I’m tired.
Today, I woke in a great mood after a good night’s sleep. The weekend had been relaxing and lovely – family, friends, food and gorgeous weather on top of it all. Plus, I bought a new necklace with a pineapple on it. It was a good couple of days!
I was standing at my favourite café near work, waiting for a takeaway coffee and thinking that the barista was a magician as I watched his choreographed movements, filling takeaway cups with perfectly brewed caffeine.
‘This good day is about to get better,’ I naively thought, the taste of that first sip of coffee so close.
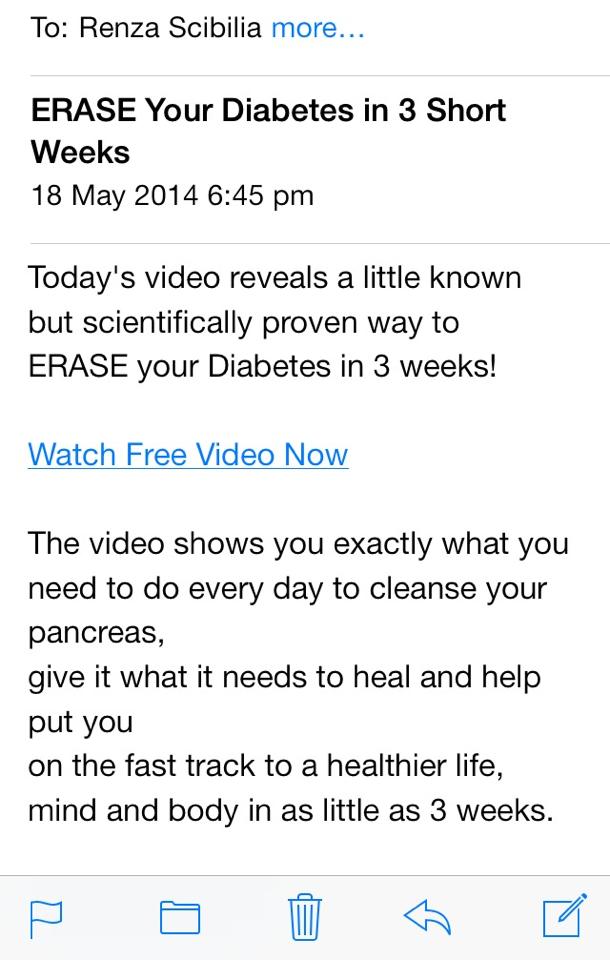
And then, I checked my email and ‘bam’. There it was.
A discussion about not distinguishing between type 1 and type 2 diabetes in a setting where it really is not relevant. I sighed.
And realised how tired I am.
Nearly thirteen years ago, I was employed to run a very small and, at the time, somewhat tokenistic type 1 diabetes program for a diabetes organisation. Thanks to a very supportive CEO and me being a pushy little thing, the program grew and grew and now, incorporates a dedicated team doing some incredibly good work for people living with type 1 diabetes.
One of the reasons for the program’s success is that we have been very clear about defining it as a program for people with type 1 diabetes, making sure the information we provide is targeted and relevant to the people we are trying to reach. We acknowledge each and every day that people with type 1 diabetes have specific information requirements and then we go about providing that information in the way people want.
In exactly the same way, a couple of years ago, we realised that the information for people with type 2 diabetes was completely forgetting the changing face of the type 2 diabetes community. There are more and more younger people being diagnosed with type 2 diabetes and the information we had was very much for an older audience. Hence, Generation T2 – a new program for 18 to 39 year olds with type 2 diabetes.
There are times that it is important to distinguish between the diabetes and there is no louder advocate for that than me.
But there are times that it is irrelevant. Yet, people still get angry – even when it really doesn’t matter if the type of diabetes is defined.
I am tired.
I am over this argument and this discussion.
Last week, the government handed down a budget that is going to hit the hip pockets of people with diabetes like never before. All people with diabetes will be affected – regardless of type.
During the World Diabetes Congress we heard of places around the world where the cost of insulin is so prohibitive that there are people dying because they cannot afford to buy the drug they need to stay alive. Slow, painful, horrible deaths because they cannot afford to buy insulin. Just think about that for a moment.
Here in Australia, there are people who cannot afford to use an insulin pump despite desperately wanting to because they cannot afford private health insurance or qualify for the Insulin Pump Program to assist with cost of purchasing the $9,000 (plus) device.
These are the issues that we should be fighting for and getting angry about. These are the issues that are important. Access to healthcare – a basic human right for all people – ALL people with diabetes – is what the topic should be; not whether or not the Channel 10 news forgot to say type 1 (or 2) before the word diabetes.
I am a card carrying member of the diabetes community. I am proud of this community and I am pleased to have a voice within it.
But we need to stop the finger pointing and the name calling and the blaming. How can we expect people outside of our community to get it right if we can’t? Why is it more important for people to understand the how and why we got this condition as compared with the how and why we’re trying to live and manage with it?
I am proud of the Australian diabetes community, but it is here that I hear this attitude more than anywhere else in the world. This discrimination is not helping us – it is harming us. Does it matter if people don’t really understand the different types of diabetes? I get it. It’s annoying, it’s frustrating; it’s constant. But really; does it matter?
This is a first world – a first class – problem.
And I am tired. I am saying it’s time to stop. Enough!


 I get in my car and there are spent strips, a spare meter and, in the glove box, a tin of jelly beans.
I get in my car and there are spent strips, a spare meter and, in the glove box, a tin of jelly beans.