectful. When that respect is truly a two-way street, then let’s talk about that. But for as long as power imbalances are at play, and HCPs insist on speaking on behalf of us, or only agreeing to speak with us if they like what we are going to say; or when HPCs feature more in diabetes campaigns because they insist on centring themselves rather than actual people living with the condition…well, then we don’t have true two-way respect.
Our diabetes community is not immune from tone policing each other. It’s happened to me. I continue to listen to type 2 diabetes voices because I can never expect to understand what they are experiencing in our community unless they tell me. It may be uncomfortable for me to hear – but that discomfort comes from a place of my complicity. It is not my place to tell them to moderate the way they are speaking about their experiences, just because it makes me feel prickly. But it does happen. In the timeline of my involvement in the diabetes world, I know that when I was first diagnosed, I contributed to the stigma many people with type 2 talk about, and then, as I learnt more, I moved to being quiet about it when I saw and heard it – even though I disagreed with it. Now I am trying to be a better ally and calling it out when I see it. And shutting up and listening and accepting what people with type 2 say.
We learn when we listen. We learn when we are open to accepting that we do not have all the answers. We learn when we stop being so centred on our own experience and try to turn the spotlight onto ourselves when instead we should be shining it on others.
We learn when we don’t tell people how they should feel or how they should speak.






