
You are currently browsing the category archive for the ‘Awareness’ category.
I know diabetes, and not much else. I have a few other health conditions that are no more than niggling, requiring minimal effort and engagement with healthcare professional. But they still do need some sort of attention and treatment. The stark difference between that treatment and the treatment for diabetes is that I never have to jump through hoops to get treatment for them.
The other day, I had to go and have imaging on my elbow because said elbow hurts, the doctor thinks it’s tennis elbow which is now being referred to as latte elbow around here because the last time I picked up a tennis racket, Yannick Noah was ranked in the top 10.
I went to the GP, told him what was wrong, and he wrote a referral straight away for an ultrasound and Xray and sent me on my way. Three days later, I had the scans done and today I’m waiting for a telehealth appointment to discuss treatment. There was no ‘let’s wait and see’ if it gets worse.
Diabetes seems to be a lot about waiting and seeing. Or use of arbitrary numbers to determine if something can be used. Or bargaining: you may have <x device/treatment>, but you must do <y intervention> first, even if <y intervention> is not want the PWD is remotely interested in.
When I wanted to start on a pump twenty years ago, I had to go doctor shopping until I could find a doctor who would agree to filling out the requisite forms so my private health insurance would cover the cost of the pump. This was twenty years ago, and while pumps had already been around for a number of years by then, there really weren’t all that many Australians using them, so finding an endo comfortable with the whole thing was not easy.
My first endo told me I hadn’t had diabetes long enough to consider using a pump. Subsequent shopped doctors told me a) my diabetes wasn’t serious enough to warrant a pump, b) my A1c wasn’t high enough to use a pump, and c) my A1c was too low to use a pump.
It took a while before I found a doctor whose response to my ‘I want to use an insulin pump’ was ‘Sure, where do I sign?’.
When CGM came out I’d already found myself the sort of doctor who was more than happy to be guided by what I wanted, because she understood that I knew my diabetes best and therefore was the best person to decide what I wanted in my management arsenal. She’s still my doctor. There’s a reason for that!
Last week, I tweeted this:

The replies and discussion that this tweet started are really not a great snapshot of person-led care. In fact, it’s more like example after example of PWD being told no for not especially great reasons.
It seems that there are two main barriers which are intertwined in some ways.
The first is that HCPs continue to act as gatekeepers of diabetes technologies, deciding who is allowed to access what particular devices and when that can happen. This is problematic and harks back to a time when people with diabetes were mere patients, gratefully accepting what care was doled out to us without question.
Some might think that this sort of archaic attitude is no longer around, but a glance through the replies shows that, sadly, that isn’t the case.
The other barrier seems to be a whole heap of rules that seem to have no purpose other than expecting the person with diabetes meet them before they are deemed worthy of whatever it is they want.
Some of the rules seems arbitrary, others probably come from a sensible place, but are not what person-centred care is about. Many don’t seem to be based in any kind of evidence at all. Regardless, all they do is promote a one size fits all process that must be met before a PWD can proceed, verifying our merit along the way.
The very idea that we need to prove ourselves worthy of a diabetes treatment is offensive. We didn’t need to prove ourselves worthy to be diagnosed with diabetes, so why should we need to do so to have access to the technologies that are there to help us manage it? Why should we need to have diabetes for a certain about of time first, or do an education course that is not necessarily directly related to what we are searching for, or reach a certain A1c to earn our right to access and utilise a piece of diabetes tech?
(There is a third barrier unique to US DOC friends, and that is insurance requirements…. I don’t know all that much about insurance in the US, but I guess it is HCPs employed by, or advising the insurance who set up the ridiculous hurdles and hoops people with diabetes are expected to navigate.)
Now, obviously, there is the (not by any means insignificant) issue of cost. I understand that there is never an endless pot of cash to support people with diabetes. But even in places where there is funding available, or cost is to the individual – not the health system – there are still barriers in place.
Living with diabetes is a constant, tough gig. If we are searching for something to help us through, and we have made the decision that we want to try something new, surely the role of our HCPs is to work with us rather than stand in our way. The holy grail for so many people with diabetes that I speak to is to make diabetes easier. And yet, all these barriers just make it more difficult. That hardly seems fair.
Today is the day. The centenary of what remains one of the greatest medical discoveries ever. Here is a reworked post (first published here). There is not a day that I am not grateful for this discovery. And not a day goes by when I am not aware that the diabetes life I live and the access I have is not the same for everyone around the world.
And so today seems a really good day to make a donation to a charity that supports people with diabetes who need it. For me, when deciding which diabetes charities I’ve decided to donate to, it’s been important that the support is tangible. And that’s why I have repeatedly written about Life for a Child, and Insulin for Life on this blog, and supported them with regular donations for a number of years. Their works provides on the ground support, medications, diabetes supplies, education, as well as doing research. They also have an advocacy function, raising awareness of not only the work they do, but the people they support.
If you are able to make a donation it’s a great day to do it. In amongst the celebrations it’s important to remember not everyone will be able to do that today. Remembering them on this important day in diabetes history is very fitting.
Donate to Insulin for Life
Donate to Life for a Child
______________________________________________________________
There has been lots of discussion about what happened 100 years ago today – on 27 July 1921. University of Toronto scientists Fredrick Banting and Charles Best successfully isolated the hormone insulin. Today, that means that I am alive and kicking, 20 years after my islets stopped making any.
It means that type 1 diabetes treatment moved from being a starvation diet and not much else, to injecting a drug that was life giving and life saving.
It means that I take a drug that while giving me life, is also lethal and if not dosed carefully and with great consideration can cause terrible side effects.
It means that people with diabetes don’t die terrible, agonising deaths simply because they were diagnosed with diabetes.
It means that I need to be able to do crazy calculations to ensure what I put into my body completely and utterly imperfectly mimics what those with functioning islet cells do completely and utterly perfectly.
It means that there is a treatment therapy that gives us hope and life and allows us to live – sometimes very long, long lives.
It means that each and every day I feel fortunate to have been born when I was and not 100 years earlier.
It means I take for granted that I have access to a drug that keeps me going.
It means that there are far too many people around the world who still do not have access to the drug I take for granted. And 97 years later, that is not good enough.
It means that it was 97 years ago – 97 years ago – since the discover of insulin to treat diabetes and we are still without a cure.
And it means that I wonder when there will be the next breakthrough that is as significant and meaningful and life changing and life saving as what those two Canadian scientists discovered 97 years ago.
But mostly. It means that I live with hope. Hope that those scientists are somewhere working away, and perhaps – just perhaps – are about to find that next big breakthrough.

I’ve just placed an order so I can have this print in my office at home.
Alex is donating 20% of all sales of this print to Type 1 International, another charity I have written about a number of times, and supported financially.
You can see more artworks by Alex at her website, Diabetes by Design.
A week out from National Diabetes Week, and this piece has been sitting in my ‘to be published’ folder, just waiting. But the post-NDW exhaustion coupled with lockdown exhaustion, plus wanting to make sure that all my thoughts are lined up have meant that I haven’t hit the go button.
In the lead up to NDW I wrote this piece for the Diabetes Australia website. That piece was a mea culpa, acknowledging my own contribution to diabetes-related stigma and owning it. I also stand by my thoughts that the stigma from within the community is very real and does happen.
But what I didn’t address is just where that stigma comes from. Those biases that many people with type 1 diabetes (and those directly affected by it) have towards type 2 diabetes come from somewhere, and in a lot of cases that is the same place where the general community’s bias about diabetes comes from. It is all very well for us to expect people with type 1 diabetes to do better, but I’m not sure that is necessarily fair. I think that we should have the same expectations of everyone when it comes to stamping out stigma.
And so, to the source of stigma and, as I’ve said before, it comes from lots of places. As someone who has spent the last twenty years working in diabetes organisations, I know that the messaging my orgs like (and including) those that have paid my weekly salary has been problematic. I still am haunted by the ‘scary’ campaign from a few years ago that involved spiders, clowns, and sharks. (If you don’t remember that campaign, good. If you do, therapy works.)
For me personally, I don’t think much stigma I have faced has come at the hands of other PWD. Sure, there’s the low carb nutters who seem to have featured far too frequently on my stigma radar, however, the most common source of stigma has undoubtedly been HCPs.
It’s not just me who has had this experience. The majority of what I have seen online as a response to experiences about stigma involves heartbreaking tales of PWDs’ encounters with their HCPs.
While I will call out nastiness at every corner, and no stigma is good stigma, it must be said that there is a particular harm that comes when the origin of the stigma is the very people charged to help us. Walking into a health professional appointment feeling overwhelmed, scared, and frustrated only to leave still feeling those things, but with added judgement, shame and guilt is detrimental to any endeavours to live well with diabetes. In fact, the most likely outcome of repeated, or even singular, experiences like that is to simply not go back. And who could criticise that reaction, really? Why would anyone continually put themselves in a situation where they feel that way? I wouldn’t. I know that because I didn’t.
It’s one thing to see a crappy joke from a comedian who thinks they’re being brilliantly original (they never are) or the mundane, and almost expected, ‘diabetes on a plate’ throwaway line in a cooking show, but while these incidents can be damaging, they are very different to having stigmatising comments and behaviours directed at an individual as is often the case when it is from a HCP.
Of course, HCPs aren’t immune to the bias that forms negative ideas and opinions about diabetes. In the same way that people with type 1 diabetes form these biases because those misconceptions are prevalent in the community, HCPs see them too. Remember this slide that I shared from a conference presentation?
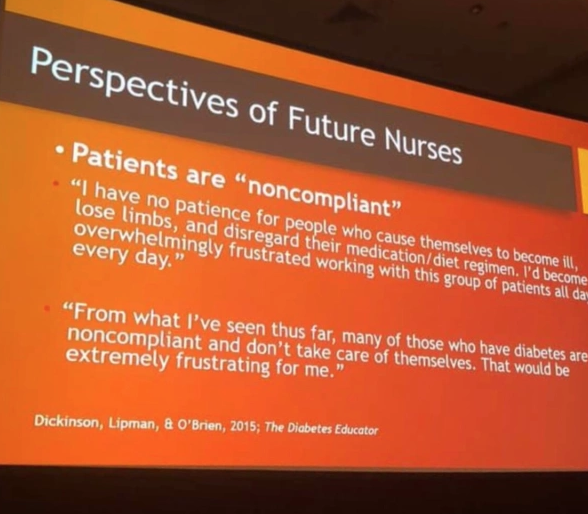
This came from student nurses. Just think about that. Students who were training to be HCPs who would inevitably be working with people with diabetes. A I wrote at the time:
‘They hadn’t even set foot on the wards yet as qualified HCPs. But somehow, their perceptions of people with diabetes were already negative, and so full of bias. Already, they have a seed planted that is going to grow into a huge tree of blaming and shaming. And the people they are trusted to help will be made to feel at fault and as though they deserve whatever comes their way.’
Is it any wonder that, with these attitudes seemingly welded on, that people with diabetes are experience stigma at the hands of their HCPs?
The impetus can’t only be on PWD to call this out. And the calls to fix stigma can’t exclusively rest on the shoulders of PWD – we already have a lot of weight there! It must come from HCPs as well – especially as there is such a problem with this group. Perhaps the first step is to see real acknowledgement from this group of their role here – a mea culpa from professional bodies and individuals alike. Recognising that no one is immune to the bias is a good step. Owning that bias is another. And then doing something about it – something meaningful – is how we make things better for people with diabetes. I really hope we see that happening.
More about this:
Becoming an ally – how HCPs can show they’re really on our side.
Ask a group of people with diabetes about their experiences of stigma, and for examples of the sorts of things they’ve heard and before long you’ll be able to compile a top ten list of the most commonly heard misconceptions that have contributed to diabetes having an image problem. When I’ve asked about this recently, the main perpetrators of these seemed to be healthcare professionals. More on that later this week.
This year, in the Diabetes Australia National Diabetes Week campaign about diabetes-related stigma, two videos have been produced and they’re almost like a highlight reel of some of the stigmatising things people with diabetes hear.
Let me tell you something I found really interesting. As part of the testing of these, I showed them to a heap of people with diabetes and a heap of people without diabetes. The reaction from people with diabetes varied from sadness (including tears), to anger and frustration, and mostly, recognition in everything they saw.
The reaction from a number of people without diabetes was disbelief that this really happens. They simply couldn’t believe that people would be so insensitive; so cruel, so shaming.
However, for so many people with diabetes, this is our reality.
Here’s one of the two videos we produced. (You can watch the second one here.) Already, this is being shared widely in our own diabetes community. I’ve lost count of the places online I’ve seen this shared. Keep doing so, if you can. Because clearly, we need to get the message out to those without diabetes so they understand that not only is this sort of stigmatising behaviour harmful, but it is also horribly common. And it needs to stop.
DISCLOSURE
I work for Diabetes Australia, and I have been involved in the development of the Heads Up on Diabetes campaign. I’ve not been asked to share this – doing so of my volition, because I think the messaging is spot on. The words here are my own, and have not been reviewed prior to publication.
I don’t know too many people living with diabetes who haven’t experienced stigma. I know I certainly have. In twenty-three years of living with diabetes, it’s come from all directions: the media, healthcare professionals, work colleagues and even family and friends. That’s because people outside the diabetes community often have pre-conceived ideas about what diabetes is all about, and a lot of those ideas are plain wrong.
But stigma doesn’t only come from outside the community. In fact, for some people with diabetes, some of the most harmful and hurtful experiences of stigma has actually come from other people with, or affected by, diabetes. [Click here to read more…]

DISCLOSURE
This piece was published today on the Diabetes Australia website, and I wrote it as part of the organisation’s National Diabetes Week campaign on diabetes stigma. I work for Diabetes Australia, and am sharing this because I’ve chosen to – not because I’ve been asked to. The words here are my own, and perhaps the only thing missing from the published text is some of the decorative language I often use when speaking about diabetes-related stigma. Bottom line – all stigma sucks. Let’s #EndDiabetesStigma now.
Gosh, I love baking a cake! It’s excellent therapy, super relaxing and is one of my favourite stress busters. I can pretty much guarantee to turn out something that not only looks Instagram-pretty but will also taste divine. I’ve written before that one of the reasons I love baking so much is because it is the exact opposite of diabetes: I know precisely what I’m going to get when I follow the steps of the recipe, and know enough that when I’m making things up as I go along what works, what doesn’t and what will yield the best results. Which is the polar opposite of diabetes, where following a ‘recipe’ guarantees nothing but confusion, frustration, and a completely different result to yesterday, and making it up can mean winding up with a rollercoaster or a straight line on the CGM. No one knows. It’s a mystery. It makes no sense to anyone.

Next week is National Diabetes Week here in Australia, and focus is going to be on diabetes-related stigma. I’ve spent a lot of time in recent weeks involved in the preparation of our campaign, listening to people with diabetes share their stories. You can check out this post on the Diabetes Australia Facebook page to see people sharing some examples of stigma they’ve experienced. It’s heartbreaking. It shouldn’t be happening.
I am very conscious that in the past I’ve probably contributed to stigma associated with type 2 diabetes. I’m horrified by it, and ashamed. I should have known better, and maybe if I’d bothered to learn from people with type 2 diabetes, I would have been more sensitive. When we blame and shame diabetes, we are blaming and shaming real people living with diabetes. I seemed to have forgotten that when I thought it was okay to demand that my diabetes was seen as the more serious diabetes, and that people make sure that they get my type of diabetes right.
And that brings me back to my cakes. And cakes in general. And comments about cakes. Especially comments about cakes being ‘diabetes on a plate’. They’re not. We all know that, right? And we all know that they are not any type of diabetes on a plate. Right?

And we know that when some idiot on a cooking show refers to a delectable, rich dessert as ‘diabetes on a plate’ that demanding clarification about ‘WhAt TyPe Of dIaBeTeS yOu MeAn’ is only contributing to the stigma. Right?
Right?
Stigma sucks. It really does. It makes people just want to curl up and hide from others, and hide their diabetes. It makes people feel ashamed and guilty and, really, that’s just not fun at all.
We don’t all need to love each other in the diabetes world – god knows that there are people who steer clear of me, and I am more than happy to return that favour – and we don’t need to align our advocacy efforts. But maybe we can all agree that all stigma associated with any type of diabetes is pretty nasty. That actually seems like a pretty simple thing upon which to agree.

That time I wrote about this (and then a HCP misread it as me saying PWD don’t need to know what type of diabetes they have. It doesn’t say that…)
That time I owned my own shitty behaviour.
That time I wrote about how heavy diabetes stigma is.

I generally don’t do my best work at 2am. I’m just not the spring chicken I used to be, and being awake, engaging and remotely coherent when I am usually in the middle of some decent REM sleep is a big ask these days.
But living in Australia, and wanting to remain as active as possible in global diabetes work and activities has meant that I have had to suck it up and learn to get on with it. I’ve become expert at stealthily getting up about so as not to wake my family, moving like a ninja about the house. I make a pot of tea, have hypo supplies handy, and layer on red lipstick to create the illusion of being alert and awake, completely together and impossibly glamourous (I fear I am only fooling myself) before settling into do whatever it is that I am needed to do in the wee hours.
Last night, it was a 1.30am call for a 2am event. I’d snuck in a couple of hours sleep ahead of the rude alarm that woke me. When I logged onto the event platform, I still had my ‘morning voice’ on, but the hot tea helped lubricate – and wake up – my vocal cords. Thankfully I was only required to speak and not sing an opera. (Silver linings!)
But despite grumbling about the hour, I’m glad I did it. Because the following couple of hours was a discussion about hypoglycaemia that combined lived experience stories from people with diabetes, peer support, all articulated with fabulous input from clinicians and researchers. It really was an exercise in how to put together an online diabetes event!
The event was the Lilly Hypo Summit, and I co-hosted with Bastian Hauck who is an absolute pro in any hosting seat. When I was asked to be involved, I had visions of a very staged and scripted event. I have worked with industry enough to understand that their compliance rules often means that events are required to be defined to the nth degree with all content being scrutinised by legal eyes, leaving little room for spontaneity or free discussion. How could we possibly get the true experience of hypos across if we were constrained by needing to stick within a pre-planned programme? I mean, hypos don’t do that, so discussions about them surely shouldn’t have to – and simply couldn’t if we were to do it justice.
Amazingly, we managed to put together an engaging and somewhat impulsive and free-formed event with full support from the global engagement team. They trusted the PWD who were shaping the event enough to understand that what we were trying to do was be respectful to the people telling their stories by not in any way censoring them. Plus we promised no one would throw caution to the wind, and talk about replacing their traditional diabetes management with bathing under a full moon and dancing to the beat of an inner drum (or something), which considering last night was a full moon, was a pretty important promise to make. We created a space for PWD to share their stories and highlight the incredibly complex challenge that is hypoglycaemia, and we punctuated those stories with research and clinical advice.
I knew that it was going to be a good event, because the speakers were remarkable. When it was over, I had dozens and dozens of messages from people congratulating me on my hosting, but there is a secret that I feel I should share. Hosting is impossibly easy when you are interviewing brilliant people. And it was programme overflowing with brilliant people. The PWD who spoke had fascinating tales to tell, and told them in wonderfully disarming ways. I’d not met them all and it was great to be just as surprised as the audience when hearing their stories. And then we had two remarkable researchers who I respect greatly, and I know to be incredible communicators.
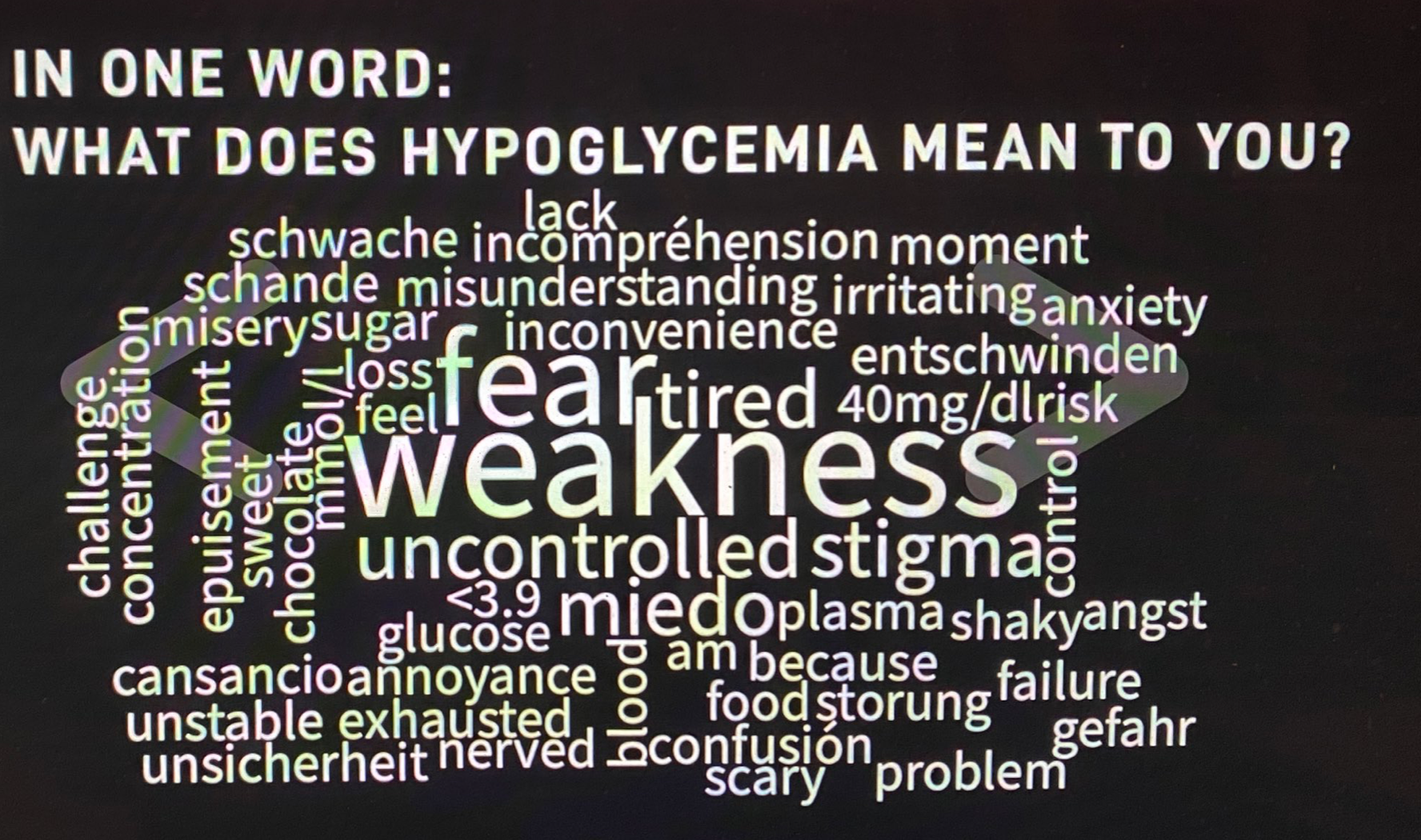
I really want to write more about what was discussed at the event, and will try to do that in upcoming posts, but for now, I just want to share this world cloud. We asked people to describe their hypos in one word. I’ve done exercises like this before and they never, ever reveal the same words. This is what the group came up with last night:
But to finish this post, I want to ask the question that one of last night’s HCPs, Pratik Choudhary, from the Leicester Diabetes Centre in the UK, asked us: ‘Do you see hypos as a slope or a cliff face?’ I can’t stop thinking about this, because I’ve never been asked about hypos this way, but it makes so much sense to consider them in this context. Of course, there are so many factors at play, but this either / or scenario does perfectly capture the in-the-moment way that I feel about hypos. I wonder what you might think about your hypos. Does it fit in here, or is it something completely different?
DISCLOSURE
I was an advisor to Lilly Diabetes for the Hypo Summit. I have been paid for my time. I have not been asked to write anything about the summit, but am sharing because there was so much amazing content at the event. No one has reviewed this post prior to publication.
‘It doesn’t matter to me; therefore, it doesn’t matter.’
Recently, former Prime Minister of Australia, John Howard was asked if he thought Australia was a racist country. This was in response to a survey which showed that 76 percent of respondents believed racism is indeed present in Australia. He replied: ‘That has not been my experience. I have to respectfully, to that 76 per cent, say I don’t think there is underlying racism in Australia’. Surprise, surprise. The privilegest, whitest, mannest of privileged white men has had no experience of racism in Australia.
I talk about privilege a lot, and I acknowledge mine daily. It’s an important and integral part of what I think about when working and playing in the diabetes space. Perhaps it’s because I’ve been working professionally in advocacy roles for a long time, often advocating for things that really don’t have all that much baring on me. But not once have I ever thought ‘That doesn’t matter to me, so it’s not important, and doesn’t matter, to others’. That is critically important in my role at Diabetes Australia, because a lot of the work that I am involved in have little impact on my own diabetes management.
And in my role as an activist outside of my day job, it is also important. When sharing my story or opinion, the two things that are important for me to relay (usually right up front) are that my story is but one story, and that due to circumstances well beyond my control, I am fortunate in many ways when it comes to access and affordability of diabetes healthcare and technologies.
It’s for that reason that I get a little testy when people put down what others are doing with their own management, critical of others’ advocacy passions, or dismissive of someone’s opinion.
Living in similar circumstances isn’t a guarantee of having the same experiences. Even when I am speaking with PWD whose situation may be similar to my own, I accept that what matters to me may not necessarily matter to them, and how I respond to certain circumstances may be different to their response. And vice versa. But I never ever belittle how they feel, or what they are for. And I never suggest that they are hysterical, or overreacting or being needlessly dramatic for feeling and behaving the way they do.
It does happen though.
I’ve seen people with diabetes shot down in our own community by others who have different opinions. Or if are really upset about something. And I’ve seen people scorn advocacy activities, or support and education programs that they think are unnecessary.
I’ve been on the receiving end of criticism from people who don’t think the language matters movement is important. They say they have never felt stigmatised or judged, or that the words used by others about diabetes don’t negatively impact them, and therefore the whole movement is unnecessary.
Not everyone has to have the same beliefs about diabetes. But to dismiss something because it’s not important to you is arrogant. And often, it’s because of privilege. Having the confidence to say something when you don’t like what you are seeing or hearing, or not needing a service or a resource does not mean it’s pointless. It just means that you have that already, or don’t feel you need it.
There is a level of meanness to this as well. And an antagonism. It undermines others’ experiences and feelings. And it is a really crappy way of undercutting the work done by others. And it is, in effect saying, ‘Not important to me so not important at all’.
Last week, a response to an incident that happened during Australian Fashion Week resonated with me and the reaction by the woman at the centre of it all was interesting. Lisa Cox is a model who closed out the show, and as she made her way on the runway, something got caught in the wheel of her wheelchair, and she needed assistance in getting moving again. This was a high-profile show, and it got a lot of coverage. Many people from the disability community commented to say that while there may have been a few disabled models involved in the show, the end product was one of inaccessibility. They spoke about how Lisa’s runway experience mirrors their everyday experiences, with no thought given to people using wheelchairs or other mobility aids.
Lisa wrote a piece for online women’s news network, Mamamia, about how horrified she was at this response from others in the disability community. She said that she wasn’t fazed, that being in a wheelchair means this sort of thing happens all the time, and she just gets on with it. It’s no big deal to her, and others should also just get on with things.
Which is great! Her response is no less significant than others with opposing views. Others who have a different reaction have every right to be heard just as loudly. And they should not be called ‘difficult’, ‘angry’ or ‘aggressive’ for communicating their views in their own way. Appearance activist, Carly Findlay has made some excellent points about this issue, also addressing how it’s not okay that people are criticised for how they are addressing their concerns. Tone policing is rife. (You can read more from Carly here.)
This goes far beyond the disability and other health condition communities. It is relevant when talking about women’s rights, LGBTQIA+ rights, and of course, when addressing racism.
So, what happens when an incident like the one at Fashion Week, or a discussion about an issue like language pops up? Predictably, devil’s advocates jump on to suggest that ‘It’s a start’, ‘At least it’s something,’ or ‘They tried’. To that, I say, ‘A start is tokenism, and it isn’t enough’, ‘Don’t tell me I must be grateful for the bare minimum’, and ‘Try harder’. The thing is, devil’s advocates are often in a position of privilege, and when they don’t look beyond their own experience, that privilege is on show. Front and centre.
More musings on privilege
This is what diabetes privilege looks like.
I really wanted to call this piece ‘Hey, ableds, leave our kit alone’, but decided against it.
Over the weekend, two main things seemed to dominate diabetes twitter. The first was the suggestion from a nurse (in a now deleted tweet) that shoving cake frosting (more commonly called icing in my parts of the world) up the arse (more commonly called ass in other part of the world) of an unconscious person with diabetes was an excellent hypo treatment. The second was this picture:

Let’s just say that sexually assaulting a PWD to give them glucose is not a good idea, no matter how hypo you think they are. Call an ambulance, rub some frosting (or honey etc.) on their gums, or, if they have glucagon with them, and you what to do with it, use that. Once again, just to be completely and utterly clear, decorating the arse of people with diabetes as if it’s a plain tea cake in need of some ready some embellishing and sprinkles, is not appropriate without consent. If everyone is conscious and there is consent, do whatever you will.
With that out of the way let’s move to the second fun little incident and that photo. That’s right, it clearly refers to one of the diabetes devices that I and many others use to keep an eye on our glucose levels because the bit of our body that takes care of it broke.
Even before this photo appeared, there has been a lot of commentary from people with diabetes (PWD) about people without diabetes (non-PWD) using any sort of glucose sensing device. I think that in coming years we’re going to only see more of it as the makers of CGMs and Flash GM start to advertise the allure of glucose tracking to a broader audience, or, as is the case with the little photo above, third party app makers jump on board.
Because the diabetes community never has one united opinion on things, (although I’m yet to have heard from a PWD who has thought the icing-up-the-bum-for-hypo-treatment idea is a good one), some people are violently opposed to the idea of non-PWD using CGM. Others couldn’t be less fussed about it if they tried. And some actually think it’s great. There is no one way to respond, and everyone’s feelings are valid.
I have a lot of feelings wondering why non-PWD would want to do diabetes. From hypo simulators, to wearing a pump with saline in it, and lining up to get an A1c checked for fun – I’ve seen it, and I’ve written about it. Again, no one needs to agree with my feelings, although it seems from the feedback I get, a lot of people do.
But I have to say that the idea of CGMs as a weight loss tool was a new one for me. I understand that some people who are deep into the keto way of life use them, but my understanding of this is so they can repeatedly prove to themselves (and badger others) that eating meat causes minimal changes to glucose levels, but eating grains of rice make lines move.
I did a bit of a deep dive into the company behind this picture, (they are not the only one that is moving to capitalise on the excitement and interest around biohacking) and all I could find was a whole lot of pseudo-science speak that just screams scam to me! It preys on the insecurities of those who are trying to find happiness in the latest and greatest wellness fad. But this time, they claim to have science on their side.
This isn’t new. Weight loss cons from ‘teatoxes’ to fat-busting pills to miracle diets to superfood super-promises, have been around for years. There is a reason that new players come onto the market every week, and that reason is not because they work. It’s because we have diet industry worth billions, we have people – often young girls – being told their worth is tied up in the number on their scales, and we have people desperately looking for something that will work to get them to that number, and get them there quickly.
To explain their claims, they use science-speak to suggest that there is a medical side to what they are doing. It seems that the ‘trust me, I’m a doctor’ line works well for a lot of people. As do the words around graphs, data and glucose statistics. That might work for people who haven’t spent a shedload of time around doctors talking about graphs, data and glucose stats, but those of us who do, might see this as a load of bullshit.
This, directly from the company’s website claims that the app ‘…provides an immersive experience that shows you a continuous line graph of your glucose data; provides alerts when glucose spikes or dips out of your weight-loss range’.
Weight-loss range? I really don’t understand what that means because the only time my glucose levels have equalled weight loss is when they have been off-the-charts high. Such as before I was diagnosed with diabetes, and the time I was in DKA thanks to gastro. I doubt that the idea is to somehow send people without insulin-requiring diabetes in DKA, because that is going to take a lot more than just banging a sensor on your arm, and loading an app onto your iPhone.
Of course, that’s not what they mean. They are suggesting that by keeping glucose levels withing a tight range (the ‘weight-loss range’), there will be no excess glucose needing to be stored as fat.
There is limited evidence to support that measuring glucose levels on non-PWD is beneficial, so the science is shaky to say the least. But that doesn’t stop the program being presented as super science-y and evidence-based. And for a lot of people, that illusion of science means they think that the subscription cost (because there’s always a subscription cost!) is worth it.
But let’s move away from that for a moment, let’s ignore the lack of science, the cost and the hint that this could be nothing more than a money-making scam, targeting vulnerable people, because there is more that comes into play which explains why so many in the diabetes community push back at non-PWD wearing diabetes devices.
Continuous glucose monitors were created for people with diabetes to better manage our condition. They give us access data that helps managing our diabetes like never before. They are life changing. They are life saving. They are also only available to a small percentage of the global diabetes population. I haven’t even touched on the fact that generally, it’s only people with type 1 diabetes who have access. People with other types of diabetes are even less likely to be able to get subsidised or funded CGM, even though many of them might benefit from using them.
The idea that CGMS are toys of privileged biohackers, and being used exclusively as a weight-loss tool does not sit well with many. It does not sit well with me. If I look at Australia, only half of people with type 1 diabetes have subsidised access to CGM. The rest of us are left to having to find about $4K per year to fund the devices that really make a difference to our lives, that some of us say we couldn’t live without.
The weight-loss focus from this particular company is problematic when considering the higher rates of disordered eating, and insulin omission or restriction in people with diabetes for the purposes of weight loss. Some claimed that seeing CGMs heralded as being about weight loss, when they are using it as part of their eating disorder recovery was triggering. These factors all come into play within the diabetes community.
And finally, the idea that increasing use to a far broader community will bring down the cost…? Let’s just be reasonable about that (or sceptical…) and say that’s not going to happen. If that was the case, the fact that every keto-follower worth their ketosis now regularly checks their ketones, would mean that blood keto strips would be cheap as chips. That’s not the case at all.
The potential of medical devices being used outside of the reason they were created is likely to be explored a lot more in coming years. With (non-healthcare) tech companies moving into the space, it is not only possible, but highly likely, that glucose sensing (albeit non-invasive) will become standard on wearables, in the same way step counters have. But we’re not there yet. Right now, the best use of these devices is where the evidence points – on the arms (or bellies, or thighs, or wherever!) people with diabetes are wearing them, to assist with diabetes management, to help us with our decision-making process, and to improve our lives.
NOTE:
In this piece, I mean ALL people with ALL types of diabetes, including pre-diabetes. Basically, any condition that means an individual needs to consider glucose levels.






