
You are currently browsing the category archive for the ‘Research’ category.
It’s not an exaggeration when I say that I give thanks to Frederick Banting every single day. I have a photo of him in my office next to an artwork of the word HOPE. And anytime I am sitting at my desk working or sitting in my office reading and find myself looking at the photo, I say these words: ‘Thank you for my life’.
The story of the discovery of insulin has been told many times. There are some excellently researched and detailed accounts of what it took to get to the ‘Eureka!’ moment, as well as documentaries and a couple of feature length movies. But despite having a dozen or so books on my shelf that tell the story, I was so excited to order this version:
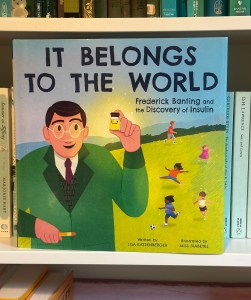
‘It Belongs to the World’ is a gorgeous children’s book by Lisa Katzenberger, and illustrated by the supremely talented Janina Gaudin, (better known online as Miss Diabetes), is a truly beautiful retelling of the story.
While it would make sense to say that this book would make a great gift for a child with diabetes, or parent living with diabetes to read to their kids, really, it’s is a book for everyone. Stories like this should be told over and over, and not just to those of us for whom it is personally relevant. Everyone should learn about the brilliance of scientific discovery. It’s a reminder of the importance of research, and how research saves lives each and every day. It serves to encourage us to get behind research efforts, as a participant or donor if possible. And it gives hope for what still lies ahead.
Oh, and it’s always good to support creators in our community. What a brilliant awareness raising effort from Janina and Lisa. Go get your copy now!
Disclosures
None! I paid for my own copy of this book through my local bookstore. They had to get it in, so you may need to order it. (Or it’s available to order through Amazon.)
So often, there is amazing work being done in the diabetes world that is driven by or involves people with lived experience. Often, this is done in a volunteer capacity – although when we are working with organisations, I hope (and expect) that community members are remunerated for their time and expertise. Of course, there are a lot of organisations also doing some great work – especially those that link closely with people with diabetes through deliberate and meaningful community engagement.
Here are just a few things that involve community members that you can get involved in!
AID access – the time is now!
It’s National Diabetes Week in Australia and if you’ve been following along, you’ll have seen that technology access is very much on the agenda. I’m thrilled that the work I’ve been involved in around AID access (in particular fixing access to insulin pumps in Australia) has gained momentum and put the issue very firmly on the national advocacy agenda, which was one of the aims of the group when we first started working together. Now, we have a Consensus Statement endorsed by community members and all major Australian diabetes organisations, a key recommendation in the recently released Parliamentary Diabetes Inquiry and widening awareness of the issue. But we’re not done – there’s still more to do. Last week I wrote about how now we need the community to continue their involvement and make some noise about the issue. This update provides details of what to do next.
And to quickly show your support, sign the petition here.
Language Matters pregnancy
Earlier this week we saw the launch of a new online survey about the experiences of people with diabetes before, during and after pregnancy, specifically the language and communication used around and to them. Language ALWAYS matters and it doesn’t take much effort to learn from people with diabetes just how much it matters during the especially vulnerable time when pregnancy is on the discussion agenda. And so, this work has been very much powered by community, bringing together lots of people to establish just how people with diabetes can be better supported during this time.
Congratulations to Niki Breslin-Brooker for driving this initiative, and to the team of mainly community members along with HCPs. This has all been done by volunteers, out of hours, in between caring for family, managing work and dealing with diabetes. It’s an honour to work with you all, and a delight to share details of what we’ve been up to!
Have a look at some of the artwork that has been developed to accompany the work. What we know is that it isn’t difficult to make a change that makes a big difference. The phrases you’ll see in the artworks that are being rolled out will be familiar to many people with diabetes. I know I certainly heard most of them back when I was planning for pregnancy – two decades ago. As it turns out, people are still hearing them today. We can, and need to change that!
You can be a part of this important work by filling in this survey which asks for your experiences. It’s for people with diabetes and partners, family members and support people. They survey will be open until the end of September and will inform the next stage of this work – a position statement about language and communication to support people with diabetes.
How do I get involved in research?
One of the things I am frequently asked by PWD is how to learn about and get involved in research studies. Some ideas for Aussies with diabetes: JDRF Australia remains a driving force in type 1 diabetes research across the country, and a quick glance at their website provides a great overview. All trials are neatly located on one page to make it easy to see what’s on the go at the moment and to see if there is anything you can enrol in.
Another great central place to learn about current studies is the Diabetes Technology Research Group website.
ATIC is the Australasian Type 1 Diabetes Immunotherapy Collaboration and is a clinical trials network of adult and paediatric endocrinologists, immunologists, clinical trialists, and members of the T1Dcommunity across Australia and New Zealand, working together to accelerate the development and delivery of immunotherapy treatments for people with type 1 diabetes. More details of current research studies at the centre here.
HypoPAST
HypoPAST stands for Hypoglycaemia Prevention, Awareness of Symptoms and Treatment, and is an innovative online program designed to assist adults with type 1 diabetes in managing their fear of hypoglycaemia. The program focuses on hypoglycaemia prevention, awareness of symptoms, and treatment, offering a comprehensive range of resources, including information, activities, and videos. Study participants access HypoPAST on their computers, tablets, or smartphones.
This study is essential as it harnesses technology to provide practical tools for better diabetes management, addressing a critical need in the diabetes community. By reducing the anxiety associated with hypoglycaemia and improving symptom awareness and treatment strategies, HypoPAST has the potential to enhance the quality of life for individuals with type 1 diabetes.
The study is being conducted by the ACBRD and is currently recruiting participants. It’s almost been fully recruited for, but there are still places. More information here about how to get involved.
Type 1 Screen
Screening for T1D has been very much a focus of scientific conferences this year. At the recent American Diabetes Association Scientific Sessions, screening and information about the stages of T1D were covered in a number of sessions and symposia. Here in Australia. For more details about what’s being done in Australia in this space, check out Type 1 Screen.
And something to read
This article was published in The Lancet earlier in the year, but just sharing here for the first time. The article is about the importance of genuine consumer and community involvement in diabetes care, emphasising the benefits and challenges of ensuring diverse and representative participation to meet the community’s needs effectively.
I spend a lot of time thinking a lot about genuine community involvement in diabetes care and how people with diabetes can contribute to that ‘from the inside’. And by ‘inside’ I mean diabetes organisations, industry, healthcare settings and in research. I may be biased, but I think we add something. I’m grateful that others think that too. But not always. Sometimes, our impact is dismissed or minimised, as are the challenges we face when we act in these roles. I don’t speak for anyone else, but in my own personal instance, I start and end as a person with diabetes. I may work for diabetes organisations, have my own health consultancy, and spend a lot of time volunteering in the diabetes world, but what matters at the end of the day and what never leaves me is that I am a person living with diabetes. And I would expect that is how others would regard me too, or at least would remember that. It’s been somewhat shocking this year to see that some people seem to forget that.
Final thoughts…
Recently when I was in New York at Breakthrough T1D headquarters, I realised just how many people there are in the organisation living with the condition. It’s somewhat confronting – in a good way! – to realise that there are so many people with lived experience working with – very much with – the community. And it’s absolutely delightful to be surrounded by people with diabetes at all levels of the organisation – including the CEO. But you don’t have to have diabetes to work in diabetes. Some of the most impactful people I’ve worked with didn’t live with the condition. But being around people with diabetes as much as possible was important to them. It’s really easy to do when people with diabetes are on staff! I first visited the organisation’s office years ago – long before working with them – to give a talk about language and diabetes. One of the things that stood out for me back then was just how integral lived experience was at that organisation. From the hypo station (clearly put together by PWD who knew they would probably need to use the supplies!) to the conversations with the team, community was in the DNA of the place. As staff, I’ve now visited HQs a few times, and I’ve felt that even more keenly. Walking through the office a couple of weeks ago, I saw this on the desk of one of my colleagues and I couldn’t stop laughing when I saw it. IYKYK – and we completely knew!

DISCLOSURES (So many!)
I was part of the group working on the AID Consensus Statement, and the National AID Access Summit that led to the statement.
I am on the team working on the Language Matters Diabetes and Pregnancy initiative.
I was a co-author on the article, Living between two worlds: lessons for community involvement.
I am an investigator on the HypoPAST study.
My contribution to all these initiatives has been voluntary
I am a representative on the ATIC community group, for which I receive a gift voucher honorarium after attending meetings.
I work for Breakthrough T1D (formerly JDRF).
In a month where there is A LOT of great stuff happening in the diabetes world, stop for a minute and get to know D-Coded, a brilliant new resource which helps to break down diabetes research in an accessible, informative, and authentic manner. It simplifies complex research studies and contextualises information without losing any of the insights and provides people with diabetes a starting point to better understand research, and work out how to delve deeper if we want.

One of the challenges of communicating research is that it can be a lot of detail using specialised language and complex stats and data interpretation. There may be an assumed knowledge that people simply may not have. There are acronyms, jargon, abstract concepts and the details can be lengthy and overly detailed. And that’s if we can see it! Often research papers are behind a paywall, so we can’t event see it in the first place.
Diabetes research is the reason that we are all alive today and it gives us hope for the future. At any one time, the research agenda is advancing to find ways to prevent, cure and treat all types of diabetes in ways that give me so much hope. And so, it makes sense that we should have access to it in a way to keep us engaged and interested and wanting to know more.
One of the tactics I’ve employed over the years is to ask researchers to break down their research into a tweet (280 characters or fewer), or as an elevator pitch. Most find it impossible to do. There is a language to research that can be complex, confusing, and complicated – just as there is a language to lived experience that confounds others. (Don’t believe me? Throw HbA1c, #YDMV, CGM, DIYAPS etc. around and see how people outside our community follow what we’re saying!) D-Coded does that for researchers. Everyone wins here!
It comes as no surprise that this came from the team at Diabesties. Led and powered by Jazz Sethi and involving community, it’s a project that once again shows how lived experience innovation drives change, this time by levelling the knowledge playing field.
Check it out and share as widely as you can.
DISCLOSURE
I am a Lived Experience Advisor on D-Coded. I don’t receive any payment for my involvement and am honoured to have been invited to be part of this project.
Hey, do you remember a couple of weeks ago when it was International Women’s Day and women got a cupcake (probably baked by a woman) and a breakfast (probably organised by a woman) and then we all agreed that gender equality didn’t need to be spoken about for another year?
Look, I know I sound cynical. But that’s only because I am. Every year at Diabetogenic, I write a post celebrating the incredible women working in diabetes. Mostly I centre diabetes advocates who are generally donating their time – and emotional labour – to power advocacy efforts and make change. And if you look back at the history of the DOC, you will see that the majority of the work has been by women in the community. (Don’t @ me with your ‘But I’m a bloke and I’ve done this’ commentary. It’s not the time for #NotAllMen.)
This year, I started to write something, and then stopped, and started again. And then stopped. Anyone who is a frequent visitor to this site or follows any aspects of my personal advocacy knows that I celebrate the incredible work done by grassroots and community advocates (many/most of whom are women) throughout the year and I didn’t want to buy into the ‘It’s-IWD-here-are-the-womens-now-it’s-back-to-the-misogyny-we-usually-deal-with’ crap that seems to be the aftermath of each and every IWD.
So, I’m using today – this random day – to give a shout out to some of the great things going on that you may have seen, or you may have missed. These things are powered by women who, in most cases, are doing this as extra work on the side of their day jobs, and everything going on in their personal lives. But it’s undeniable that it’s this sort of stuff that is going on all the time, usually flying under the radar, but it’s making a difference to so many folks in the diabetes world.
And so…
There is some remarkable work out of India where the Blue Circle Foundation continues to make a mark in diabetes advocacy. On IWD, a team of women from the Foundation conducted an awareness program for 200 women inmates in Yerwada Jail in Pune, India. This is part of their ongoing Project Gaia which creates safe spaces for women with diabetes. Snehal Nandagawli is just one of the women involved in this work. You can hear more from her at this week’s #dedoc° #docday°.

From the UK, Mel Stephenson-Gray has been a brilliant force in the diabetes community for a number of years. She recently launched a fabulous new Insta page celebrating and empowering women with diabetes. It’s called Diabetes Women’s Health Club and the information she’s been sharing (accompanied by gorgeous graphics) is brilliant. I loved the profiles of some of women who were groundbreaking pioneers in diabetes research. Go give the page a follow now!
Dawn Adams hasn’t managed to convince me that she is only one person because the sheer volume of the work she is doing is immense and she’s bloody everywhere. Dawn continues to blaze trails in her research and writings about diabetes and menopause (follow @MenopauseMither on Twitter for great information and support), has been featured in a number of Diabetes UK publications, spoke at the recent #dedoc° symposium at ATTD, and continues to be a daily support and mentor to people across the global diabetes community. I’ve barely scratched the surface with this list. Someone please send Dawn a coffee and cinnamon bun so she can sit down for 30 seconds and recharge her batteries!
Another woman who is a human powerhouse and obviously works 23 hours a day (lazily, she sleeps for an hour) is Jazz Sethi whose work with the Diabesties Foundation continues to multiply exponentially. She’s also a brilliant speaker and gave an emotional talk at ATTD last month. Check out just some of what she is doing here (and stay tuned for something super exciting that we’ve been working on together!)
Also at the recent ATTD #dedoc° symposium, Hamidah Nabakka from the Sonia Nabeta Foundation captivated the packed-to-capacity room, sharing stories of children and young people living with diabetes in Africa. This was held on the first day of ATTD and for the rest of the week, I had people coming up to me and saying that it was their highlight of the whole conference.
I’m getting to this a little late because it was started last year, but Niki Breslin started a brilliant Insta page to build community called ‘My Type of Family’ for anyone with diabetes who is planning and trying to conceive, pregnant, recently had a baby and parenting. There’s lots of great information and encouragement for the community with this page and definitely worth a follow!

I was so excited to see some artwork by Miss Diabetes from New Zealand make it across the ditch Melbourne in an IWD street art exhibition. Her comic ‘Women and Diabetes’ was on show in our city’s iconic Hosier Lane! Miss Diabetes’ diabetes advocacy is super well-known in the community thanks to her tireless efforts supporting Insulin4All efforts and with work she’s done with the WHO diabetes team. You can see the artwork here.
Anita Sabidi in Indonesia continues to drive and build community with her advocacy work that shine very bright lights on issues such as emotional wellbeing and mental health, and women’s health. Anita is a regular speaker about these important topics, and also leads a number of community initiatives supporting women with diabetes in Indonesia. She’s also speaking at #docday° this week.
Dana Lewis never ceases to amaze. Last week she ran 100kms in a day, but unbelievably, it’s not her physical feats that make her name so well known in the diabetes world. It is, of course, her work in open source AID. Last month she gave two presentations at the Open Diabetes Closing Conference, and she has an upcoming session at the ADA Scientific Sessions in San Diego. On top of that, she continues to publish regularly and is a force for nothing but good!
Ashley Ng from Australia has been documenting life with two gorgeous little girls on her blog, opening up about some of the more difficult aspects of parenting while living with diabetes. I love Ash’s candidness and honesty and am always grateful for her ability to be so raw, but also hopeful. Read and subscribe to her blog here.
These women are just a few of the many who continue to make our community tick and flourish. There work is not only meaningful on 8 March: it’s making a difference every, single day. The very idea that women and their achievements get just one day of real celebration (albeit while battling the calls of ‘where’s International Men’s Day?’) is in equal parts frustrating and insulting. I celebrate the incredible work that women spearhead all the time because I know that alongside that work, they are dealing with patriarchal attitudes that make their successes all the more remarkable. That deserves far more than a cupcake!
Postscript
The UN theme for the day was DigitALL: Innovation and technology for gender equality, not the saccharine sweet ‘EmbraceEquity which means absolutely nothing and was created by some corporate machine that does nothing to advance equality in any way. So, if you spent IWD posting selfies of you hugging yourself, that’s great, but what did that really mean when it comes to advancing gender equality?
If you haven’t had a look at the website from the UN, it’s definitely worth it, even if it’s just to see the high-level details, one of which explains that online gender-based violence silences women and discourages their public participation. It may be odd to think this is a thing in the diabetes community when so much of what you see comes from women, but actually, it’s real. Harassment is a concern for many women, and I know of many women who have stopped sharing or locked down their accounts (permanently or temporarily), or deleted them completely, due to this harassment. I’m one of those women. This is something to be mindful of every day – not just a single day in March.
C/W This post contains content about diabetes and suicide and intended self-injury.
If you need help, this Wikipedia page has a list of mental health crisis lines around the world. And for a list of contacts actively updated and maintained by the Wikimedia Foundation, go here.
We talk a lot about taboo topics in diabetes. For years, there have been concerted efforts to shine a light on many of the issues and topics that have not received enough attention but are very important to people with diabetes. Often it is people in the diabetes community who find ways to delicately begin conversations, and that is then followed by an interest from researchers and clinicians.
But there are still some topics that are often seen as just too difficult, just too fraught, just too scary.
Suicide and intended self-injury (ISI) fall into that group.
At EASD this year, I was invited to join a meeting for the RESCUE Collaborative Community, a project that is lifting the veil on one of the most difficult issues in diabetes mental health. The name of this project is a clue to what it is trying to achieve: RESCUE (REducing SuiCide rates amongst individUals with diabetes).
The mission of this project is:
To reduce rates of intended self-injury (ISI) and suicidal acts by people with diabetes through improved understanding of the risk factors and implementing strategies to address them. In support of this mission, RESCUE works with stakeholders across the health spectrum including patients and care partners, academia, healthcare professionals, advocacy groups, industry, payers, federal and state agencies and regulatory bodies.
This is a big issue and a difficult one. There is a lot to think about, a lot of unknowns and a lot of questions to be asked. To work out how to help people with diabetes who are at risk, there needs to be a better informed workforce, with evidence to develop strategies that are going to help. And we also need to know how to approach the very basics when talking about suicide and ISI in relation to diabetes.
When it comes to diabetes and mental health something comes up frequently: there is limited dialogue and understanding between diabetes HCPs and mental health HCPs. I remember hearing Georgie Peters speak at the IDF World Diabetes Congress in 2017 about living with diabulimia. She said that she would be told to ‘go home and take your insulin’ – a completely inadequate approach. In her talk, Georgie said that is the same as telling someone with anorexia to ‘go home and eat’. But when trying to navigate care from two highly specialised health areas, that sort of response is rife.
And so, how to we make sure that when looking at diabetes and suicide and ISI, we are mindful of the specific diabetes issues that need to be considered?
At the meeting last week, we spoke about trying to identify people with diabetes who may need attention. Contemplating how insulin may be used as a way to self-harm is one consideration, so people being admitted to hospital with frequent DKA, and people admitted for a serious hypo could be a starting point to investigate. Of course, not everyone who has DKA or a serious hypo is self-harming. Diabetes gonna diabetes and sometimes, things just happen. But it certainly does seem a good place to begin, with targeted approaches to ask questions in an appropriate way that might help identify people who need mental health support, in particular about ISI and suicide, with an aim of reducing risks.
One of the other discussion points was asking about the role of peer support and the community when talking about suicide and diabetes? Is peer mentorship an idea? How can peers support each other? In the way that #TalkAboutComplications kickstarted meaningful community discussions about the taboo topic of diabetes-related complications and helped people with diabetes feel safe to first open up and speak about their own experiences of living with diabetes-related complications, could there be a way to signpost discussions about serious mental health conditions. And would this break down stigmas, help people realise they are not alone, and seek help, or at least ask where to seek help? Or, is this a burden too big for peer support?
There’s a lot to unpack here, and there really are no simple answers. But this work spearheaded by Professor Kath Barnard-Kelly with a team of dynamic health professionals, with input from diabetes advocates is lifting a veil to start to look for those answers.
MORE
#dedoc° voice, the brilliant Niki (@WhatNikiDidNext) live tweeted a symposium on suicide and ISI at EASD, and you can see her tweets here. Presenters at this session were Kath Barnard-Kelly, Marissa Town, Tadej Battelino and Simon O’Neil.
Disclosure
My travel and accommodation were covered by #dedoc°, where I am employed as Head of Advocacy. Thanks to EASD for the press pass.
I was invited to attend the RESCUE Collaborative Community meeting. I was not paid for my time to attend.
Have you see The Human trial, the documentary film about searching for a cure for type 1 diabetes? I saw it a while ago, and then again last week. It’s remarkable viewing.
I’m delighted to publish this guest post from Elizabeth Snouffer, freelance writer, diabetes advocate and a remarkable woman I’m fortunate to call a friend. Elizabeth wrote this review of The Human Trail just after it was released to US audiences, but I wanted to wait to share it until it could be viewed by people from around the world. Thanks, Elizabeth, for sharing your thoughts.
___________________________________________
The Human Trial documentary film is an intimate look at the overwhelming, messy, and unpredictable nature of living with type 1 diabetes alongside a similarly defined clinical trial seeking to fund and find a cure for the disease. Directors, Lisa Hepner and Guy Mossman, have painstakingly worked on their documentary film for more than a decade as Producer and Writer, and Director of Photography respectively. Abramorama released the film in theaters on June 24, 2022.
Diagnosed with type 1 diabetes at age 21, Hepner, who narrates the film, represents millions of people in the diabetes community – including families, physicians, advocates and more – who would do anything to put an end to the auto-immune condition that leads to terrible complications and early mortality.
Mossman calls his documentary an observational film and it is hard to disagree. The cinéma vérité approach allows the audience to experience the relentless burden diabetes exacts on the people it touches. In the first scene, we watch Hepner prick her finger for blood while her 3-year-old son Jack looks after the test strip in the glucose meter. He is excited but turns quiet while we observe the countdown and Jack tells his mom the result—2-9-4. Hepner brushes off her disappointment and Jack quickly moves on asking Dad to test his glucose. Mossman complies with the child’s request, but the result, 96 mg/dL is startling. The health gap between Jack’s parents is a poignant reminder of the difficult impact disease has on a family. “I’ve spent the last 30 years trying to outrun diabetes, but it’s not working,” says Hepner as she prepares for an appointment with her nurse practitioner, expressing hope to stave off retinopathy and blindness. Without adequate care for blood glucose stability, what will tomorrow bring for this young family? When the well-meaning public questions prioritizing a diabetes cure because insulin is often misrepresented as the answer, The Human Trial offers a strong rationale for funding diabetes cure research.
The film is always on the move, symbolic of the stamina it takes to both manage a chronic illness and fight for cures. From her car, Hepner asks “Why is the cure for diabetes taking so long?” and we wonder, too. Viacyte, a California Bio-tech company, gives Hepner and Mossman real-time access to film various aspects of their first clinical trial – only the sixth-ever embryonic stem cell trial in the world. It’s clear the film has moved away from the personal sphere into medical science and in a sense, the business of diabetes. We become onlookers to an employee filled conference room celebration and listen to former Viacyte CEO, Paul Laikind, announce FDA approval for the biotech’s first human clinical trial with a bio-artificial pancreas. We feel the impact of their excitement and anxiety. Will our methods work? Will we run out of money?
Trials take place across the world but Hepner and Mossman’s camera lands at the University of Minnesota where the first participants, who are high risk for acute life-threatening complications, are implanted with multiple small-format cell-filled devices called sentinels to evaluate safety and viability. Maren, aka Patient 1, suffers from hypoglycemic unawareness and seizures, and Gregory, Patient 2, is concerned about vision loss. Their ability to deal with adversity is uncanny, and their fortitude as pioneers on a surgical journey to the unknown is inspiring to watch. We observe the operating room from above as Maren and Gregory are implanted and witness the risks associated with the new therapeutic approach. They have similar questions to the Viacyte team, but the stakes are higher.
Could I be cured?
Participants in clinical trials aren’t usually given any indication of outcomes before trial completion which is understandably excruciating for Maren and Gregory during the trial. The countless surgeries and tests are grueling, and we are gripped by their resilience on the screen and our mutual desire for a positive outcome.
The Human Trial gives visibility to the invisible—the often-hidden and challenged lives of people with type 1 diabetes and the thousands of scientists and researchers working arduously to fund and discover cures. The film’s subjects are not just fighters; they have accepted how obstacles, even failures, are a part of the journey to success. I call that courage.
Please click here to see where you can watch.
Elizabeth Snouffer is a freelance writer living in New York City.
Psst…forgotten something?
If you’re in the northern hemisphere right now, you’re possibly all caught up in the sunshine, splashing around at the beach or spending time off work just taking time out. If you’re from the southern hemisphere, you’re either smart and have taken a holiday to Europe because EVERYONE.IS.IN.EUROPE.RIGHT.NOW, or under fifteen quilts in front of a roaring fire, counting down the days until it gets warmer. Sadly, I’m in the latter group.
I get it. Things slip by either way.
But! You only have a few days left to make sure you don’t miss out on applying for a #dedoc° voices scholarship. Wherever you are, a scholarship means you have something to look forward to in a couple of months’ time and the absolute thrill of either virtually or in-person attending a global diabetes conference or two. That’s right – TWO! EASD (European diabetes conference) and ISPAD (paediatric diabetes conference) are the next international conferences on the diabetes conference calendar. Both will be hybrid, with the in-person locations being Stockholm and Abu Dhabi respectively.
We’re well over two years into the #dedoc° voices program now, and the awesome thing about it is that it’s not just about the few days of the conference where you get to learn from incredible researchers and clinicians, while waving the lived experience flag and being surrounded by others with diabetes. I mean, that is all pretty great. But being a #dedoc° voice goes way beyond that! Once you receive a scholarship you are part of a network of remarkable diabetes advocates from across the world, and this network is the most supportive, encouraging, brilliant group of people, always ready to help. Every single week, I see people reaching out for support and advice and the responses are swift and many. I’ve not seen a single example of anything other than support, and have watched advocates truly flourish as they have worked with others, developed mentoring relationships and been supported to do brilliant things.
Unless you’re part of the program, you wouldn’t know this. And here’s the deal: anyone can become part of it. The #dedoc° voices program is open to people from across the world and everyone is in with an equal chance. You just need to spend some time completing an application. It is a competitive process, and places are limited. The people who get accepted are the ones who have taken some time with their application and really been able to demonstrate just how they are going to #PayItForward to their diabetes community if successful. No one is a shoe in; having a high follower count on socials means nothing if your application is sub-par. We take people who are new to the diabetes advocacy space, and are looking for a hand carving out their space, as well as seasoned advocates who are keen to work with others and become part of a global network, outside their own country.
So, get on it! Click on the image below, fill in the form and join us! You get to work on your advocacy while giving back to the community, all while wearing the #NothingAboutUsWithoutUs badge. How amazing is that?!

More on #diabetogenic about the #dedoc° voices program:
#dedoc° voices helping people with diabetes get into professional conferences
How #dedoc° voices supported people with diabetes in Ukraine
More on why to apply to join the #dedoc voices program
Disclosure
I have been an advisor for a number of years, and am now working with them as Head of Advocacy.
Gosh, it’s been a hot minute since I last did one of these. The whole point of Interweb Jumble posts on Diabetogenic is to highlight anything that has caught my interest in the online diabetes world, write about initiatives I’ve been involved in, and, most importantly, to elevate the great work being done by others living with diabetes. Building folks up and promoting their amazing efforts has been at the heart of what I do, so I’m always happy to share what others are doing.
Grab a coffee, tea or shandy, (Don’t. Don’t grab a shandy), and read on.
Diabetes Chat
YES!! There is a new place to congregate online, in a different format, and with this one, you get to hear people’s voices. (Sorry to everyone who had to endure my 7am Aussie accent last Tuesday!). This is a new initiative that’s been set up by three DOC folks – Tom from the UK, and Chris and Sarah from the US, utilising a new feature on Twitter called Spaces. It’s a terrific way to host an online peer meeting, creating yet another time and place that is BY people with diabetes, FOR people with diabetes. There is a weekly guest who gets put through their paces with terrific questions from the hosts and those listening in, and an open mic chat time as well.
It’s super impressive to see people from all over the globe participating. It reminds me a little of the DSMA tweetchats which are very welcoming and open to all, regardless of where you live around the world.
Search #DiabetesChat on Twitter for more.
dStigmatize
The team at diaTribe has once again tapped into one of the important issues, and much spoken about topics in the diabetes community and developed a terrific new website addressing diabetes stigma. It’s called dStigmatize and you can find it here.
I’m delighted to see Diabetes Australia’s work on stigma and language highlighted so prominently on the site (disclosure: I work at Diabetes Australia and have been involved in this work), including the videos from last year’s Australian National Diabetes Week campaign, which have been viewed hundreds of thousands of times.

Seasons of…diagnosis
New research out of Finland asked if more people were diagnosed with type 1 diabetes during colder months. You can read the paper here.
And a discussion on Twitter about it here.
HypoRESOLVE podcast
The HypoRESOLVE comms team created a new podcast to showcase the incredible work of this researchers involved in the project, with a strong emphasis on how people with diabetes are involved in the project. I was delighted to host this podcast and speak with some truly remarkable clinicians and researchers as well as other people with diabetes who are on the projects Patient Advisory Committee. (Disclosure – I am on the HypoRESOLVE PAC. PAC members are now paid an honorarium for our time working on this project, however we were not at the time of recording or working on this podcast.)
Here is the most recent episode (on Spotify).
Better engagement with PWD = better services
Great paper from a team out of the UK looking at how connecting with the lived experience expertise of people with diabetes, health professionals and diabetes health services can improve service delivery.
One of the co-authors is one of the GBdoc OG, Laura (@Ninjabetic1 on Twitter), and it’s great to see her name back in the diabetes world, contributing to this important discussion.
And the DDA podcast…
The Danish Diabetes Academy developed a podcast out of their Winter School that featured Postdocs who had participated in the academy speaking with others in the diabetes world to discuss who academic researchers work to ensure their research reaches and benefits those they are researching. I was so honoured to be invited to be interviewed for their first episode and answered questions about how communication is important when engaging people with diabetes to be part of the research process. You can listen here.
Language Matters for Portuguese speaking friends with diabetes!
The latest in the Diabetes #LanguageMatters stable is this document out of Brazil. Always terrific to see more and more statements coming out, highlighting the importance of language and communication in diabetes.
Thinking of starting on an insulin pump?
If so, the awesome Grainne at Blood Sugar Trampoline has you covered with this post. It is truly one of the most measured pieces I’ve read about things to consider if you are on the path to starting an insulin pump. The gushiness and superlatives that many of us resort to when banging on about how much we love our pumps are replaced with sensible, and practical advice and suggestions. If this is where you’re thinking of taking your diabetes management, Grainne’s piece is a must read.
Who doesn’t want to come to ATTD!?
#dedoc° voices is back and heading to ATTD in April this year, and applications are still open if you would like to be considered as part of the program. Successful applicants will be granted access to the entire ATTD program, giving them an opportunity to share what they see and learn with their networks. Make your submission count – this is a competitive process and success is more likely for those who take the time to provide details of how they will be involved in the program. Details here.
(Disclosure: I am an advisor to the #dedoc° voices program. I do not receive any payment for this role.)

World Health Organisation
In March, the World Health Organisation, through the Global Diabetes Compact, is hosting a two-day focus group for people with lived experience of diabetes. If you’re interested in getting involved, there is an expression of interest process you can complete here.
Also from WHO is this survey which is asking people with diabetes how to improve messaging and communication. You only have until 28 Feb, so get onto it now! (Disclosure: I was a volunteer consultant in the development of this survey)
Massive kudos to the Global Diabetes Compact team who are doing an absolutely stellar job engaging with the community. Always so terrific to see!
A diabetes sea shanty…
You’re welcome.
(Follow @TypeWonDiabetes on Instagram here.)
People with diabetes and their involvement in research
An end of year delight was this article that I co-authored making it to publication. The article is about how to better involve people with health conditions in research (which really seems to be something I’ve been very focussed on recently!).
Spare a Rose – last push
February still has a last few days which means that Spare a Rose isn’t over yet. You can still donate and contribute to this year’s total and support people with diabetes in under-resourced countries through the Insulin for Life program.

Seventeen years ago, I had a decision to make. Would I enrol our soon-to-be-born baby in research that would tell us if she had any of the antibodies for type 1 diabetes?
I thought about it long and hard. Aaron and I spoke about it a lot. He wanted to support me with whatever I thought would be best. In the end, we decided not to do it. Even before our daughter was born there was a dread that I could barely give word to – I was terrified that I would be responsible for passing on my diabetes to my baby. That feeling hasn’t gone, by the way. I have spent a lot of hours working through it with a psychologist to try to understand the source of the anxiety and learn to manage the fear in a way that doesn’t become all encompassing. Because there were times that I felt paralysed with that fear. I knew I needed to get through that.
I felt horribly guilty about not signing her up straight away and registering her in research. When I returned to work after maternity leave, there was a trial that was in full recruitment mode, and I once again faced the decision. I was actively promoting this study through my work, and speaking to the researchers a lot. A couple of times, I asked if I could speak with them in a personal rather than professional capacity and explain my reticence to enrol my daughter, even though I could understand why the work was so important. I asked for their advice and guidance, and they were always so wonderfully kind and understanding when I said that I simply didn’t feel that I could proceed. I think that part of the reason was that there wasn’t really all that much that could be done if it was identified that she did indeed have one or more of the islet autoantibodies.
Over the last couple of years, there has been a lot of interest and excitement in research into prevention and delay of type 1 diabetes. That ‘p’ word that has only ever been attached to type 2 diabetes now very firmly has a place when it comes to type 1 diabetes. At the ADC earlier this month, I listened to a couple of hours of talks from researchers who were talking all about screening for type 1 diabetes, and interventions that are taking place around the world with remarkable results.
The Type 1 Screen program has been running in Australia since 2018. It is open to relatives of someone with type 1 diabetes, aged 2 – 30 years. After initial screening, people without antibodies are screened every five years; people with antibodies are screened annually. Up until now, screening has been by doing a pathology blood test. However, home collection is being developed and, at the time of the presentation, was about to be launched. Home collection will be done by using blood from a finger prick.
So, what are the benefits of screening for type 1 diabetes? Well, there are many!
Early diagnosis (of anything) is a good thing! In a perfect world, early diagnosis means early treatment which means better outcomes. It also helps people and families prepare for progression to diabetes.
Screening reduces the risk of DKA at diagnosis. While that may make for a less traumatic diagnosis experience, there are also linger term benefits for this. DKA at diagnosis increases the risk of recurrent DKA, a higher A1c and increases the risk of diabetes-related complications.
Prevention is on the horizon! Knowing people who are at risk of type 1 diabetes means employing interventions that have the potential to delay, and may one day prevent, type 1 diabetes. Research using the drug Teplizumab delayed the onset of type 1 diabetes by two years.
Researchers and clinicians are talking about stages of type 1 diabetes and this is where it gets super interesting. Stage three type 1 diabetes I diagnosis and, typically, that’s where treatment starts. But in the future, it’s possible that treatment, including glucose monitoring, could be routine for stages one and two.
I listened to all this carefully and one thing that was clear to me: even seventeen years later, the emotional impact of this is significant. Thankfully, Dr Christel Hendrieckxs from the ACBRD is part of the project team for this work here in Australia. It goes without saying that this is about a lot more than just early diagnosis of type 1 diabetes. There is also the impact on the family, especially if someone in that family already has type 1 diabetes. The mother guilt I have at the thought of passing on diabetes to my daughter is by no means a small thing. I know a number of other parents with diabetes who have similar thoughts.
After that session, I asked my sixteen, almost seventeen, year old how she would feel about enrolling in Type 1 Screen. It’s completely up to her now – I am happy to chat about it, and tell her all about the program, but ultimately, it’s her decision. She understands why I was reluctant to enrol her when she was tiny, but now, I am giving her the option to get involved, and she needs to make her own decision which we’ll fully support. I don’t know what she will decide, but the seed has been planted, and I am here to chat with her about it, and organise times to meet with the researchers too if she’d like.
Watch my Q&A with A/Professor John Wentworth from Type 1 Screen about getting involved in this research.
Yesterday, the Australian vaccine rollout was expanded to include children. This follows the TGA approving the use of the Pfizer COVID-19 vaccine for children in the 12 – 15 year age group. ATAGI responded by including children with diabetes in that age group into Phase 1B, meaning they are eligible right now for a jab (provided, of course, they can find one…!).
Already I’m seeing in diabetes online discussions some parents of kids with type 1 diabetes saying their child will not be getting the vaccine, stating that the reason for that decision is because their type 1 diagnosis came shortly after one of their childhood vaccines.
And so it seems a good time to revisit this post that I wrote back in 2017. It has a very long title that could have been much more simply: correlation ≠ causation.
It is understandable to want to find a reason for a health issue. Being able to blame something means that we can, perhaps, stop blaming ourselves. I imagine that for parents kids with diabetes that desire to find something – anything – to point to would come as somewhat of a relief. But there is absolutely no evidence to suggest that vaccines are that reason.
Unfortunately, the idea that vaccines are the root of all evil and cause everything under the sun is a myth that is perpetuated over and over in antivax groups; groups where science, evidence and logic goes to die. Vaccines save lives and they are safe. Anyone who says otherwise is lying.
My sixteen year old is not in a priority group and cannot be vaccinated just yet, but she is ready to go as soon as her phase has the green light. All the adults nearest and dearest to her – her parents, grandparents, aunts and uncle, friends’ parents – are fully vaccinated now, and she knows what a privilege it is to be in that situation. She understands that with that privilege comes responsibility to do what you can to protect vulnerable cohorts in the community. And she also understands that vaccines are safe and they save lives.
If you are feeling unsure about getting a COVID vaccine – for you or your child – please speak with your GP. Don’t listen to someone in a Facebook group. And that may come as a surprise to anyone who knows how important I consider peer support and learning from others in our community, but to them I say this: I listen to and learn from people in the diabetes community because they don’t suggest anti-science approaches. They talk about support, and provide tips and tricks for living with diabetes. If anyone tells me to ignore doctors (because all they care about is getting rich), or to stop taking my insulin (because there is a natural supplement that will do the trick), I would block them as quickly as I could. Science works. Science is why people with diabetes are alive today. Science is why we have vaccines. Trust science. THAT’S what makes sense.
__________________________________________________________________________
In the next couple of weeks, our kid gets to line up for her next round of immunisations. At twelve years of age, that means that she can look forward to chickenpox and Diphtheria-Tetanus-Pertussis boosters, and a three-dose course of the HPV vaccine.
When the consent form was sent home, she begrudgingly pulled it out of her school bag and handed it to me. ‘I have to be immunised,’ she said employing the same facial expressions reserved for Brussels sprouts.
She took one look at me and then, slightly sheepishly, said, ‘I don’t get to complain about it, do I?’
‘Nope,’ I said to her. ‘You don’t get to complain about needles because…well because…suck it up princess. No sympathy about needles from your mean mamma! And you have to be vaccinated because that’s what we do. Immunisation is safe and is a really good way to stop the spread of infectious diseases that not too long ago people died from. And herd immunity only works if…’
‘….if most people are immunised so diseases are not spread,’ she cut me off, finishing my sentence. I nodded at her proudly, signed the form and handed it back to her. ‘In your bag. Be grateful that you are being vaccinated. It’s a gift.’ (She mumbled something about it being a crappy gift, and that it would be better if she got a Readings gift voucher instead, but I ignored that.)
Over the weekend, the vaccination debate was fired up again with One Nationidiot leader, Pauline Hanson, sharing her half-brained thoughts on the issue.
I hate that I am even writing about Pauling Hanson. I despise what she stands for. Her unenlightened, racist, xenophobic, mean, ill-informed rhetoric, which is somehow interpreted as ‘she just says what many of us are thinking’, is disgusting. But her latest remarks go to show, once again, what an ignorant and dangerous fool she is.
Her comments coincided with a discussion on a type 1 diabetes Facebook page about vaccinations preceding T1D. Thankfully, smart people reminded anyone suggesting that their diabetes was a direct result of a recent vaccination that correlation does not equal causation.
I get really anxious when there is discussion about vaccinations, because the idea that this is something that can and should be debated is dangerous. There is no evidence to suggest that vaccines cause diabetes (or autism or anything else). There is, however, a lot of evidence to show that they do a shed-load of good. And if you don’t believe me, ask yourself how many cases of polio you’ve seen lately. People of my parents’ generation seemed to all know kids and adults with polio and talk about just how debilitating a condition it was. And they know first-hand of children who died of diseases such as measles or whooping cough.
This is not an ‘I have my opinion, you have yours. Let’s agree to disagree’ issue. It is, in fact, very black and white.
A number of people in the Facebook conversation commented that their (or their child’s) diagnosis coincided with a recent vaccination. But here’s the thing: type 1 diabetes doesn’t just happen. We know that it is a long and slow process.

What this shows is that even if onset of diabetes occurs at (correlates with) the time of a vaccination, it cannot possibly be the cause.
When we have people in the public sphere coming out and saying irresponsible things about vaccinations, it is damaging. People will listen to Pauline Hanson rather than listen to a doctor or a researcher with decades of experience, mountains of evidence and bucket-loads (technical term) of science to support their position.
The idea that ‘everyone should do their own research’ is flawed because there is far too much pseudo-science rubbish out there and sometimes it’s hard to work out what is a relevant and respectable source and what is gobbledygook (highly technical term).
Plus, those trying to refute the benefit of vaccinations employ the age-old tactic of conspiracy theories to have people who are not particularly well informed to start to question real experts. If you have ever heard anyone suggesting: government is in the pockets of Big Pharma / the aliens are controlling us / if we just ate well and danced in the sunshine / any other hare-brained suggestion, run – don’t walk – away from them. And don’t look back.
I have been thinking about this a lot in the last couple of days. I have what I describe as an irrational fear that my kid is going to develop diabetes. It keeps me awake at night, makes me burst into tears at time and scares me like nothing else. If I, for a second, thought for just a tiny second that vaccinating my daughter increased her chances of developing diabetes, she would be unvaccinated. If I thought there was any truth at all in the rubbish that vaccines cause diabetes, I wouldn’t have let her anywhere near a vaccination needle.
But there is no evidence to support that. None at all.






