
You are currently browsing the category archive for the ‘Diabetes’ category.
If you’re on social media, you’ll be more than familiar with the ridiculous clickbait style articles that tell you about ‘things you should know’. These lists are often targeted to specific age groups (20 things all women in their twenties should know), gender (5 things men should do on a date) or include things to make you feel like you’re falling behind (23 things your daughter should know by the times she’s 13 years – subtext: and if she doesn’t, you’re a lousy parent).
The aim of these articles is to make the reader feel inadequate and feel that they are failing at things because they are 34 years old and haven’t worked out the 10 things every woman should know about orgasms.
I steer clear of any of these lists and simply don’t give in to the desire to click. So, here’s my list of 16 things every person with diabetes should know:
- Diabetes sucks.
- Diabetes can also be interesting and eye opening.
- Finding a healthcare professional who understands you and what you need will make navigating the system easier. And it’s perfectly okay if you want someone to ‘tell you what to do’ rather than someone who is more consultative. Horses for courses.
- Cinnamon doesn’t cure diabetes and anyone who says it does is a big lying liar. And possibly a bit simple.
- There is no unsuitable response to the question ‘should you be eating that’. Gentle violence is acceptable, as are tongue lashings, death stares and bursting into tears.
- Further to number 5 – yes, you can eat that.
- Cupcakes with sprinkles make as suitable a lunch for a person with diabetes as a person without diabetes.
- It’s perfectly okay to squeal when you see another person pulling out an insulin pump, giving themselves a shot of insulin, or checking their BGL. Even if you don’t know them.
- You do not need to explain your diabetes to anyone. That includes how you choose to manage it, how you feel about it, what you say about it. Your diabetes; your rules.
- I’ll just say that again: Your diabetes; your rules.
- There is no room for judgement. From anyone about anyone. (Except for people who wear leggings as pants. I’m all for judging them. And the Kardashians.)
- Unicorns are real – I rode mine to work this morning.
- Feeling sad or happy or down or ecstatic or miserable or pissed off about diabetes are all reasonable emotions – even within the same five minute period.
- It’s okay to grieve. Life with diabetes is different.
- There is no substitute for a friend with diabetes saying ‘I get it’.
- Lists about diabetes are stupid
What if diabetes ruins my life?
Is it line-change day?
What if I have passed on my diabetes to my beautiful daughter?
When is my next endo appointment?
What if I have a heart attack or stroke?
Should I check my BGL?
What if I have a hypo in my sleep and don’t wake up?
Did I bolus for lunch?
What if I pass out while driving and run off the road?
Am I hypo?
Again?
What if I can’t do the things I love?
Why is my BGL 29.9mmol/l?
What if I develop diabetes complications?
Where’s my freaking meter?
What if I can’t look after myself anymore?
What if my kidneys fail?
What if…?
What if it’s all okay?
An article appeared in The Conversation last week about how the food industry gets us to buy and eat ‘nutritionally worthless’ foods and drinks. The thing I found most interesting about the piece was when the authors were talking about number of choices we have today when we take a walk down a supermarket aisle as compared with in the 1960s.
Today, supermarkets stock about 30,000 items. That’s a lot of breakfast cereal or yogurt from which to choose. By comparison, anyone doing a weekly shop in the 1960s had between 600 and 800 items on the shelves.
One of the things we complain about in Australia is that we have limited choice when it comes to diabetes devices and management options. This is true when we compare what is available here with the options of those in the USA and Europe. I have seen and held and played with all sorts of devices that I would love to be able to use, but they are not available on our fair shores – and not likely to be launched here either. ‘Market is too small’ is the reason given all the time.
I like choice and as a consumer advocate, I am the first to say that all the options for management of our diabetes should be before us before we make a decision as to what we will use. It frustrates me that I cannot choose to use a T-Slim pump or the OmniPod system.
I’m not sure exactly how many BGL meters are available in Australia, but I know it’s certainly not as many as at any Walmart I’ve popped into when travelling in the US. I’m always astounded at the ‘diabetes aisle’ in these stores.
Do we want that sort of choice when it comes to diabetes management tools? I’m not sure. I guess I like the idea of being able to choose the device best-suited to me. Do I think that we need a choice of two hundred thousand (slight exaggeration) BGL meters that do pretty much the same thing? Maybe not. I actually do think that we have a good selection here from which to choose and don’t really feel we’re missing out.
But it’s a different matter with pumps. There are not really that many pumps on the market to begin with. We have a choice of only four or five here. We don’t have the option of a tubeless pump, which is definitely a point of difference, nor a touch screen pump.
Some may say we shouldn’t complain – that a pump is an insulin delivery device and as long as it does that, everything else is just fancy-pants add-ons that mean nothing.
But surely that same argument can be applied to everything. We don’t need choice in the cars we drive – a car gets us from point A to B – leather seats and auto windscreen wipers are superfluous. Or a phone is a device to call people and chat – cameras, calculators and other applications are unnecessary and bonus extras.
We wouldn’t accept that. We SHOULDN’T accept that.
For me, when it is time to consider a new pump or CGM or BGL meter, the things that are the most important are safety and accuracy. But I do want to be able to line up all the options, look at their particular features and then make an informed decision. It’s my right to choose.
‘Which five albums would you want with you on a desert island?’
Putting aside issues of how to play the albums (I’ve not watched enough Gilligan’s Island to work out how to fashion a coconut, palm frond and pile of sand into a sustainable electricity source), it’s fun (and hard!) to think of the five albums I’d want to listen to repeatedly until rescued by Captain Jack Sparrow.
It’s just as fun to decide the five movies or five books I’d choose. (At least with the books, electricity is not needed.)
But what about the five diabetes things I’d want with me if I found myself stranded?
Disaster management when it comes to diabetes is something that I have stored in the to-do list at the back of my mind along with sorting out my Will and cleaning out the third drawer in the kitchen. I know I should do them, but really, really, really don’t want to. I’ll get around to it eventually.
I also think that given my personal situation – inner-city living, five minutes from the nearest tertiary hospital, know heaps of people I can call on if all my diabetes supplies get eaten by a wild animal etc. etc. it’s not likely that I am going to need to set my disaster plan in action any time soon. But never say never, right?
The only time I really think about it is when I am travelling and there is a (tiny) chance I could lose all diabetes supplies on me and be somewhat stranded without the support and emergency back-up I’m used to. When I travel, I over-pack for any situation. I take two spare pumps, enough diabetes supplies to last at least twice the time I’ll be away and make sure that everything is packed in a bag that is never out of my sight.
But…what if?
Well, for the sake of the diabetes desert island play list game, I think it would be the following:
Insulin – obviously. Lots of it. And some way to deliver it. While I am very attached to my pump (literally as well as figuratively), for the sake of this exercise, I’m going to say that I’ll use syringes to deliver said insulin. That way, no need to worry about batteries, pump failures, infusion sets, reservoirs etc. etc. I’d also want a BGL meter with a very long-life battery and lots of strips. Of course I’d need lancets. Ha-ha-ha-ha. Just kidding. I’m assuming it’s going to be hot on the desert island, and warm weather always results in lows, so I’ll need enough jelly beans to see me through until I find another source of glucose (hoping there will be a plantation of delicious berries somewhere). And finally, a Nutella tree. Just because.
Whilst I doubt (hope?) I’ll never be stranded on a desert island, this exercise reminds me once again that diabetes adds that extra layer to thinking about how to manage different circumstances. But I think my list is sorted. I am now going to spend some time watching Gilligan’s Island to really prepare myself.
Friday tunes. This would definitely be on my playlist. Because even if stuck on a desert island, I’d still want to listen to Tom Waits.
‘You have brittle diabetes,’ the diabetes educator told me, regret in her voice.
Brittle. It’s such a sharp sounding word – all edges to cut yourself upon.
I first heard the term ‘brittle diabetes’ about three years after I was diagnosed. It was handed to me as a grave diagnosis within a diagnosis. Not just diabetes for me. I had brittle diabetes. I heard it, thought about it, said the words a few time together, jarring at the sound.
I was given this ‘diagnosis’ during a really rough period. My diabetes was all over the place thanks to a totally unrelated stomach issue. There were thoughts it may have been gastroparesis or, for a moment there, thanks to the significant weight loss I was experiencing, an eating disorder.
I became terrified to eat because every time I did, I was in extreme pain. At times I threw up everything I ate, other times I didn’t. My blood sugars were all over the place and the delightful insulin regimen which at the time involved Protophane was incredibly hopeless at doing anything other than send me plummeting low, or sky-rocketing high. It was a very tough few months.
I was seeing doctor after doctor after doctor. And all anyone could think about was my diabetes. My brittle diabetes. I was told: ‘This is what your diabetes is like. Sometimes there are no answers and we can do nothing to better manage things. This is it for you.’ There was an undertone of ‘get used to it, love’.
I wasn’t prepared to just accept it though. I wanted to have a baby and I knew that there was no way that I could even consider going down that path while my health was all over the place.
I finally sacked all the health professionals I was working with and sought out someone – something – else. I refused to believe that this was how I was going to be forever. I knew there were answers; I just didn’t know how to find them.
I found a new endo and when I walked in I told her that I had brittle diabetes. ‘I can’t be fixed, apparently. Give me everything you’ve got!’ I thought silently.
‘I don’t like that term,’ she told me gently. She wasn’t rude about it; she just explained that she thought we could work out why things weren’t going so well. And then, she went about finding answers. And we found them.
It took time and it took a lot of thinking outside of the square. It took putting diabetes to the side and not thinking that it was the only reason for all my health problems. Once I got sorted and my stomach was sorted and I spent some time talking things through, my diabetes was much easier to manage. I know that a big part of getting through was not only addressing the physical side of things. There were mental health issues I needed to address, mostly dealing with the grief I was experiencing about having to let go of my life before diabetes.
I too came to not like the term ‘brittle diabetes’. When I hear it now, I want to ask what else is going on. And I can’t help wonder where I would be now if I had just accepted that as my lot in diabetes.
Want more? Mike Hoskins wrote this interesting post on Diabetes Mine last year.
So much going on. So much to do. So much to plan. So many presentations to write.
So….naturally, I’m surfing!
BIONIC
I’m still really excited about the Bionic Pancreas. I know that when we hear of new research it’s often about mice, labs, five years’ time etc. So hearing and reading about the ‘real-life’ applications of this technology has been so very exciting. And hopeful. I interviewed someone who participated in the Melbourne trials (you can read about it in the next edition of Conquest). And for another beautiful, goose bump-inducing read about it, here’s what Kerri wrote at Six Until Me.
BLUE CIRLCE APP
A couple of months ago, the IDF launched a new photo app to help raise awareness of diabetes. You can add a blue circle to any photo and then share on social media. Here’s my latest masterpiece:
ZOE BOWIE SINGS
Earlier this year, I sat on a Google Hangout panel with Jamie Tripp Utitis who recently presented at the Doctors 2.0 and You conference in Paris about her beautiful new book ‘Zoe Bowie Sings, Despite All Sad Things’. Jamie wrote this book for kids with a parent with MS. Jamie writes an awesome blog of her life with MS. You can read it here.
WHERE ARE THE PEOPLE?
I threw a huge tantrum let out a huge sigh of defeat when this appeared in my (virtual and real) inbox today. It’s the promotion of a conference in Melbourne later this year about the future of primary care. One of the focuses is patient outcomes. Looking through the myriad speakers what do I find? Not. A. Single. Patient. In. Sight.
SCRIBBLES
Mike Lawson (who I was lucky enough to meet briefly at year’s ADA conference) recently started ‘Scribbling My Life Away’, a blog of his drawings. It’s not really, diabetes-related (although there is the occasional diabetes reference) but nonetheless very cool. (And, Mike, if you’re reading this, can you please do me a scribble of a jar of Nutella and a big spoon. I’d like to put it up in my office?)
SWEET PRETTY THINGS
Totally, completely and utterly not diabetes-related, but I can’t stop looking at the gorgeous artwork of Aussie Illustrator Kerri Hess. I am trying to work out how I could commission a life-size piece that would fit perfectly on a big blank wall in our bedroom.
MEOW
In other news, a cat café opened in Melbourne this week.
CRAZY BIKE RIDING TYPE 1 PEOPLE HEADING TO VIENNA
Last year a group of mad folk with type 1 diabetes rode from Brussels to Barcelona as part of the mHealth Grand Tour. Not content with this achievement, the group known as Team BG, will be doing it all again, kicking off in Barcelona and heading to the location of this year’s EASD conference, Vienna, where I intend to greet them and call them all crazy. I might then buy them a beer.
HAVE YOU REGISTERED YET?
A reminder that TODAY IS THE LAST DAY to get the early bird rate to attend the first ever ADS-ADEA Consumer Outreach program. Book now!
This post was first published in 2011. Sometimes, I think that there is progress being made when it comes to consulting people with diabetes in the development of programs, services and resources for us. Other times, I’m not so sure. Some groups and organisations are incredibly tuned in to people with diabetes (I’m talking about you, Australian Centre for Behavioural Research in Diabetes) and I cannot express enough my gratitude for the high regard of the ideas and thoughts of people with diabetes this group regularly demonstrates.
I stand by what I have written in this post: We are the experts in living with diabetes and we want to work with those who are working to help us. Please, please let us.
——————————
There seem to be a lot of people who like to be the voice of people living with diabetes. Strangely enough, a lot of the time, these voices don’t actually have diabetes themselves.
As far as I am concerned, every single person out there who wants to advocate and support people living with diabetes is terrific. Continue doing it! But make sure that if you are speaking for us you have first heard what we want to say.
Any time an advisory panel or steering committee looking at anything to do with people living with diabetes is formed, the first people invited should be consumers. How can other people possibly advise or steer for us unless they hear what we need and what we want?
If government wants to improve our lot, ask us how to do it.
Experts in diabetes are not the people who care for us. I know how blunt and arrogant that sounds, but it’s true. I have a brilliant team of health professionals around me – I have written of this on several occasions; hell, I even named my daughter after one of them. But these outstanding, talented, exceptionally smart people do not speak for people with diabetes.
I struggle regularly with the way that we are not considered in the planning and development of new resources, activities, devices and technology designed to ‘help us’. When we pipe up and say ‘hey we’re here’, we often get told that we’ll be consulted ‘later’ – often too late when changes cannot, or will not, be made. That sort of consultation is, I’m afraid, tokenistic. It doesn’t count for anything and those doing this shouldn’t get to then say that they did work with the community.
The experts when it comes to making lives better for people with diabetes are us. The people with diabetes. We’re the ones who live with it, love with it, scream at it and want to turn our backs on it in disgust. We’re the ones who agonise, cry, laugh and celebrate it.
Don’t speak for us. Don’t assume. It should always be nothing about me without me. Always. Listen to us. Ask us. Take cues from what we say. Believe me, we’ll tell you what we need.
Am I being too harsh with this? I wonder what others with diabetes have to say and if they feel the same way.
I haven’t quit sugar and I’ve no intention of doing so because Nutella, doughnuts and the red velvet Tim Tams* that Adriano Zumbo has just developed with Arnott’s. Also, candied bacon.
So looking at the I Quit Sugar Facebook page the other day was a pointless exercise that was only ever going to end in stress eating (of foods mentioned above). And the development of a twitch in my right eye.
The I Quit Sugar (IQS) Facebook admins had caught on that last week was National Diabetes Week and were outraged – OUTRAGED – to discover that on some diabetes sites were recipes containing sugar. Because, you know, sugar causes diabetes. Right?
Wrong!
But let’s not allow facts, a broad evidence-base, and the medical fraternity to get in the way of a good bit of ignorance, will we?
I know; I should have walked away. Shoulda, coulda, woulda. Instead, I read. And read and read and read post after post after post of ignorance and judgement and lies.
Whilst for the most part I sat there shaking my head at the witlessness of the posts, it was when people started outright lying that I decided that I had to write something. One woman claimed that the Australian Paediatric Endocrine Group (APEG) is run by ‘pharmacy companies that make insulin’. She went on to say that JDRF is ‘owned and run by pharmacy companies with an interest in insulin’.
Both these statements are complete lies. The APEG Council is made up of very highly regarded healthcare professionals. The current President of APEG is Professor Fergus Cameron who is the head of Diabetes Services at the Royal Children’s Hospital in Melbourne.
JDRF is a global not-for-profit, raising much-needed funds which go towards research that is looking to find a cure for, and improve management of type 1 diabetes. Run by pharmacy companies? I don’t think so.
The conspiracy theorists on the IQS bandwagon remind me of the anti-vax brigade. The ridiculous claims that the entire medical establishment is simply trying to keep people unwell and feed the pockets of Big Pharma is offensive. The only difference between the two is that the anti-vaxxers are stupid and dangerous. The IQS zealots are just plain stupid.
But here’s the other thing that I find so offensive about so many of the posts from proponents of IQS – the judgement. One woman (in a comment that has now been removed) said she’d like to ‘slap diabetics who eat sugar’.
Quitting sugar is a personal choice – a lifestyle choice, if you will. In exactly the same way that doing yoga, going for a run, not eating red meat or only wearing stripes is a personal choice. These things may work for you, which is terrific, but judging someone because they still want to eat sugar – or wear polka dots – is crazy.
The foolish conspiracies on the IQS website say the advice provided by the medical establishment and health organisations should be questioned and ignored.
But, as I posted in my comment on their FB page, whose integrity should we really be questioning here? Researchers and healthcare professionals with years of training in their specialised field? Organisations supporting people, and raising money to help researchers further developments in living well with these conditions? Or money-making endeavours based on pseudo-science with no evidence-base run by a celebrity?
DISCLAIMERS
*I am so not sponsored by Arnott’s, but seriously – these are amazing! And perfect for an intended week of eating only red food to coincide with a new-found addiction to True Blood!
Professor Fergus Cameron is a member of the Medical Advisory Committee of the Diabetes Camps Victoria Program at Diabetes Australia – Vic. I am employed by DA-Vic and the chair of this committee.
On the third day of #NDW14, I’m trying to avoid the doom and gloom. Which is proving rather difficult, I have to say. Tweet after tweet; article after article – it’s all bad news and promises of complications. The negativity of the reporting of diabetes can get me down.
So I’m trying to equal things up a little.
During the American Diabetes Association conference last month, I saw this photo tweeted.
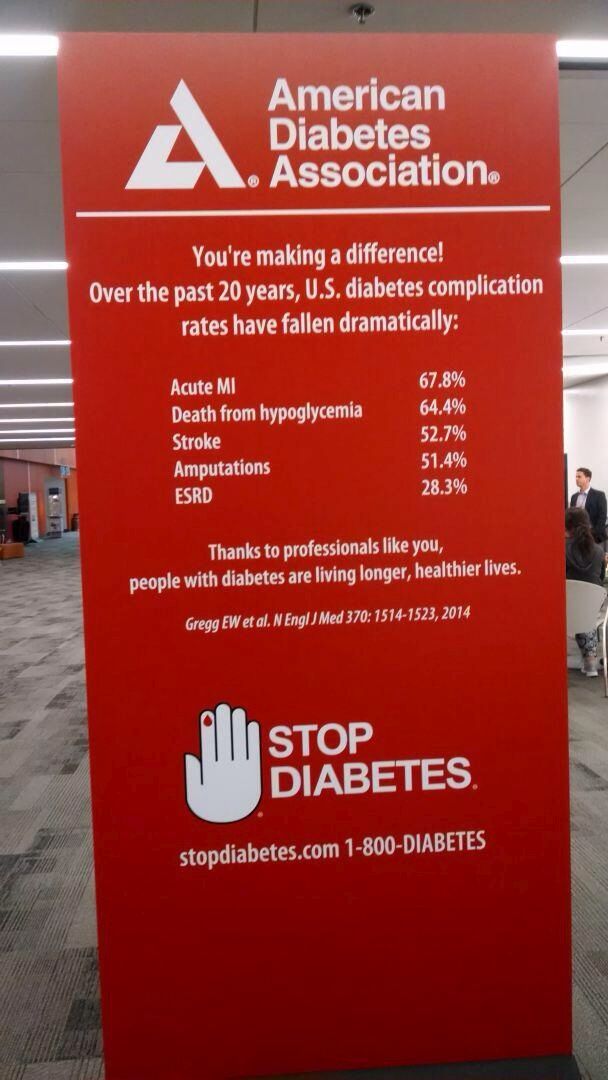
Look at those stats for just one minute and maybe bookmark this page and come back to it if you are feeling overwhelmed by what you’re hearing and reading. (You can read more about this research here.)
And this morning, this one from RCH foundation.
And this from Professor Jane Speight and CERA.
I am not saying that we need to sugar coat (no pun intended) diabetes and only talk about the good things. But the doom and gloom can be a little overwhelming. Equally, I am not here to be Pollyanna and start listing all the reason that we should be celebrating that we have diabetes.
However we can, perhaps, have a little bit of balance. By all means, get the message out that diabetes is serious – it is! But how about also making sure that some of the better news – advances in research; better management options, etc. are reported too. How about we try that for a day?
Have you seen any GOOD news stories about diabetes? As the #OzDOC crowd would say, share the #dlove!
Speaking of #OzDOC – 8.30pm (AEST) tonight on Twitter it’s party time! Follow @OzDiabetesOC and join the two year anniversary celebrations.






