
You are currently browsing the category archive for the ‘Communication’ category.
Often when we talk or read about technology it is very much about the latest, newest, shiniest devices. And yes, I wrote about those last week. There’s nothing wrong with learning about latest tech releases, or desperately wanting to get your hands on them.
But the devices are only ever half the story. And that’s why it was so great to see that in amongst all the data and the new things, was a presentation that reminded everyone watching the technology symposium at ADC that the data belongs to people and the devices are worn on the bodies of those people.
This is the whole warm hands, cool tech concept that is often missing when we hear about technology. The devices are not inanimate, they need human interaction to make them work for … well … for humans.
I despair at some of the stories we hear about technology and people with diabetes. Some talk experiences that have left them feeling like a failure when the tech has simply not been right for them. Because that is the way it is posed. If we decide the tech doesn’t suit us, hasn’t worked for us, hasn’t helped us achieve our goals, we’ve failed it.
The truth is, it’s more likely that the failure – if we need to frame it that way – is not the PWD at all. It’s more likely that the tech is not right for the person, and there wasn’t enough assistance to help navigate through to choose the right tech. Or the education was insufficient, or not tailored for the PWD, or not interesting, or not relevant (more on that soon, from Dr Bill Polonsky’s opening plenary from the conference). It is possible that the timing wasn’t right, the circumstances were not optimal, not enough conversations about cost or effort required … whatever it is, none of the blame for something not being right should be placed on the PWD.
When we look at diabetes education, or engagement with healthcare professionals, the stories that are celebrations or considered successes (from the perspective of the PWD and, hopefully, the HCP) show the right recipe. The ingredients will all be different, but the method seems to be the same: the person with diabetes is listened too, time is taken to understand what is important for them, the PWD’s priorities are clear, and goals are realistic and checked along the way. The end results are not necessarily based on numbers or data points, but rather, just how well the person with diabetes is feeling about their diabetes, and if anything new has added to their daily burden. Reviews are focused on successes more than anything else.
My favourite ever diabetes educator, Cheryl Steele, gave an outstanding presentation on how HCPs can best work with people with diabetes to ensure we get the most from our technology.
I spoke with Cheryl after her talk (you can watch the video of our chat for Diabetes Australia at the end of today’s post), and she laughingly said that she could have said the most important things she wanted to say in 2 minutes, and with one slide that basically just said that HCPs need to be truly person-centred and listen to PWD.
But thankfully, she spoke a lot more than that and covered a number of different topics. But the thing that got to me – and the thing that I hope the predominantly HCP audience would take home and remember – was Chery urging her colleagues to focus on the positives.
Cheryl said, ‘The emphasis has to be on what you’re doing well’ and I feel that is a wonderful place to start and end healthcare consultations. I think about experiences where that has happened to me. Such as the time I went to my ophthalmologist after a few years of missing appointments and his reaction to seeing me was not to tell me off for not showing up previously, but instead to welcome me and say it was great I was there. I’ve never missed an appointment since.

How many PWD reading this have stories to share of times when they went into an appointment with data and all that was focused on was the out-of-range numbers? There are countless stories in online diabetes groups where HCPs have concentrated on the 10% out of range numbers rather than the 90% in range. Actually, even if only 10% of numbers were in range, that is 10% that are bang where they need to be!
Perhaps that’s what’s missing from diabetes appointments. Gold stars and elephant stamps!
There is something devastating about walking into an appointment and the first, and sometimes only, thing that is on the HCPs radar is numbers that are below or above the PWD’s target glucose range. I’ve sat in those appointments. I know the feeling of walking in and feeling that I’m tracking okay, only to have none of the hard work I’ve managed acknowledged and instead, only the difficulties addressed.
But then, I think about one of the first experiences with the endocrinologist I have been seeing for twenty years. Without judgement, she acknowledged that I wasn’t checking my glucose much, and asked if I felt that I could start to do one check every Wednesday morning when I woke up. I said that it seemed like such a pathetic goal to set, but she gently said, ‘One is more than none’. The focus was not on what I wasn’t achieving. It was on what I could.
What a wonderful motivator that is.
Disclosures
Thanks to the Australian Diabetes Society and Australian Diabetes Educators Association, organisers of the Australasian Diabetes Congress for complimentary registration to attend the conference. This gave me access to all the sessions.
I work for Diabetes Australia and the video shared is part of the organisations Facebook Live series. I am sharing here because is relevant to this post, not because I have been asked to.
As usual, no one has reviewed this piece before I hit publish (which is unfortunate because I could really do with an editor).
A week out from National Diabetes Week, and this piece has been sitting in my ‘to be published’ folder, just waiting. But the post-NDW exhaustion coupled with lockdown exhaustion, plus wanting to make sure that all my thoughts are lined up have meant that I haven’t hit the go button.
In the lead up to NDW I wrote this piece for the Diabetes Australia website. That piece was a mea culpa, acknowledging my own contribution to diabetes-related stigma and owning it. I also stand by my thoughts that the stigma from within the community is very real and does happen.
But what I didn’t address is just where that stigma comes from. Those biases that many people with type 1 diabetes (and those directly affected by it) have towards type 2 diabetes come from somewhere, and in a lot of cases that is the same place where the general community’s bias about diabetes comes from. It is all very well for us to expect people with type 1 diabetes to do better, but I’m not sure that is necessarily fair. I think that we should have the same expectations of everyone when it comes to stamping out stigma.
And so, to the source of stigma and, as I’ve said before, it comes from lots of places. As someone who has spent the last twenty years working in diabetes organisations, I know that the messaging my orgs like (and including) those that have paid my weekly salary has been problematic. I still am haunted by the ‘scary’ campaign from a few years ago that involved spiders, clowns, and sharks. (If you don’t remember that campaign, good. If you do, therapy works.)
For me personally, I don’t think much stigma I have faced has come at the hands of other PWD. Sure, there’s the low carb nutters who seem to have featured far too frequently on my stigma radar, however, the most common source of stigma has undoubtedly been HCPs.
It’s not just me who has had this experience. The majority of what I have seen online as a response to experiences about stigma involves heartbreaking tales of PWDs’ encounters with their HCPs.
While I will call out nastiness at every corner, and no stigma is good stigma, it must be said that there is a particular harm that comes when the origin of the stigma is the very people charged to help us. Walking into a health professional appointment feeling overwhelmed, scared, and frustrated only to leave still feeling those things, but with added judgement, shame and guilt is detrimental to any endeavours to live well with diabetes. In fact, the most likely outcome of repeated, or even singular, experiences like that is to simply not go back. And who could criticise that reaction, really? Why would anyone continually put themselves in a situation where they feel that way? I wouldn’t. I know that because I didn’t.
It’s one thing to see a crappy joke from a comedian who thinks they’re being brilliantly original (they never are) or the mundane, and almost expected, ‘diabetes on a plate’ throwaway line in a cooking show, but while these incidents can be damaging, they are very different to having stigmatising comments and behaviours directed at an individual as is often the case when it is from a HCP.
Of course, HCPs aren’t immune to the bias that forms negative ideas and opinions about diabetes. In the same way that people with type 1 diabetes form these biases because those misconceptions are prevalent in the community, HCPs see them too. Remember this slide that I shared from a conference presentation?
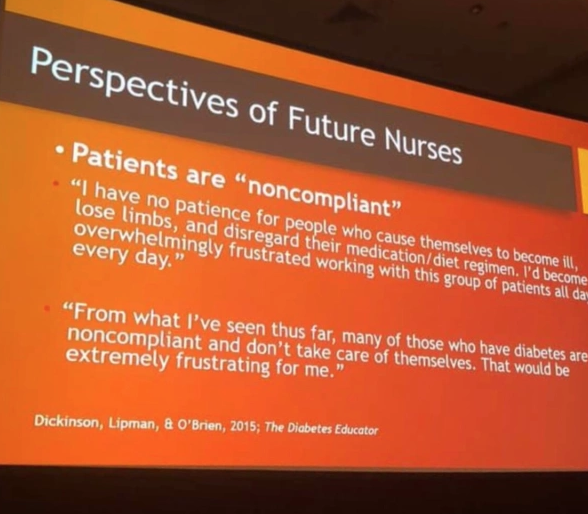
This came from student nurses. Just think about that. Students who were training to be HCPs who would inevitably be working with people with diabetes. A I wrote at the time:
‘They hadn’t even set foot on the wards yet as qualified HCPs. But somehow, their perceptions of people with diabetes were already negative, and so full of bias. Already, they have a seed planted that is going to grow into a huge tree of blaming and shaming. And the people they are trusted to help will be made to feel at fault and as though they deserve whatever comes their way.’
Is it any wonder that, with these attitudes seemingly welded on, that people with diabetes are experience stigma at the hands of their HCPs?
The impetus can’t only be on PWD to call this out. And the calls to fix stigma can’t exclusively rest on the shoulders of PWD – we already have a lot of weight there! It must come from HCPs as well – especially as there is such a problem with this group. Perhaps the first step is to see real acknowledgement from this group of their role here – a mea culpa from professional bodies and individuals alike. Recognising that no one is immune to the bias is a good step. Owning that bias is another. And then doing something about it – something meaningful – is how we make things better for people with diabetes. I really hope we see that happening.
More about this:
Becoming an ally – how HCPs can show they’re really on our side.
As someone who spends far too much time sharing far too many things across far too many online platforms, this Hartley Lin cartoon for the New Yorker hits far too close to home. (But it made me laugh all the same.)

Today I’m talking menopause, because for fuck’s sake, why don’t we do that more?
Actually, I know why. It’s because it’s considered an exclusively ‘women’s issue’ and has been the butt of jokes from male comedians and talk show hosts, and really, who gives a fuck anyway?
This post is likely to continue being sweary, because as I’ve tried to find information on diabetes and menopause it seems that the road is similar to pretty much any other issue about diabetes and women’s health. Sure, there’s quite a bit out there about pregnancy – and you bet I take some credit for that because back in 2001 when I started working in diabetes organisations the very idea of lived experience-led information about diabetes and pregnancy was not typical at all, but we wrote a resource and it is still (in a very updated format) still available) – but it’s up there with trying to find details about women with diabetes and sexual function and sexual health.
I am literally counting down the days until Dr Jen Gunter’s new book, The Menopause Manifesto, makes its way to our bookshelves, because I know it is going to be an absolute wealth of no-bullshit, evidence-based, straight-talking information. Her previous book, The Vagina Bible, (known in our house as ‘The Vible’) delivered that in spades as it busted myths, is easy to read and matter of fact, and suggested just where Gwyneth Paltrow might like to shove her $300 jade eggs (spoiler: not up her, or anyone else’s vagina). I was so pleased that when she mentioned diabetes a few times in her book, the information was spot on. In fact, I think that her explanation as to why women with diabetes may experience yeast infections more commonly was one of the clearest I’ve ever read.
Now, Jen Gunter has turned her full attention to the issue of menopause. This great piece is an excerpt from the book (due out at the end of the month and available for pre-order now), and the part that stood out for me was the bit where she said that often, menopause gets blamed for everything any time a ‘woman of a certain age’ has symptoms they take to their HCP.
Sounds a little familiar, doesn’t it? I guess I’ll have to add ‘Sometimes it’s not menopause’ to my lexicon, right there alongside ‘Sometimes it’s not diabetes’. How easy, and convenient, it is to simply dismiss someone’s concerns simply because there is something easy (and perhaps obvious) to blame it on.
Of course, with diabetes and menopause, there is the bit I have learnt where some of the symptoms of aspects of menopause look very much like the symptoms of aspects of diabetes. Looking into patenting a game called Hypo or Hot Flush in the coming years. I think it might be popular with PWD of a certain age. The winner gets a cold compress and a jar of jellybeans.
Here’s the thing. I’m not actually menopausal. I don’t even know that I’m necessarily peri-menopausal yet. But in the same way that I wanted to know all there was about diabetes and pregnancy before I was ready to get pregnant, I’m trying to prepare myself as much as possible for the somewhat mythical period of menopause. Forewarned is forearmed or whatever that saying is. The problem with that is that there is so little info out there that arming myself is proving a little difficult. And it appears that I am not alone in my thinking.
In much the same way as speaking about sexual health when I’ve found myself in a room with a few of my female diabetes friends (and wine), it seems that once we hit our mid-40s we start wanting to talk about menopause as well, searching out any titbits of information that may just help us know what we need to get ready for. We’re desperate for tips and tricks and a glimpse into what we have in store. And it seems that very few of us is having these conversations with our healthcare professionals.
Lucky for me, my endo has spoken with me about it a little – after I’ve asked. She tells me that the mean age of the start of menopause is 47 years, which is smack bang my age, so I’m expecting to have some firsthand experience soon. And when it comes to sharing that experience, I am already committed to writing about it in a way that moves from the focus on loss that seems pervasive in most of what I’ve read about it – the loss of fertility, the loss of libido, the loss of vitality. #LanguageMatters in menopause too, and the idea that we are writing off those going through it when it’s possible they still have half their life ahead of them sounds a little grim.
So, my question is, what do people with diabetes need to advance discussions around this? What do we want to know? And when and how to we want that information? Is it a matter of just starting to talk about it more in public forums? Do we routinely start asking our HCPs for information so that slowly (because everything in healthcare takes time) it is on their radar? Do we need more research? (Yes, the answer to that is a resounding yes.) Do we need a snappy hashtag? Is that hashtag #HypoOrHotFlush? (No, I think not.)
If you’d like to join the conversation, please respond to this tweet. Or to this post. Or send me a message privately. And I’ll follow up with another post in a few weeks.
Looking for more?
Great post here by DOC legend, Anne Cooper.
Sarah Gatward has written a terrific series of her experiences of menopause on her blog here.

I want to acknowledge that not only women experience menopause. Thanks to this brilliant website, Queer/LGBTQIA+ Menopause, that I kept referencing today, which provides fantastic advice for how to speak about menopause to capture the experience of people who are not cisgender and/or not heterosexual.
Back when I first started writing and talking about diabetes language matters, it didn’t seem to be all that contentious an issue. I had been following with great interest how this discussion played out among people with diabetes, and it was super clear to me back then that there wasn’t a one size fits all approach or way of thinking. Some people were interested, some couldn’t have cared less. It was accepted that there would be different opinions and attitudes with different people. I know, how completely unexpected, because in every other way, people with diabetes are a tidy, identical, homogenous group who agree on EVERYTHING! #SarcasticFont
Many, many, many years down the track, more and more people are buying into this topic of conversation, which leads me to think that language does, in many ways, matter. To lots of folks.
Which is why it’s frustrating – and problematic – how fixated this discussion can become on specific words. That, I believe, is the problem with #LanguageMatters.
When I think about why I became so interested in this issue, I’m really clear why it mattered to me. It wasn’t about manners. It certainly wasn’t about suggesting that people with diabetes (that’s my preferred terminology, but you do you!) be told how to speak about the health condition we own.
To me, it never was about individual words. It was about words, broadly. It was about images used to accompany diabetes discussions. It was about attitudes. It was about behaviour. It was about addressing the image problem that diabetes (still) has. It was about changing the mindset that it’s okay to use diabetes and those of us living with it as a punchline. It was about shifting the public perception about diabetes. It was about people with diabetes not feeling ashamed to do their diabetes tasks in public. It was about elevating our health condition to the same level as other health conditions. It was about people with diabetes being respected. It was about stopping blame and shame and stigma. It was about people with diabetes deciding and directing how their own brand of diabetes would be discussed by those around them.
It was always about communication as a whole – communicating to and about people with diabetes.
And yet, with all that in mind, so many online discussions that I see still want to reduce this big body of work to: ‘But I want to call myself a diabetic.’ If someone said that to me, which some people certainly have, my response has been, ‘Okay, cool. You should definitely do that then!’
So why does THIS seem to be the particular tiny, infinitesimal, microscopic, miniscule part of the whole language discussion that some people keep coming back to?
I’ve started to wonder what are their motives behind focusing on this issue? When I see someone, especially someone who’s been around for a couple of years and who everyone knows has been part of these discussions before, start with the PWD vs diabetic debate, I wonder if they’re trolling. They know it will get a response. They know it’s likely there will be disagreements. There are some super savvy people on social media out there who know that asking this question, or even just mentioning it will get a reaction – every single time – and it might even add to their follower count. I guess that some people think that’s currency.
But really, all it seems to do is narrow and diminish the broader discussion. These days, when I am asked to give a talk on language and diabetes, I dedicate one slide and about 45 seconds at the beginning of my talk to get the diabetic / PWD issue over and done with, and then focusing on what I want people listening to the presentation to take away with them.
I don’t know how or when the diabetes #LanguageMatters hashtag started. It wasn’t the name of the first language position statement, but it certainly has been used for a very long time, and been associated with the global movement that has its foundations very firmly rooted in the diabetes community – even before the advent of the DOC, because this discussion has been happening for long before our community moved into online spaces.
The problem with using #LanguageMatters is that it is too often drawn into being about one tiny part of the whole big issue. But it seems that #LanguageMatters is here to stay with a whole lot of material and dialogue and debate behind it – a lot of which is making a huge difference to the way people feel about their own diabetes. So, what a shame that it so often gets minimised to something that is only one little part of it. What a shame that some people knowingly fuel the fire and the arguments that ensue by bringing up diabetic/PWD again. What a shame that this really important, really BIG issue is reduced to something quite tedious.
Perhaps we should have gone with #CommunicationMatters to signpost that it wasn’t about specific words. Perhaps we should have gone with #AttitudesMatter to bring in how language adds to attitudes of stigma and blame Perhaps #BehavioursMatters would have addressed how body language and other behaviours can be just as important as verbal language.
Or perhaps we should have used all of them because, really, #ItAllMatters.

You can read read more on my frustration about this issue in this post (and frequently on my Twitter feed).
Last night, I had the honour of speaking at the World Health Organisation Informal Consultation on Diabetes, which is currently taking place as a virtual event. It’s a three night/three day (depending on where you are in the world) event that has brought together people living with diabetes from all corners of the world.
This was a widely advertised event, and anyone could apply. The expression of interest call out was all over Twitter, Facebook and diabetes community groups. Unlike some other initiatives and programs, PWD didn’t need to be nominated by a diabetes organisation or HCP to be part of it. You just needed to fill out the application form (which didn’t take too long), and submit. Clearly a lot of people with diabetes saw it and thought it was something they wanted to be involved in! I’m not sure of the overall numbers, but there is certainly terrific representation from a number of communities.
On my Zoom screen I could see a combination of familiar faces, faces of people I know of but have never met or engaged with, and a whole lot of new faces. Hearing their stories, and reading the discussions that are filling up the chat box are enlightening. And reassuring. Because once again I was struck by how strong, vulnerable, admirable and strong-willed others treading the diabetes path can be. There are striking similarities and glaring differences. But common threads that run through the narratives we heard And mostly? There is support and gratitude to be there and to bear witness to others sharing their stories, ask questions and learn. Not a single snipy comment or passive aggressive remark – not because we all agree or are a homogenous group. But rather because we respect and value and admire the people who have the courage to stand up and be present.

I was invited to speak in a session about diabetes advocacy. The session’s title was ‘Strategic communication in global diabetes advocacy’, and it included Christel Marchand Arpigliano from Beyond Type 1 and Lauren Carters-White, a research fellow from the University of Edinburgh. Christel spoke about how when we tell our diabetes stories, we are translating the language PWD use – language that makes sense to us – into words that reach a broader audience.
Lauren used some terrific examples from around the world to show the impact data and evidence can have in advocacy efforts.
And I rounded out the session by talking about how when we bring the two together, we win the hearts and minds of the people we are trying to influence – decision makers, legislators, policy makers, educators, healthcare professionals and researchers. Because when we have the emotional pull of how diabetes impacts on daily life, combined with the evidence to show what that means, we can’t be ignored! I highlighted how working with healthcare professionals and researchers to further our messages means that our lived experience can’t be dismissed.
I also spoke about how the power of stories is magnified when there are many voices and many different narratives. I have rarely, if ever, heard someone share their diabetes with the pronouncement that they speak for all with diabetes, or that their story is THE story. But they are all experts in their own lived experience and that certainly should be celebrated. And its power should not be underestimated.
I think the thing I have felt most strongly in that Zoom room is the camaraderie and solidarity – again, not because we are all on the same page and all want the same things. But rather, everyone truly supporting each other and bringing others into the conversation has been an overarching quality of the meeting. No one dominates; no one is more important than anyone else; no one claims to be THE advocate. We are all advocates working together, and supporting each other for a bigger cause.
Of course, we want, and expect, to see action come from the three days of meetings and workshops, and I have confidence that will happen. But in the meantime, to have such large group of dynamic people come together whose only agenda is community and to build each other up, rather than tear each other down, reminds me that THIS is what diabetes advocates can do and what the community is mostly about. Those snippy voices who try to minimise people who are truly trying to improve outcomes for people with diabetes aren’t present. Because what a waste of time that would be!
I may have spoken about, and given tips about how to win others’ hearts and minds in my talk, but it’s my own heart and my own mind that have been won over by my peers in this event.
(You can follow along the discussion by using the hashtag: #WHOPLWDs)
Disclosures
None. I am not being paid to attend this event, and have not received payment, honoraria or in kind donations for my presentation, and am attending in my own time. I might need a nap later today though, because the 11pm-3.30am time for Aussies on the east coast is tough going!
Apparently, diabetes blogs are dead. At least, that’s the proclamation that seems to made every month or so. You should very much consider my bias when I say that I don’t agree with that sentiment at all. I mean, I have a shitload of content on this here site – including new and re-visited posts that for me have some relevance to my diabetes life in the moment.
Newer and shinier platforms are here now, so surely that means it’s time to retire WordPress and Blogger. Or is it? Newer and shinier platforms are great, so I’m not here to claim that that they’re a waste of time. Podcasts and vlogs are great tools for sharing diabetes information. YouTube and Reddit are great places to learn. And then there is Tik Tok, but I am too old to be allowed to even log into that platform. (Not true, and I have loved some of what’s been shared there. It can be a brilliant storytelling and info-sharing format!)
I’m here to say that every single platform for sharing a diabetes tale has its place. And blogs are still very relevant: the long-form post is not dead. Not yet anyway.
It is from blogs that I learnt, and continue to learn from others with diabetes. I revisit old posts I’ve read because they remain relevant today, and have many bookmarked and saved because the information shared is so spot on! I use them as research for pieces I’m writing and presentations I’m giving. I send links to old (and new) blog posts to others with diabetes when they ask questions that I know someone has answered so beautifully. And I send posts to HCPs to give them an insight into real life diabetes that they may otherwise have not understood – a glimpse into the things we are hesitant to share with them – and how our interactions with them can leave a lasting impression: both good and bad.
Blogs are also where we hear from those who are adjacent to actually living with diabetes. Reading posts from parents of kids with diabetes and partners of loved ones gives me a perspective that I simply don’t have firsthand.
Advocacy and awareness efforts have been described and fought through blog posts. I’ve used this blog to advocate increased funding for products, research and healthcare. It helps get the message out to people, with simple calls to action so they can get involved too. And the first time I ever heard about Spare a Rose was via this post (the links in the post are not current), and from there so many in the diabetes blogosphere – myself included – jumped on the bandwagon to support this important campaign. We knew that while donating was important, getting the word out was critical too. Since 2013, dozens and dozens of posts have been shared, raising awareness about how this ‘by the community, for the community’ grassroots initiative.
Blogs are where some of those deep and scary issues that we only whisper about or hide away are discussed. It was in blog posts that I first read about just how diabetes impacts on mental health. Experiences about diabetes-related eating disorders were shared without judgement and shame. It was through my writing about infertility and diabetes that I connected with so many other people going through the same thing.
Diabetes blog posts – old and new – are a patchwork quilt of lived experience gold, with the common thread that no one’s diabetes story is more valuable or important, but that everyone has a story to share that is worthwhile.
Some believe that blogs posts are just a way for people to ramble and navel gaze and seek attention. Well to them, I say please enjoy (or don’t) exhibit A – the 1100+ posts here that may be navel gazing to some, but paint a picture of my 22 years of diabetes. It’s not everyone’s experience; it’s not everyone’s cup of tea. And I’m okay with that! If you don’t like the blog format, move on. No one is forcing anyone to read a blog post. Or to get on any other format for that matter. Because, of course, your preferred diabetes info mode may vary (#YPDIMMV).
Someone said to me that reading new blog posts these days is boring because there is nothing new – it’s already been said. And you know what? That could well be true. Diabetes is boring and even though everyone’s diabetes is different, many of us write about similar situations. But actually, that’’s okay. Because for some people, it may be the first time they see or read a post about a particular topic – even if there are five million others! – or perhaps there is a different outlook in there.
I think that people write for different reasons. I write for a creative outlet and writing provides me with a way to explore different ideas about not only my own diabetes, but the diabetes landscape. But mostly, I write to connect with others. I don’t think anything I have to say is particularly erudite or mind blowing. I don’t have any revelations that will help someone else’s diabetes make sense. My own diabetes makes no sense to me, so the chance of it making sense to someone else is very unlikely.
I found most diabetes blogs because their writer shared them on Twitter or on Facebook. Or, others in the community shared them, which is one of the truly wonderful things about the DOC – the way some people elevate others in the community. There used to be an annual event called #DBlogWeek which was a brilliant opportunity to learn about others writing about diabetes. Diabetes Mine’s monthly blogosphere wrap up keeps me updated with some wonderful pieces. (And for German speakers, here you can find a curated collection of blog posts by Bastian from deDOC : I run posts through Google translate to understand them.)
And so, here are some of the brilliant pieces written by PWD I’ve read in recent times. I hope that you enjoy them too.
Corinna Cornejo writes at Type 2 Musings, and is also a contributor to the Ascensia Editorial Board (disclosure: I am too and am paid for my contributions). This great piece about power imbalance in the clinic room.
One of my favourite Aussie bloggers, Frank Sita, wrote this insightful piece about taking a pump break over the festive season:
Diabetes and pregnancy and baby blogs have always been a favourite of mine. I cannot tell you how many I read back when I was at that stage of my life! New mamma Ashley has shared this gorgeous post while (literally) awaiting the arrival of her baby girl.
I loved Dave Sowerby’s 2020 look back in this post.
Kerri Sparling may have retired her blog a couple of years ago, but I was so grateful for this new post on September last year while Melbourne was in the depths of lockdown. I’m sharing it here for others who are locked down at the moment. (And Kerri’s fourteen years of posts are still available at SixUntilMe.com)
Tim Street’s blogs are not for the faint hearted! They are often super technical, but non-techies (my hand is raised) will definitely get a heap out of them. His latest blog post from just a couple of days ago has me thinking about what I need to do to jiggle my basal rates a bit.
I haven’t watched the video that accompanies this blog post from Jen Grieves, but the words expressing how she is feeling in the midst of lockdown resonated so beautifully.
Holly Allen’s post from the end of 2020 about imposter syndrome hit a little too close to for comfort! It’s a recurring theme from some diabetes advocates (and my hand is raised for this one too!)
This from Molly at Hugging the Cactus had me aching as I read it. I miss my diabetes mates so hard and mourn all the opportunities we’ve missed to catch up.
And finally, I’ve not been able to stop thinking about this piece from Cherise Shockley that she wrote for diaTribe recently, and the idea of a carb glass ceiling. I realise that I have a very similar way of thinking when it comes to counting carbs and I love how she has explored the psychology behind why people may think this way.

Diabetes Awareness Month has come to a close and with it the blue that has washed over my social media feeds will dim a little. I had a quiet month, spending most of my time following others rather than sharing my own content. It seems to have been representative of my year in diabetes advocacy, really.
I’ve been quiet. It wasn’t planned, but it has been deliberate. And it hasn’t gone unnoticed. I’ve started and stopped and started and stopped this post for a while to answer the messages from people who have so kindly asked if I am okay. Let’s see if this is the one that sticks…
Earlier this year, I wrote about having a panic attack while on a plane after landing back in Melbourne from ATTD in Madrid. You can sort of read about it here, although I was pretty vague about what actually happened saying little more than that I turned on my phone to a million Twitter notifications about a blog post that some people had assumed was written about me and then subsequent comments. I was surprised, horrified and more than a little confused.
This came hot on the heels of a couple of other tricky situations. There was the run in with the diabetes HCP who told me to tone down (after they completely misrepresented what I had written about). And then there was another HCP rallying troops to call me out (that caused me to lock my twitter for the first time ever at the end of last year).
Anyway…the culmination of all these things resulted in the realisation that this year was going to be a lot different for me. I was going to take a massive step back from much of the work I did that was public facing. I felt that I simply couldn’t take the scrutiny that was coming my way.
Even before the panic attack on the plane incident, I was feeling unsettled. I was unspeakably nervous about the presentation I had been invited to give at the conference in Madrid. This was a completely alien feeling to me. I have been speaking publicly for decades, and for twenty years, comfortably stood on stage playing the flute for anyone who would listen. Standing in front of an audience doesn’t make me nervous. It doesn’t make me sweaty and scared. And yet, here I was wondering whether I should not go to Madrid at all to stand up on that stage. But after some ridiculous bravado as seen in this post, I decided that I had to go.
As I sat on that plane, desperately trying to recover from the panic attack that was making it difficult for me to breathe and hiding my tears from the other passengers, I had a fleeting thought that I probably should have gone with my gut feeling and stayed home!
And so, I felt that there was only one thing I could do. Forget the whole stand up thing and instead step back. I wasn’t necessarily sure what that would look like. I couldn’t stop attending and being part of diabetes meetings and conferences because that is part of my job, but I could turn down speaking engagements or anything that put me in a position where I was sharing my personal, lived experience that others might find challenging, or at odds with their own. I needed to deal with the diabetes burnout that was so, so heavy and weighing me down.
COVID-19 certainly helped with that. As the world got turned upside down, a lot of the things that I was worried about simply didn’t happen. It became easier for me to limit my interactions with people and hide away a bit more.
The feelings of burnout and anxiety about being part of the community didn’t disappear, but they seemed less urgent.
And with that came the realisation that the burnout I was feeling because of diabetes actually was not because of my diabetes at all.
Diabetes burnout has always happened to me when those constant diabetes tasks became too overwhelming; when just the thought of opening up a meter bag, or checking my CGM trace was too much to even contemplate. Burnout meant that every single number became a measure of my value and worth. I’d lose all perspective and lose all confidence of my abilities to actually do what I needed to do.
The burnout I felt now was the effort of being a diabetes advocate IN the diabetes community. It was fearing that I was being seen in ways that actually were completely inaccurate – in fact at complete odds with everything I have ever stood for – and that led me to second guess everything I said, fearing that I would be misunderstood. It was feeling vulnerable and scared and exposed in the community that was meant to support me.
I received an email from someone in the DOC who has been around for many years, and I have known (on Twitter only) who told me that because I am confident in my communication, am comfortable challenging ideas different to mine and share opinions that not everyone agrees with it, I leave myself open to criticism. And that criticism and the dialogue that follows resulted in their corner of the diabetes community being less enjoyable to him and others. All while suggesting that, unlike he, who has never deliberately set out to disagree with anyone – I seem to revel in it.
Interesting take. I don’t seek to disagree with people. But if anyone is saying something that I believe is stigmatising to PWD or minimising our experiences, I will call it out. It’s been my MO for almost twenty years.
I never replied to the person who sent me that email. I cried about it for days, however, and have it filed away and occasionally return to the half-written response that I keep meaning to finish so I can hit send on my reply. I feel it’s quite impolite that I’ve not replied to someone who took the time to write to me… But, truthfully, I am too tired, and that so-called confidence has abandoned me.
Diabetogenic is the least active it’s been since I started it close to ten years ago. That’s not because I have nothing more to write – I still write every single day, I just squirrel things away now, too afraid to share them, sticking to safer topics – research call outs, fundraising initiatives, commenting on things that aren’t controversial or taboo topics.
I started this blog because it was the space for me connect with others – not only people who were walking the same diabetes path as me, but also those who were doing things very differently. Because often, they are the people I learn most from.
It became a place I could write about those issues that were tough – the mental health challenges of diabetes, the frustrations and desperation I felt about the health system, trying to navigate through health professionals who refused to acknowledge that PWD belong everywhere and anywhere diabetes is spoken about. And it was a place that my split-apart heart was able to open up and share the unspeakable sadness that I felt as fertility issues became part of my life. I am so grateful that I was able to do that and receive the support that I so desperately needed from people who understood how the impact of diabetes on those fragile, and so, so hard parts of life shattered me into a million broken pieces. Because it was those people who helped glue me back together.
Wanting and needing that support and connection hasn’t stopped. I still seek it. I’m just a little more cautious about how I go about it these days sticking with friends and others I feel safe with rather than the wider community that doesn’t feel safe. I know where to go to get what I need.
I don’t really know what to do with this blog anymore. Feeling unable to share a lot of what I want to say is alien to me. But for now, this doesn’t seem to be the place to do it. I guess I continue as I have been – hitting publish when I feel I can, and for the next month, anyone popping by will see a lot of pleas to donate to Insulin for Life.
And I guess that will have to be enough for now.







