
You are currently browsing the category archive for the ‘Awareness’ category.
I’m heading to Sydney this morning (it’s early…too early) for the Australasian Diabetes Advancements and Technologies Summit – ADATS, (follow along at #ADATS2018), which had me thinking about the conference last year where I spoke about Loop, scared a shitload of HCPs, was almost traumatised into never speaking again in public (almost – didn’t happen) and was happy to be branded non-compliant.
Today will be a far gentler experience – my role is as a member of the organising committee, and as a session chair. Surely no one will want to sue me for that. Right?
As I ponder that, and reminisce about last year’s talk, here are some links. So many links that I have been wanting to share. So, have a cuppa, have a read, and share stuff.
Also, being deliberately non-compliant is kind of fun…

(Disclosure first: My flights from Melbourne to Sydney are being covered by the National Association of Diabetes Centres (NADC), the organisers of ADATS. I am on the organising committee for the conference.)
_________________________________________
Finally DIYAPS makes it to the mainstream media in Aus
I’d heard of The Saturday Paper, (which was a surprise to the journalist who interviewed me), but apparently not all that many people have. It’s a weekly newspaper (somewhat unimaginatively named – it’s a paper and comes out each Saturday) with long-form articles. One of those articles was about DIYAPS and came about after journalist Michele Tyde heard about the Diabetes Australia DIYAPS Position Statement.

Read the DIYAPS Position Statement here.
The body part is connected to the PWD
‘Talking about the “diabetic foot,” the “diabetic kidney,” or the “diabetic eye” suggests they are somehow separate from the person whose body actually hosts the diabetes. This language suggests the diabetes-complicated body part is more like a malfunctioning car part that needs service – if only we could be provided with a courtesy foot, eye, or kidney to use until our own is better!’
The language at ADA this year (all the way back in June…all the way over in Orlando) didn’t really set off too many alarm bells. Until we had a good look at the program. I wrote this piece with The Grumpy Pumper for diaTribe about how it seems that #LanguageMatters a whole load less when talking about diabetes-related complications…and that needs to change.
Conference blogs
It’s great to see the Ascensia Diabetes Care team continue to support diabetes bloggers by inviting them to write up their thoughts on diabetes conferences. The latest contribution is from Sascha Stiefeling (who blogs at Sugar Tweaks) where he gives some insights into the start of EASD. (It was written in German and translated into English.)
Oh – and here’s the post I wrote for them about the Australasian Diabetes Congress a couple of months ago. (I was not paid to write this, or supported by Ascensia to attend, but I did work with them on their Social Media Summit.)

No weakness at all
On Mental Health Awareness Day this year, UK writer and poet David Gilbert wrote this beautiful post about the strength – not weakness – of living with mental illness.
How we are wrong about obesity
This piece about obesity is a must read. It talks about how weight bias from healthcare professionals and stigma often results in higher weight people avoiding going to the doctor because they fear discrimination, not being believed and being shamed.
More on weight stigma
And read this piece (also on diaTribe) about how weight stigma hurts people and affects health outcomes.
Keep Sight
This week, Diabetes Australia officially launched the first ever national eye screening program, Keep Sight. The program will make it easier for Aussies with diabetes to get their eyes checked. You can read about the program here (from when it was announced back in July).
Disclosure: I work at Diabetes Australia, but was not asked to write about this program. I’m doing so because it is important.

Your story is important
True champion of listening to ‘the patient’, Marie Ennis-O’Connor wrote this wonderful piece about the power of storytelling in healthcare.
Always be kind
I’m always fascinated to read stories from HCPs who write about their experiences on the other side of healthcare. Moving from care-giver to the one needing care can be life-changing. In this BMJ Opinion piece, health researcher Maria Kristiansen writes about how important compassion and kindness from healthcare professionals were for her and her family during her young son’s illness and death.
More on kindness (because we can never have enough)
The first sentence of this article in BMJ by Dr John Launer had me hooked: ‘I’m not a clever doctor, but I’m a kind one’. Have a read.
Diabetes in hospital
I know I’m not the only one to be terrified of needing to go into hospital, worrying about a lack of knowledge about type 1 diabetes treatment and my technology, and having to fight to maintain ownership of my own diabetes care. Adam Brown at diaTribe has written about his recent trip to A&E, surgery and subsequent recovery after his appendix ruptured. Lots of great tips for anyone who may wind up in hospital.
Digital diabetes
How can digital medicine and research, and artificial intelligence transform diabetes? That’s the question research scientist in diabetes, Dr Guy Fagherazzi, asks in his (open source) review in Science Direct that you can read here.
Bake these!
And finally…It’s nearly the weekend and if you have a spare 20 minutes, you really, really should think about baking these! They are crackled parcels of molasses, spice and all things nice and are, quite possibly, one of the best things I’ve ever baked.

After a wonderful couple of weeks of real holidays – sun in Italy, less sun in London – I headed to Berlin, saying good bye to my family as we headed in different directions. I was bound for meetings before EASD officially kicked off. And they were headed to Wales and canal boats with extended family. We could not have found ourselves in more different settings!
My first day in Berlin was dedicated to HypoRESOLVE, the Innovative Medicines Initiative (IMI) funded project looking to provide a better understanding of hypoglycaemia. I am on the Patient Advisory Committee (PAC) for this project, which kicked off back in May this year in Copenhagen.
The project is divided into eight work packages (WP) and it was WP 8 that convened the first meeting. I was there as part of the PAC, and also to provide the personal perspective on hypoglycaemia.
Back in May at the kick off meeting, I had given a talk called ‘The literal lows of my diabetes’, where I spoke about my own experiences of 20 years of diabetes and how hypoglycaemia had impacted on my everyday life. This was a very personal talk, where I spoke about the fear and anxieties of lows, my different hypo personalities and the terror that comes with impaired hypo awareness.
But for this new talk, I wanted to do something different. I didn’t want to highlight my own experiences, because I am but one person and it is important that the audience never feel that they have ‘done diabetes’ and understand the ‘patient view’ because they have listened to one person.
I wanted my focus to be on the disconnect between how hypoglycaemia is regarded in the clinical and research world as compared with the real-living-with-diabetes world.
So, I used the tools at hand, and the fact that there is a vocal and ready to help diabetes online community just a few clicks away and sent out this tweet:

It was apparent straight away, as the responses came flooding in, that the way hypos are described and classified in clinical and research terms is very, very different to the way those of actually experiencing lows see them.
Here is how hypos are categorised in the literature:
 Straight forward, neat, tidy, pigeon-holed.
Straight forward, neat, tidy, pigeon-holed.
And yet, when I asked PWD how they would describe hypos, here is what they came up with:
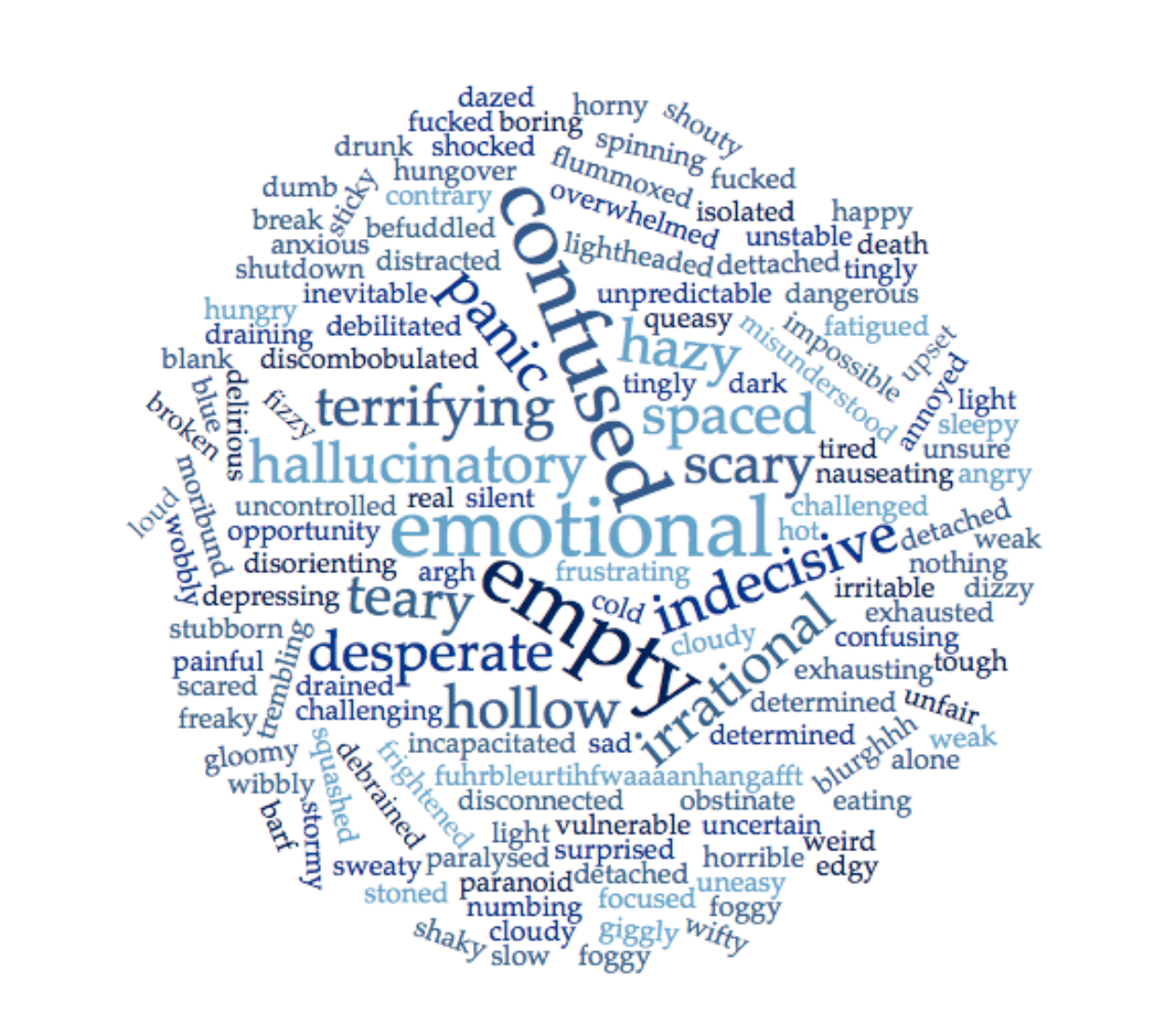
Some of the words were repeated multiple times, others appeared only once. Some of the words are the words I use to describe my own hypos, many I had not considered. Yet every single word made sense to me.
Hypoglycaemia, in the same way as diabetes, is not neat and tidy and it cannot be pigeon holed. I hope that my talk was able to illustrate that point.
And I hope I was able to highlight that using simple words and simple categorisations only service to limit and minimise just how significant and impactful hypoglycaemia truly is for those of us affected by diabetes.
You can keep an eye on the progress of HypoRESOLVE on Twitter, and via the website.
DISCLOSURE
The HypoRESOLVE project funded my travel from London to Berlin and provided me with one night’s accommodation. I am not receiving any payment for my involvement in the Patient Advisory Committee.
Previous disclosures about my attendance at EASD 2018, can be found on this post.
I have spent a lot of time listening to presentations about diabetes. It’s one of the perks of the job – hearing from leading clinicians, researchers and advocates is a privilege I never take for granted.
Often, I am mesmerised as the speaker holds court, sharing details of a new study, intervention, clinical program or anything else that they are working on.
Usually, I sit there interested, listening to what is being said, live tweeting content and wondering what this means for the average diabetes punter in their day-to-day diabetes life. Occasionally I am completely and utterly blown away by something – even if it just a small comment in the overall talk – and that is what happened last Monday.
I had been asked to sit on a panel at the Roche Media event, which is a morning for health journalists. The program was jam-packed and the panel session tied together the presentations from earlier in the day. I was coming from another meeting, so unfortunately, I wasn’t there for the whole morning, but I arrived just in time to hear Professor Stephan Jacob, a diabetologist from Germany.
The theme for the whole day was ‘Connecting the Dots’, with Roche continuing to promote their development of a connected eco-system with PWD in the centre, linked with HCPs, health systems, policy makers, industry, data and more.
I have become pretty good at getting a read on the way HCP and researcher presenters regard PWD. A lot of this is in the language they use (i.e. use the word non-compliant, and it’s not looking good…). Immediately, it was clear from the way Stephan was speaking that he understood the whole self-management nature of diabetes, the burden that a chronic and demanding condition such as diabetes places on the lives of those living with it and those around us, and who is responsible for the day-to-day management of diabetes. It was also clear that he understood the barriers that we face to optimising our own care.
The moment in his talk last week that had lightbulbs going off in every direction was when he made a comment about diabetes messaging, which went something like this:
‘If someone comes into a clinician’s office and has elevated blood pressure, we take note straight away. We consider the right medication and what needs to be done, and then we usually see them again a week later, maybe less. But diabetes? When someone come in with out of range glucose levels, we may make a few tweaks; we may tell them to go for a walk after dinner; we may change some of their medications. And then we tell them to come back in three months. Three months. What does that say about urgency or seriousness? It tells that we don’t really need to do anything urgently; that it’s not important.’
I gasped when he said this, because it is so true. There is no urgency in diabetes. People newly diagnosed with type 2 diabetes may still be told that they have just ‘a touch of sugar’, which sounds like something a recipe may suggest be sprinkled on top of a freshly baked streusel cake!
We have visits every three, six and often twelve months which may be fine if everything is ticking along nicely and we just need a tune up or to check in. But what about if it’s not?
And what happens when something does occur? When we have a hypo that sends us crashing, wind up in DKA after a day or two of elevated glucose levels, or are diagnosed with complications? We are blamed for not acting swiftly enough. But why would we?
Perhaps part of the issue is that we remain so reliant on A1c checks as a measure of how we are doing, and traditionally, we do these every 3 months. But the limitations of A1c should mean that we don’t rely on that and that alone.
I was thinking to a time where diabetes has felt truly urgent for me, and really, the only time I think it did was while I was pregnant. Sudden changes to patterns in glucose levels were addressed immediately. Instead, changes to therapy were swift and aggressive, and I understood that at that moment how I needed to be diligent about keeping an eye on things, reporting issues and expecting action. And my HCPs knew it too. I had far more regular appointments and at no point during planning for or during pregnancy was I sent away with an indecisive ‘We’ll just wait and see what happens and talk about it when you are in here at your next visit.’
I also know that it was exhausting and draining and that maintaining that level of care is not sustainable in the long term. Burning out is a reality of that sort of scrutiny and constant focus.
But surely there is a middle ground in there where we all understand that while needing to live life alongside a condition and have it fit in with our daily lives, there is also no space for ambivalence or messaging that it doesn’t matter if we just trek along, happy with the status quo, for a few months.
I had a conversation with Stephan later, thanking him for his talk and telling him how that moment of his presentation really rang true. We spoke about how many people with diabetes would be feeling really unwell during periods where they were waiting for something to be done – changes to therapy made, introduction of new drugs… Were they just accepted to feel that way until they were helped to work out how to improve the situation?
Mostly, this resonated as another example of terrible messaging in diabetes; more missed opportunities to optimise care; another time that highlights how people with diabetes actual feel is ignored as we are forced to fit into a system that is not purpose-built for our condition.

Panel discussion at the Roche Diabetes Care Media event. Professor Stephan Jacob is far left. I’m the one who forgot the ‘white shirt/black jacket’ dress code. (Click for photo source.)
DISCLOSURE
Roche Diabetes Care (Global) covered my (economy) travel and accommodation costs to attend their #DiabetesMeetup Blogger event at #EASD2018 and present at their media event the day before EASD. Roche Diabetes Care also assisted with providing me press registration to attend all areas of the EASD meeting. As always, my agreement to attend their blogger day and participate in their media event does not include any commitment from me, or expectation from them, to write about the company, the events or their products.
Before travelling to Adelaide for the Australasian Diabetes Congress, I had a couple of days in Sydney, and on one of those days, Grumps and I had two meetings that I’ve not been able to stop thinking about, because in both cases, they were about people with diabetes who we rarely get to hear from.
The first meeting was with some of the team at Life for a Child (LFAC). It was great to catch up LFAC General Manager, and meet Rachel who is the program’s Marketing Coordinator.
We then jumped in a cab and headed to Canterbury Hospital and met with a diabetes educator who spoke about some of the challenges she faces working in the diabetes clinic.
Since these meetings, I’ve been thinking a lot about the people with diabetes involved in these programs. For LFAC, it is young people unable to afford insulin and other life-saving diabetes supplies, living in developing countries. And at Canterbury Hospital, it is adults with type 2 diabetes from lower socio-economic and CALD backgrounds.
I want to know more about these people and I want to hear their stories. But I don’t want them told by, or from, the perspective of a supporter or a healthcare professional. In the case of LFAC, the story shouldn’t be about someone who supports the program or what they have discovered now they’ve read about it, worked with the staff, or even met with, and perhaps worked with the people supported by the program.
I do understand that there may be a place for hearing from those with a understanding of a program or service. Dr Fran Kaufman’s article after her travels to Ethiopia was enlightening. But honestly, I now want to hear directly from some of the 3,500 children with diabetes in Ethiopia who receive their supplies from LFAC.
And while hearing about the challenges Marita and her team face at Canterbury Hospital has provided me with some level of understanding about the how the hospital systems and structures impact on her ability to work as well as she can with the people with diabetes who use the service, I really want to hear from those people to truly understand their lives with diabetes and how those challenges affect them.
It is too easy for those of us who are comfortable and confident and already have a voice to tell the stories of others. Or, even worse, to eclipse their stories. That’s not okay because they are not our stories to tell. Our words are not their words. And their stories are the ones that matter here.
If we are in a position to support (financially or otherwise) services and charities, that is great, and it’s necessary in many cases for them to exist and carry on their important work. But if then all we are speaking about is how that contribution or involvement is affecting us, how has the person with diabetes – the one utilising the service/charity – truly been heard?
I got to thinking about this because Rachel from LFAC has been doing a wonderful job making sure that the people who have received insulin and other supplies from the program do have a voice. Their stories are the ones mostly seen on the social pages of LFAC.
And then, I mentioned how I was feeling and they used the term ‘charity (or poverty) porn’ to describe the way supporters speak about their involvement in different causes. They told me that often, the people being supported are presented as ‘needing saving’, and those donating are presented as ‘saviours’.
This sat a little uncomfortably with me, because I am pretty sure that I am guilty of having written about LFAC in those terms before. I am sure I have focused my involvement in LFAC on what I can do and have done to support it; what I have learnt about the people benefiting from the program; how I feel that because I live in a country that provides access to healthcare and I can afford what the system doesn’t provide me, I therefore feel obligated to fundraise and donate.
But when I do that, I make the story about me. And the voice being heard mine. I already have a platform to speak about my own diabetes. But the diabetes here isn’t mine; the stories are not mine; the words people hear should not be mine.
And so, here is Amita’s story:
To make a donation to support children just like Amita, go here.
Last week, I spent a busy week at Australasian Diabetes Congress. I spent a lot of time with work colleagues, health professionals, the event organisers and researchers.
And I was fortunate because most of the time, I was around at least one of my peers. Between the #DAPeoplesVoice team, (Mel, Frank and David), other diabetes friends from home, (Ash, Kim, Gordon and Cheryl), and away (Grumps), there was always someone nearby who I could rely on to ‘get’ diabetes. (This is important always, but conferences have their own special challenges where diabetes mates are certainly appreciated to help keep some perspective!)
I have written countless times before about the power of peer support. I have also written that my peers have been the ones to have truly helped me through some of the most difficult diabetes situations I’ve faced – not necessarily with advice, but simply a knowing look, a nod of the head, or the words ‘me too’. Our peers help us make sense of what we are dealing with, provide us with endless support and help make us feel connected to others. And that’s important with a condition such as diabetes, because it is all too easy to feel that we are on our own.
Which is why I was so pleased to learn about ConnecT1ons, a new initiative from Diabetes Vic, which is looking to provide that support to another group within the diabetes world – parents of kids with diabetes.

It is undeniable that parents of children living with diabetes have their own brand of challenges. This was brought home to me again last week during the Diabetes and Schools Forum when parent of three children with type 1 diabetes, Shannon Macpherson, spoke about some of the difficulties she and her family have faced with her children in the school setting.
And again this morning, when I was speaking with a parent who is having a very tough time with her young, kindergarten-aged child. ‘Renza,’ she said to me, as she explained what was going on. ‘You have no idea. Having a child with diabetes is impossible because we cannot be with them when they probably need us the most.’ She’s right – I have no idea.
But other parents of children with diabetes would and do understand. And as they shared their empathy, they would also probably share some of the things they’ve done to help them through similar tricky situations.
Diabetes Victoria is looking to bring parents like this together for an event where they can meet other parents of children with diabetes. Plus, it’s a few days of respite from looking after their child with diabetes, while knowing their kid is safe (and having an absolute ball) at diabetes camp. What a brilliant idea all ‘round!
You can watch a video explaining the project here, and hear from Jade, the mum of a young boy with diabetes share some of her experiences – and how parents just like her will benefit from ConnecT1ions.
As is always the case, finding funds for initiatives like this is a struggle, so today, Diabetes Victoria launched a crown funding campaign and is seeking to raise $15,000 to run ConnecT1ons. If more is raised, they can run additional events. The crowd funding is only open for a week, so please do consider making a donation – and doing it now! Click here to be taken to the Pozible page.
Congratulations to Diabetes Victoria for acknowledging that parents of kids with diabetes are a specific group that need support amongst their own peers. Extra huge congrats to Kim Henshaw who has spearheaded this project as part of her role as Children and Families Coordinator.
Please do donate. I returned home last week after spending time with my peers feeling refreshed, energised and connected. Parents of kids with diabetes deserve to feel the same by spending time with each other.

Not a functioning beta cell amongst us.
Disclosure
None! I was sent information about ConnecT1ons from the Communications Manager at Diabetes Victoria last week, but she did not ask me to write about it. I don’t work for Diabetes Victoria (I left there back in Jan 2016) and have had nothing to do with this new initiative. But you have to admit it’s a good one. Hence, this post.
I still believe everything I wrote in this post from three years ago. And with the Australasian Diabetes Congress due to kick off next week, I thought it a good time to revisit.
People with diabetes have a place at diabetes conferences – even those designed for healthcare professionals. I truly believe that #NothingAboutUsWithoutUs needs to be the overarching philosophy when it comes to all diabetes activities, services and resources. Until we get to that place, I – and many others who feel the same way – will continue to plead our case for inclusion.
Put us on the program, on planning committees and at the front of your minds.
_________________________________________________
Following the announcement at the end of last week from Diabetes UK that a new CEO had been appointed, there was much chatter online about whether or not the best person had been selected for the role. I have no opinion on this. I do not necessarily agree that you need a person with diabetes to be the CEO of a diabetes organisation – there are many other ways that meaningful engagement can take place ensuring that the organisation is representing the needs of people with diabetes.
What I was far more interested in was the direction the discussion took – specifically about the inclusion – or, as was being discussed, not – of consumers/patients/PWD/whatever you want to call us at professional conferences.
I watched on in silence as healthcare professionals, PWD and consumer groups all weighed in on the subject.
I am rarely a fence sitter, and on this issue, my position is very clear. Very, very clear.
I have yet heard a good argument as to why PWD should not attend diabetes conferences. In Australia, just as in the UK, we have the same limitations about people with diabetes having access to drug-branded information. This is archaic because, well, the internet. But whatever. (Read more here.)
Notwithstanding these code regulations, there is no reason that a PWD should not be welcome at a professional meeting about diabetes, hearing about diabetesresearch, learning about diabetes medications and technology and talking with the healthcare professionals working with people with diabetes. And if it is deemed that we are not fit to see the brand names of drugs, then keep us out of the exhibition spaces, but allow us to attend information and networking sessions. (For the record, I don’t support that idea either, but if that is what is necessary for us to be able to attend the sessions, then so be it.)
I would go one step further. PWD should be involved in the planning of these meetings. Why? Because surely if HCPs working with PWD are hoping to improve their knowledge and understanding of diabetes, a big part of that is gaining a better understanding of people with diabetes. And there is no one who gets that more than those of us living with diabetes.
I absolutely do not subscribe to the ‘why can’t we have a professional conference for health care professionals’ viewpoint. Well, of course you can. But there is no reason that PWD should not be involved in this and attend alongside healthcare professionals.
I’ve been more than a little vocal on this in the past. Search ‘consumer involvement’ or ‘PWD at diabetes conferences’ on this blog and you might just come up with a few things. I’ve given talks both here in Australia and overseas about it. I constantly expound the value of the consumer voice and consumer participation and consumer involvement.
The thing that interested me in the discussion I was following was just how hostile it was at times. With 140 characters or fewer at our disposal, we can’t always be as tactful as we might be in person. Sometimes, being direct is the only way. And knowing a few of the people involved in the discussion, tact is perhaps not a characteristic that they generally employ. I say that without any snippiness at all – it is part of the way they get their point across. I get it – I am often accused as being like that and I wear it as a badge of honour. As far as I am concerned, the involvement of PWD is non-negotiable and if I sound pissed about it, I probably am!
But being hostile and aggressive is not likely to result in a favourable resolution.
Working for a diabetes organisation puts me in a unique position. As part of my work, I get to attend the very conferences from which other PWD are excluded. Plus I am frequently invited to speak and this privilege is due to a combination of my diabetes org work and also my work as a blogger and diabetes activist that I do outside of paid employment. It’s a sticky situation that I manage as best as possible. There are disclaimers everywhere and even the whiff of a conflict of interest is declared.
However, there is one thing that I have learnt from ‘being on the inside’ and that is working collaboratively is highly likely to produce results more than being combative. There is a lot of negotiating required at times and an understanding that things take time. Sometimes lots of it. It’s taken me a lot of time to understand that!
Call me – and those who are trying for a more collaborative approach – political or bureaucrats. You can think we’re sell-outs. We’re not. At all. We actually have a seat at the table and are working for people with diabetes. And you want us sitting at that table! Come join us.
So, think you want to get involved, but not sure how? There are myriad ways that you can try to work with organisations. If paid employment is not what you are looking for, there are many volunteering opportunities including Boards (some may be paid positions), advisory panels, expert reference groups or simply, pick up the phone and pitch your idea!

I have a very scientific way of collecting info to share in these Internet Jumbles. I make weird notes on my phone that absolutely make sense when I note them down, and then make absolutely no sense when I revisit them to put together the latest edition. (Case in point: ‘DMK mine’ had me stumped for a few hours until I realised that was shorthand for the HypoRESOLVE piece on Diabetes Mine. The DMK is because the meeting was in Copenhagen. Of course it makes sense. Perfect sense.)
Half the time, even after trying to work it out, I still can’t understand my notes, so there is a shedload of stuff I wanted to share that is still a mystery trapped in my iPhone.
But! Here are the ones I was able to decipher. Buckle up…it’s a long one.
Ask patients? That’s novel
Results of a review of international literature examining patient involvement in the design of healthcare services showed that patient engagement can inform education (peer and HCP) and policies and improve delivery and governance.
I am always interested to read these sorts of articles, but must say, my response is often an eye roll and the words ‘No shit, Sherlock’ muttered under my breath.
Research and people with health conditions
What is the role of people with health conditions when it comes to research? This editorial from BMJ suggests that full partnership is the best way.
And this infographic from Public Health Research and Practice about how to involve consumers in health research is also useful.

Thanks for listening
It’s so nice when people actually take home some tips and tricks from presentations I’ve been involved in. This tweet over the weekend from diabetes educator Belinda Moore (referring to a symposium at last year’s ADS ADEA meeting in Perth in which I was fortunate enough to be involved) was gratifying.

Peer support remains an absolute cornerstone of how I manage my diabetes as effectively as I possibly can. It is those others walking the same road who help me make sense of a health condition which takes delight in confusing the hell out of me!
The driver’s seat
This post from Melinda Seed underlines why she believes that the idea of diabetes being a ‘team sport’ is not especially accurate.
Complications and language
The awesome PLAID Journal (which you really should bookmark and read) published a piece just as ADA kicked off about why we need to change the way we speak about diabetes complications.
The piece was written by me and Chris Aldred (AKA The Grumpy Pumper), bringing together Grumps’ #TalkAboutComplications initiative and my constant banging on about language. (I first wrote about needing to reframe the way we talk about complications five years ago in this piece. Every word still holds true.)
You can reads the PLAID Journal piece here. And please share. This is a message that we need to get out.

Wellness is not the same as medicine
My huge crush on OB/GYN Dr Jen Gunter only increased after she published this piece in the NY Times last week.
I have written before about how damaging the ‘wellness industry’ can be in diabetes, including this piece on the language of wellness.
Diabetes Voice reboot
The IDF’s magazine has had a reboot and is not delivered in a digital format. Check it out here.
Well, that’s candid…
This photo of Cherise and me snapped at Diabetes Mine’s DData Exchange is hilarious in itself, but Amy Tenderich’s caption is gold!

(Click for source)
Right device, right person, right time
Dr Kath Barnard’s piece in Diabetes Medicine Matters reiterates her message from the 2017 ATTD meeting (I wrote about it here) about the importance of matching the right device at the right time for the right person.
What are the barriers to preconception care ?
This piece was just published in Diabetes Research and Clinical Practice looking at the reason women with diabetes may or may not attend pre-pregnancy care. (I was a co-author on this piece.)
‘If only there was a….online community for people with diabetes’
That comment came from a HCP at a diabetes conference a few years ago – just after someone (maybe me? I can’t remember…?) had literally just given a talk about the diabetes online community.
The DOC is not new – it’s been around for some time – and this great piece from Kerri Sparling gives a history of the DOC.
HypoRESOLVE on Diabetes mine
I was interviewed by Dan Fleshler from Diabetes Mine about HypoRESOLVE. You can read his piece here – it gives a great overview of the project.
On a break
I’m going to be taking a little Diabetogenic break for the next couple of weeks. The rest of the year is shaping up to be super busy, so I thought I’d use the next fortnight to get myself organised.
I’ll be sharing some old posts from the Diabetogenic archives and expect to be back just in time for the Australasian Diabetes Congress which kicks off in Adelaide on 22 August.
In the meantime, be well and be kind to yourself.
The Monday after National Diabetes Week is a chance to take stock, take a deep breath and take a moment to look back over the busy days.
This year’s campaign was terrific in that the messaging was strong and it got a lot of attention. It was great to see the same information being rolled out across the country, and shared internationally, too. I certainly believe the campaign’s main theme of needing to detect and treat all types of diabetes sooner resonated with people across the globe.
So, there are some of my highlights from last week:
Frank Sita can certainly claim best on ground for his relentless support of the campaign. He blogged, vlogged and SoMe’d the hell out of the campaign and was also interviewed in a great piece for The West Australian newspaper. (Plus, he nailed the #LanguageMatters talk with the journalist.) Nice work, Frank!
Diabetes NSW & ACT held their Diabetes Australia Research Program Awards on Thursday night, using NDW as an opportunity to underline the importance of research, and recognise just some of the wonderful researchers working to unwrap the secrets of diabetes.
There are far too many stories of missed type 1 diabetes diagnosis, and many were featured last week. You can see these stories on the Diabetes Australia Facebook page. It’s simply not good enough that people have to become really, really sick before they are correctly diagnosed. Everyone must know the 4Ts.
There was a most welcome announcement with Health Minister Greg Hunt launching Australia’s first national diabetes eye screening program to reduce vision loss and blindness in people with diabetes. this is a great example of Government, and industry (Specsavers will also be contributing to the program) working together and with health groups to support people with diabetes.
Bill Shorten’s Friday evening call to the Government to broaden CGM funding was beautifully timed and was a great way to end the week, providing an awesome bookmark to the previous week’s piece on The Project.
Theresa May would have no idea that she provided an outstanding opportunity for us to get in a little #NDW2018 last-minute advocacy and awareness across the national press, just by wearing her Libre sensor.
And so, it’s a wrap. Except, of course it isn’t. We still need to remind people of the signs and symptoms of diabetes. We need better detection programs. We need more awareness. This campaign doesn’t get boxed up and archived, never to be thought of again. We must keep talking about it.
Of course, National Diabetes Week may be over, but for those of us living with it, every week is diabetes week. And so on we go: ‘doing’, ‘living’ and ‘being’ diabetes.

Yesterday an article was published across Australia detailing a new report showing that Australians with diabetes are missing out on the recommended levels of diabetes care. Most of these people receive their diabetes care in general practise.
A couple of things before I go on:
- The article was behind a paywall, but Diabetes Australia shared an image of a portion of the it, and that can be accessed here. If you have access to a News Ltd. account, you can read the article here.)
- I want to say that in writing this post today I do not want to be seen to be doctor-bashing. I don’t believe that is constructive in any way whatsoever. However, I do think that there needs to be acknowledgement that the level of diabetes care in general practise is not ideal for a lot of people.
- The language of the article was atrocious. It appeared first under the heading ‘How diabetes sufferers are dicing with death’ Seriously, journos, ready the freaking Diabetes Australia Language Position Statement.
Onwards…
There was some discussion online after the article was shared, with a few doctors believing the article wasn’t all that helpful and feeling that it was unfairly unfavourable towards GPs. Someone also commented on the language used. (I’m not sure if they meant on Twitter or in the article. The language in the article was strong and very critical of GPs.)
The report is damning, and it shows that the results for people with diabetes are not good at all with only one in three people diagnosed with diabetes receiving expected standards of diabetes care. Only half had their A1c checked, and of those, only half again were in range.
This is despite there being a documented diabetes annual cycle of care (for which GPs receive funding). If completed fully, the annual cycle of care includes: annual A1c, cholesterol, and kidney checks, weight and blood pressure checks, as well as two-yearly eye and foot checks.
For me, it shows yet again how stacked the decks are against so many people with diabetes. We don’t receive the level of care recommended and then, when we don’t meet expected outcomes, or develop diabetes-related complications, we get blamed.
If we want to talk about things that are unhelpful and not constructive, let’s begin with that.
We seem to forget that most people don’t innately know what is required to manage diabetes, or what screening checks are required – especially people newly diagnosed with the condition. A lot of people rely on their healthcare professional – in the case of diabetes, usually their GP – for this.
I’ve written before that in my case, my GP is not in any way involved in my diabetes care. This is a deliberate decision on my part. I understand it is also a privileged decision – I have easy access to my endocrinologist, and other diabetes specialists for all my diabetes healthcare needs.
But that’s not the case for everyone, and a lot of people are reliant on their GP for all their diabetes clinical care.
People with diabetes are being let down.
Even though pointing fingers and appropriating blame is not necessarily helpful, it’s what we seem to do. We can blame the system. We can blame a lack of funding. We can blame a lack of continuity of care. We can blame the fact that there are no coordinated screening programs. We can blame the need for more specialist care. We can blame a lousy and ineffective electronic records system.
But what we can’t do is blame people with diabetes. No one asks to get diabetes. No one asks to get diabetes-related complications. So how is it possible that in a system that is letting us down, we are the ones blamed when it happens?
Also, this week, we have heard story after story of missed type 1 diabetes diagnoses with people reporting that despite seeing their GP (often repeatedly) about their symptoms, they were not checked for type 1 diabetes.
It is undeniable that some GPs simply do not know enough about diabetes to diagnose it in the first place, and then to treat it in an ongoing and effective way, and this is leading to those of us living with it not receiving an adequate level of care to live as well as possible with diabetes.
While there may be some hard truths in the report, hopefully the result will be better care for people with diabetes. Because, surely, that is all that matters.







