
I generally don’t do my best work at 2am. I’m just not the spring chicken I used to be, and being awake, engaging and remotely coherent when I am usually in the middle of some decent REM sleep is a big ask these days.
But living in Australia, and wanting to remain as active as possible in global diabetes work and activities has meant that I have had to suck it up and learn to get on with it. I’ve become expert at stealthily getting up about so as not to wake my family, moving like a ninja about the house. I make a pot of tea, have hypo supplies handy, and layer on red lipstick to create the illusion of being alert and awake, completely together and impossibly glamourous (I fear I am only fooling myself) before settling into do whatever it is that I am needed to do in the wee hours.
Last night, it was a 1.30am call for a 2am event. I’d snuck in a couple of hours sleep ahead of the rude alarm that woke me. When I logged onto the event platform, I still had my ‘morning voice’ on, but the hot tea helped lubricate – and wake up – my vocal cords. Thankfully I was only required to speak and not sing an opera. (Silver linings!)
But despite grumbling about the hour, I’m glad I did it. Because the following couple of hours was a discussion about hypoglycaemia that combined lived experience stories from people with diabetes, peer support, all articulated with fabulous input from clinicians and researchers. It really was an exercise in how to put together an online diabetes event!
The event was the Lilly Hypo Summit, and I co-hosted with Bastian Hauck who is an absolute pro in any hosting seat. When I was asked to be involved, I had visions of a very staged and scripted event. I have worked with industry enough to understand that their compliance rules often means that events are required to be defined to the nth degree with all content being scrutinised by legal eyes, leaving little room for spontaneity or free discussion. How could we possibly get the true experience of hypos across if we were constrained by needing to stick within a pre-planned programme? I mean, hypos don’t do that, so discussions about them surely shouldn’t have to – and simply couldn’t if we were to do it justice.
Amazingly, we managed to put together an engaging and somewhat impulsive and free-formed event with full support from the global engagement team. They trusted the PWD who were shaping the event enough to understand that what we were trying to do was be respectful to the people telling their stories by not in any way censoring them. Plus we promised no one would throw caution to the wind, and talk about replacing their traditional diabetes management with bathing under a full moon and dancing to the beat of an inner drum (or something), which considering last night was a full moon, was a pretty important promise to make. We created a space for PWD to share their stories and highlight the incredibly complex challenge that is hypoglycaemia, and we punctuated those stories with research and clinical advice.
I knew that it was going to be a good event, because the speakers were remarkable. When it was over, I had dozens and dozens of messages from people congratulating me on my hosting, but there is a secret that I feel I should share. Hosting is impossibly easy when you are interviewing brilliant people. And it was programme overflowing with brilliant people. The PWD who spoke had fascinating tales to tell, and told them in wonderfully disarming ways. I’d not met them all and it was great to be just as surprised as the audience when hearing their stories. And then we had two remarkable researchers who I respect greatly, and I know to be incredible communicators.
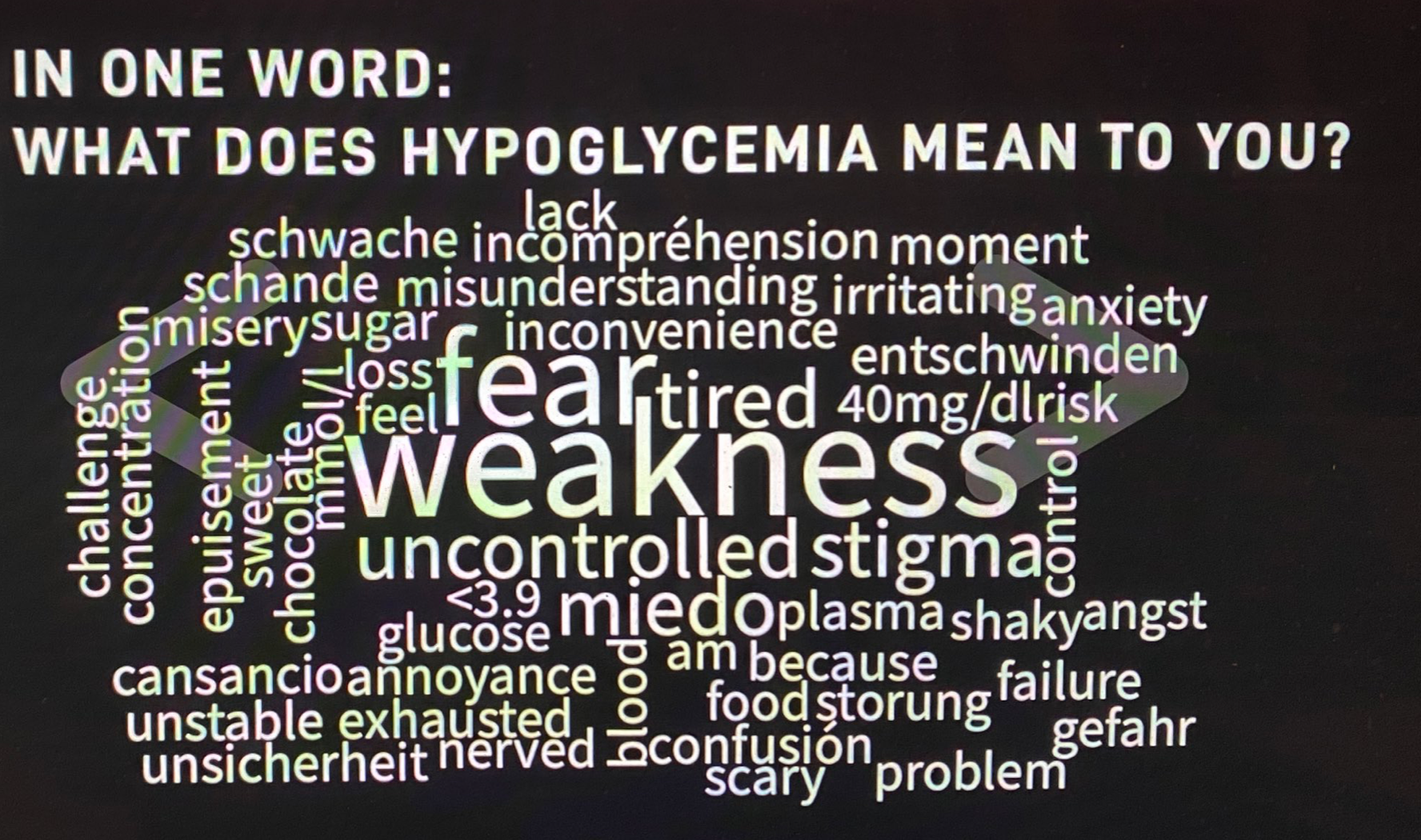
I really want to write more about what was discussed at the event, and will try to do that in upcoming posts, but for now, I just want to share this world cloud. We asked people to describe their hypos in one word. I’ve done exercises like this before and they never, ever reveal the same words. This is what the group came up with last night:
But to finish this post, I want to ask the question that one of last night’s HCPs, Pratik Choudhary, from the Leicester Diabetes Centre in the UK, asked us: ‘Do you see hypos as a slope or a cliff face?’ I can’t stop thinking about this, because I’ve never been asked about hypos this way, but it makes so much sense to consider them in this context. Of course, there are so many factors at play, but this either / or scenario does perfectly capture the in-the-moment way that I feel about hypos. I wonder what you might think about your hypos. Does it fit in here, or is it something completely different?
DISCLOSURE
I was an advisor to Lilly Diabetes for the Hypo Summit. I have been paid for my time. I have not been asked to write anything about the summit, but am sharing because there was so much amazing content at the event. No one has reviewed this post prior to publication.







2 comments
Comments feed for this article
June 25, 2021 at 9:33 pm
Min
Hmmmm, well there are hypos and there are H Y P O S ! !. The later is the most terrifying experience, For me it is a cliff face, since I have a cliff phobia that is shocking uncontrollable fear. I have hypo unawareness only during the night, so when I come around from pure adrenaline that allows me a fraction of brain capacity to let me know I am a human, I am not sure if I have been totally unconscious or then coming back to life or still on my way out, I am not even sure how long I have been gone for, 2 minutes or 2 hours? Either way it is totally messed up. The brain without sugar is hell on earth, terrifying, lights, sounds, nightmares, ringing in the ears, the room turns upside down, your voice does not come to call out for help, when it does you sound like a moaning whale. When I am approached everything is in slow motion including their voices, again sounding like a moaning whale. Its not good, in fact it is horrendous. I have needed counseling after a hypo as I struggle for the weeks afterwards not to cry, I’m sure I have PTSD from having nocturnal hypos. I think a medical person assumes you have no recall of what has just happened to you but sorry you do and its not nice and it is mentally disturbing. As soon as your BSL returns to normal they send you home from ER in the middle of the night, in a taxi sobbing, yes send you home a basket mental case from the experience with no counseling or debrief because its assumed you were so unconscious you didn’t feel the experience, sorry…wrong. I am so disturbed by my hypo experiences I cannot watch anything on TV where they depict a mental breakdown scene in the form of cutting in and out of scene like time stops and starts, in reality I have done that while having a hypo. Time stops and starts and reattaches like a scary scene in a move. So to answer your question, I see a H Y P O as a horror movie.
LikeLike
June 29, 2021 at 2:02 pm
Rick Phillips
I see it as a slope. Yes sometimes I fall off a cliff, sometimes, but i mostly slip down the mountain.
Gosh i wish I had known o the summit. I would have loved to be involved.
LikeLiked by 1 person