
You are currently browsing the category archive for the ‘Advocacy’ category.
This post was first published in 2011. Sometimes, I think that there is progress being made when it comes to consulting people with diabetes in the development of programs, services and resources for us. Other times, I’m not so sure. Some groups and organisations are incredibly tuned in to people with diabetes (I’m talking about you, Australian Centre for Behavioural Research in Diabetes) and I cannot express enough my gratitude for the high regard of the ideas and thoughts of people with diabetes this group regularly demonstrates.
I stand by what I have written in this post: We are the experts in living with diabetes and we want to work with those who are working to help us. Please, please let us.
——————————
There seem to be a lot of people who like to be the voice of people living with diabetes. Strangely enough, a lot of the time, these voices don’t actually have diabetes themselves.
As far as I am concerned, every single person out there who wants to advocate and support people living with diabetes is terrific. Continue doing it! But make sure that if you are speaking for us you have first heard what we want to say.
Any time an advisory panel or steering committee looking at anything to do with people living with diabetes is formed, the first people invited should be consumers. How can other people possibly advise or steer for us unless they hear what we need and what we want?
If government wants to improve our lot, ask us how to do it.
Experts in diabetes are not the people who care for us. I know how blunt and arrogant that sounds, but it’s true. I have a brilliant team of health professionals around me – I have written of this on several occasions; hell, I even named my daughter after one of them. But these outstanding, talented, exceptionally smart people do not speak for people with diabetes.
I struggle regularly with the way that we are not considered in the planning and development of new resources, activities, devices and technology designed to ‘help us’. When we pipe up and say ‘hey we’re here’, we often get told that we’ll be consulted ‘later’ – often too late when changes cannot, or will not, be made. That sort of consultation is, I’m afraid, tokenistic. It doesn’t count for anything and those doing this shouldn’t get to then say that they did work with the community.
The experts when it comes to making lives better for people with diabetes are us. The people with diabetes. We’re the ones who live with it, love with it, scream at it and want to turn our backs on it in disgust. We’re the ones who agonise, cry, laugh and celebrate it.
Don’t speak for us. Don’t assume. It should always be nothing about me without me. Always. Listen to us. Ask us. Take cues from what we say. Believe me, we’ll tell you what we need.
Am I being too harsh with this? I wonder what others with diabetes have to say and if they feel the same way.
Apparently there is more to write about than diabetes. (The photo is blurred, but the book’s title is 642 Things to Write About.)

After a busy #dblogcheck day, I’m not sure I believe that….
Totally irrelevant, but this was taken on a cold Friday night in Readings, Carlton at an in-store performance by local guitarists Paul Carey and Julian Scheffer. Check them out here, just jamming in the kitchen….As you do.
On the sixth day of #NDW14, I’m looking beyond our shores and remembering that we really are lucky here when it comes to accessing diabetes supplies.
Last night, I attended a special screening of Sweet 16, a movie about a young Canadian woman with type 1 diabetes. The documentary film tells the story of Katia Shannon, who shares her story of life with diabetes.
Featured in the film is Insulin for Life, a not-for-profit organisation founded (and based) here in Australia. There are affiliates all over the world. I’ve known about Insulin for Life (IFL) for a long time and have been aware of the incredibly important work undertaken by this organisation. The objectives of IFL include obtaining diabetes supplies (insulin, syringes, BGL meters and strips) and then donating and distributing them to diabetes associations in countries in need. They also look at developing and implementing sustainable improvements in accessing diabetes supplies in countries in need.
The film last night highlighted a kids’ camp program in Ecuador. The average monthly income for many families in this South American country is $250 and a month’s supply of insulin is $200. Do the maths and think about that for a minute. You can see how dire this situation is for many families. Without IFL, many people in Ecuador would not be able to access insulin to treat their type 1 diabetes. This is just one country supported by IFL.
Today, with National Diabetes Week drawing to a close, have a look at the Insulin for Life website and see some of the amazing and much-needed work they are doing. Supporting them is good karma.
It’s Friday after a very long week, but’s not over yet? So, to keep up our energy, here’s some Georgie Fame to get you (go-go) dancing. Yeh Yeh!
On the fifth day of #NDW I’m shouting #SHOWMEYOURPUMP. Well, maybe not shouting it out to random people – that would be weird – but I’m certainly getting very excited about it.
Last week, the interwebs were on fire with a photo of Bethany Townsend who lives with Crohn’s Disease. Whilst on holiday, she posed in a bikini with her colostomy bags clearly visible. In a campaign of solidarity and Crohn’s awareness, other people with the condition started posting photos online showing their colostomy bags, which are usually hidden away.
Not to be outdone (not that it’s a competition) the diabetes world has our own advocacy queen this week with the newly-crowned Miss Idaho, Sierra Anne Sandison who stood on stage this weekend in a bikini with her insulin pump clipped to her bikini bottoms. Just like that!
And with it came a call for people with diabetes to be just as out and proud by posting photos of themselves with their pump, using the tag #ShowMeYourPump
By last night, the photo of Sierra and her pump had been retweeted nearly 2,000 times and there were hopes that the #ShowMeYourPump tag would trend on Twitter. Today, both my Facebook and Twitter feeds are full of pictures with the tag.
This is an easy, fun and far-reaching advocacy and awareness campaign that (once again) shows how social media can be used for good.
So, for a bit of fun, take a photo of you and your pump. There’s no need to pop on a bikini to do it, but knock yourself out if you want to. For my money, it’s Melbourne black – and far too cold for bikini craziness!

Showing our pumps in the office today. #ShowMeYourPump
Sara from Moments of Wonderful has left a comment below reminding me of this great awareness campaign from a couple of years ago. Pumps and glasses! I thought I’d share it here too.
On the third day of #NDW14, I’m trying to avoid the doom and gloom. Which is proving rather difficult, I have to say. Tweet after tweet; article after article – it’s all bad news and promises of complications. The negativity of the reporting of diabetes can get me down.
So I’m trying to equal things up a little.
During the American Diabetes Association conference last month, I saw this photo tweeted.
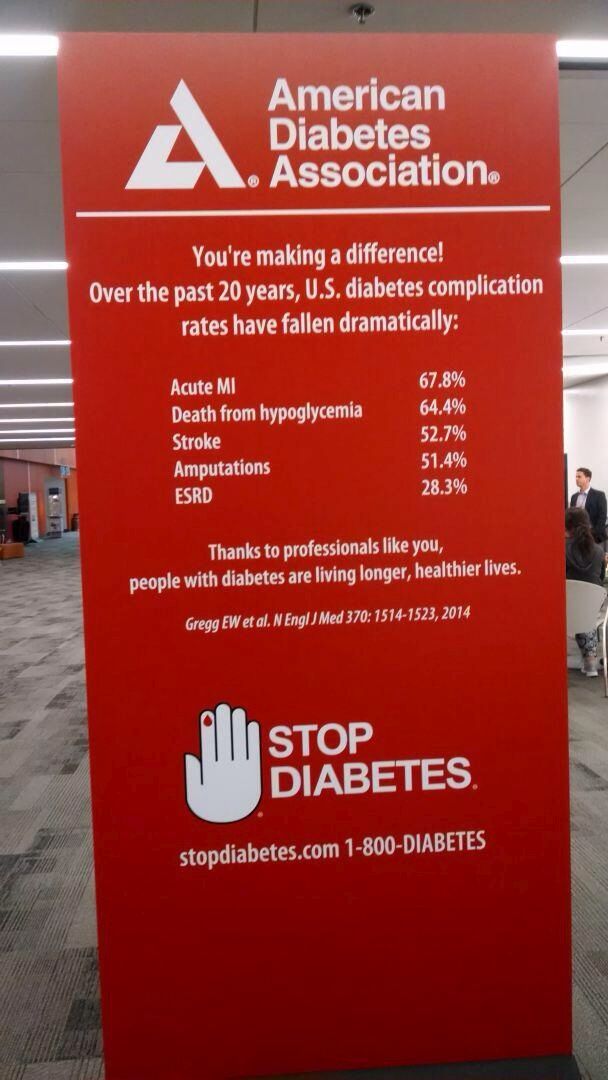
Look at those stats for just one minute and maybe bookmark this page and come back to it if you are feeling overwhelmed by what you’re hearing and reading. (You can read more about this research here.)
And this morning, this one from RCH foundation.
And this from Professor Jane Speight and CERA.
I am not saying that we need to sugar coat (no pun intended) diabetes and only talk about the good things. But the doom and gloom can be a little overwhelming. Equally, I am not here to be Pollyanna and start listing all the reason that we should be celebrating that we have diabetes.
However we can, perhaps, have a little bit of balance. By all means, get the message out that diabetes is serious – it is! But how about also making sure that some of the better news – advances in research; better management options, etc. are reported too. How about we try that for a day?
Have you seen any GOOD news stories about diabetes? As the #OzDOC crowd would say, share the #dlove!
Speaking of #OzDOC – 8.30pm (AEST) tonight on Twitter it’s party time! Follow @OzDiabetesOC and join the two year anniversary celebrations.
It’s the Friday before National Diabetes Week here in Australia. Over the next 10 days, diabetes will be in the press. A lot. And that means a lot of misreporting and a lot of people saying the wrong things about diabetes.
So, here are some of my thoughts about how to address this:
- Stay calm. If you hear or see or read something about diabetes that is incorrect, don’t get angry. Send a balanced, calm response to the journalist, radio/TV station/person talking with CORRECT information. Be brief, use facts – dot points are good.
- Know your facts! And that means no perpetuating other myths to bust the one that’s pissed you off.
- Get over the type 1 versus type 2 thing. Seriously. Don’t bash the ‘other’ diabetes.
- I send the Diabetes Australia Language Position Statement out to any journalist who uses damaging language when writing about diabetes. I tweet the link directly to journos all the time!
- Naming and shaming is okay if you’re nice and polite about it.
- Don’t engage. Make your point and walk away. There is no need to enter into an argument that will most likely get heated and result in abuse. Grace and dignity are amazing qualities; demonstrate them in spades!
- Action! If you’re going to complain, make sure you actually do something meaningful with it. It’s all very well to bitch and moan amongst your peers, but find the source of whatever has upset you and write to them directly. (See point 1 for the tone to use.)
- Follow up. And if you do take the time to write, you should expect a response. If you don’t get one within a reasonable time, re-send your correspondence.
- Pick your battles. I can tell you now that no one has bucket loads of money to spend on diabetes campaigns, so no matter how much you want the government or diabetes organisation in your state to run a full-blown campaign explaining the difference between type 1 and type 2 diabetes, it’s not gonna happen. Accept it!
- Remember that you know a lot about diabetes out of pure necessity. Don’t expect that same level of knowledge from everyone. Most of the stupid things people say are out of sheer ignorance or bad manners. Politely correct and move on.
- There are some great resources out there that can help. Check out this and this.
The primary aim of National Diabetes Week is to raise awareness of the condition – specifically awareness about prevention of type 2 diabetes. Consider any misreporting or silly comments an opportunity to provide information and education in the hope that the people perpetuating the myths won’t do it again. And as your (and everyone’s) grandmother would say: Keep yourself nice.
It’s Friday! And it’s freezing here in Melbourne. I’m trying to imagine warm sun on bare skin, so here are The Beatles with ‘I’ll Follow the Sun’.
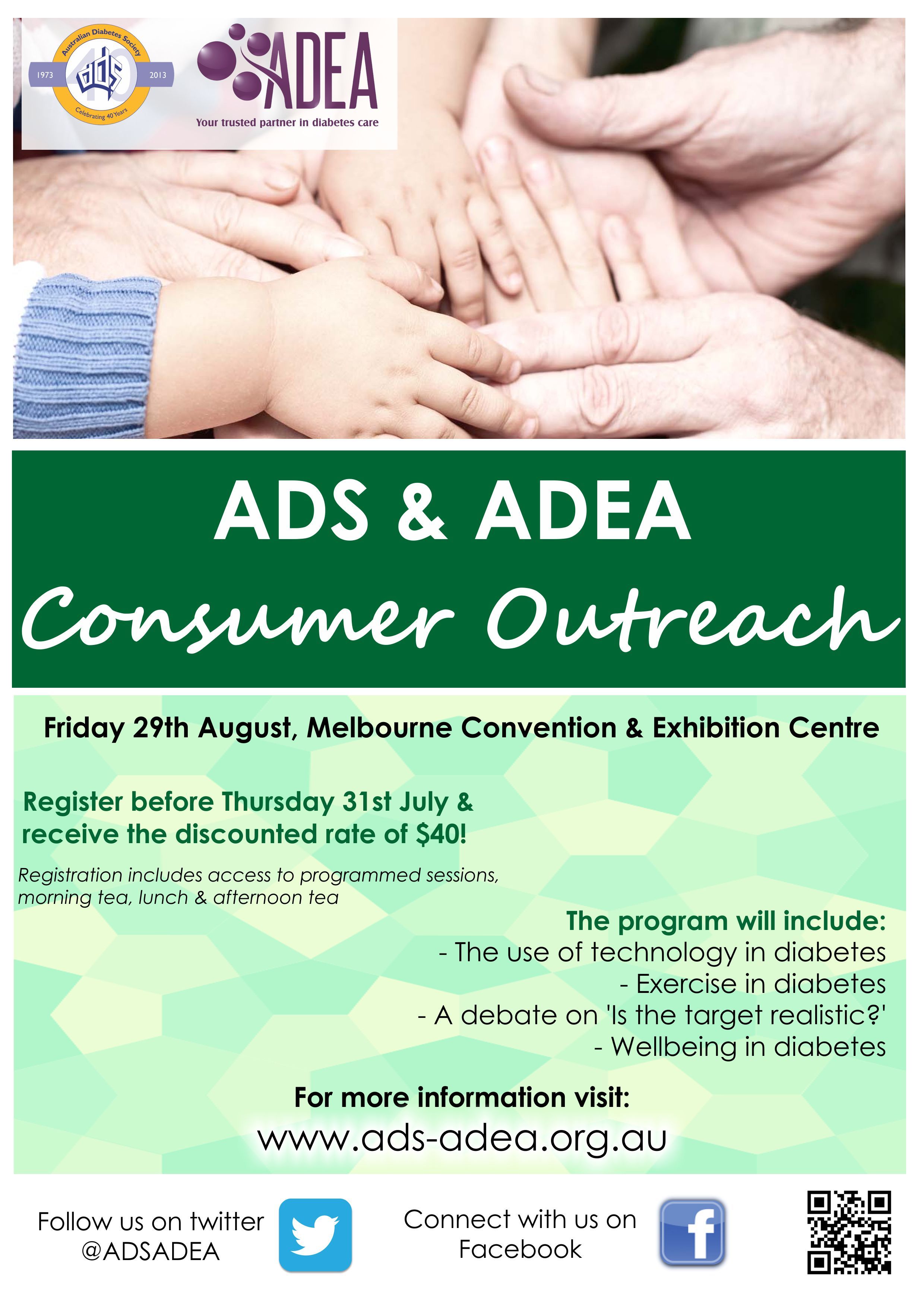
Next month the annual ADS-ADEA Scientific Meeting will be held in Melbourme. This is the leading diabetes conference in Australia and attracts diabetes healthcare professionals from all over the country and boasts a program of outstanding local and international speakers.
This year, for the first time, there will be a consumer stream as part of the conference. This is really exciting because it seems that finally, after many years of petitioning (by petitioning, I mean whining), people with diabetes are actually involved and encouraged to attend.
Details of the Consumer Outreach day are below.
Someone has commented to me on Facebook that registration should be free for consumers and whilst I understand the reasoning behind that, I also know the costs involved in putting on a conference of this magnitude. I also know that sponsorship dollars are tight at the moment. I would urge anyone who wants to attend, but cannot afford it, to contact their local diabetes organisation and see if there is any way they can contribute to the costs.
I also know that having an event during the day on a Friday may not be ideal for many who work. But that’s the reality – conferences are held during the week. If you have any time in lieu owed, or an annual leave day you are prepared to take, this is a great way to spend it! Not only will you get to hear some interesting presentations, but it will be an opportunity to hang out with some incredibly awesome diabetes people.
Peer support for the win!
SCHOLARSHIPS AVAILABLE
#OzDOC will be providing two scholarships to cover the cost of registration for the event. To apply, jump on Twitter and send a direct message to @OzDiabetesOC. Make sure you include your email address in your message. You’ll then receive an application form. See you there!
DISCLAIMER
I am on the organising committee for the Consumer Outreach program. I am not receiving any payment for my involvement in this committee; however, my registration fee for the entire conference has been covered. I am also an invited speaker at the ADS-ADEA conference (at both the healthcare professional and consumer sessions and I have been involved in the submission of two abstracts that have been accepted for presentation at the conference).
It seems that barely a day can go by when mainstream media doesn’t report on the latest ‘thinspro’ trend – always dangerous; frequently scary and mostly downright disturbing. In this weekend’s The Age was an article about a new phenomenon – the triple zero dress size. I can’t even fathom what that would look like, but I am no longer surprised when I read these articles.
A few years ago now, I managed a project about diabetes and eating disorders. The project was funded by the NDSS and the aim was to produce a national resource that would address the issues of diabetes-related disordered eating behaviours.
As is often the case, I started off thinking I had a pretty good idea of what the project would be about and how it would end up looking, only to realise how completely off the mark I was. I had no idea just how complex diabetes can make eating disorders. In addition to ‘traditional’ eating disorders, throwing diabetes into the mix meant addressing insulin manipulation, restriction and/or omission for weight loss. Often referred to as ‘diabulimia’ (a term that I personally despise for its sensationalist leaning), this issue has been covered in mainstream as well as diabetes-related media in recent years.
As our work started, I could see the complexity of this issue. We worked with the Centre for Adolescent Health at the Royal Children’s Hospital, Melbourne and developed an anonymous online survey and, from the results, a report addressing the most significant issues. The report focussed on women with type 1 diabetes aged 18 to 35 years.
One of the startling things to come from the research was how rarely insulin omission was actually discussed with HCPs. In fact, the survey showed that 85 per cent of females with type 1 diabetes had never been asked about insulin omission, and of these women, about 50 per cent were restricting or omitting insulin with the aim of losing weight.
We heard over and over and over again how isolated people felt. Frequently, we read comments where people thought they were the only ones engaging in this behaviour and thought there was nowhere to turn. They feared they would be judged by others and that no one would be able to help them. They were scared to mention their behaviour to their healthcare team.
Following the publication of the report, I did a lot of presentations at diabetes (and other) conferences about our findings and the resource that was subsequently developed. And one of the things I always spoke about was the feeling of isolation reported by the women who completed the survey.
The response to these presentations startled me at times. In the Q & A section of one session, a dietitian stood up and said she was horrified that we were developing a resource for people living with diabetes. ‘You’re developing a how-to for people’, she told me. I, in turn, was equally horrified at her response.
I think that, given the results of the survey (which were in line with international literature) we could safely say that many people with diabetes had put two and two together to work out insulin restriction results in weight loss. (Those of us who can remember our diagnosis often talk about the rapid and sudden weight loss we experienced prior to diagnosis and commencement of insulin therapy.)
Not talking about this very serious issue sends it underground. It contributes to the feelings of isolation we heard about and it means that people engaging in these behaviours feel unable to address them.
Instead, I believe we should be discussing diabetes and eating disorders – a lot – and ensuring that people feel safe and secure talking about it with their HCP, confident in the knowledge that they will not be judged and that there is help at hand. Sweeping it under the carpet does not make it go away; it just causes a lump that we keep tripping over.
In the recently launched resource for adult endocrinology trainees, Enhancing Your Consulting Skills, there is an entire chapter dedicated to eating disorders, including offering specific words to use to ask people with diabetes if they are engaging in insulin restriction or omission for the purpose of weight loss. This is a huge step forward!
Some (many?) of the things that go with living with a chronic health condition are incredibly difficult. This is indeed one of them. But just because it is hard and not easily defined or dealt with does not mean that we should ignore it or put it in the too hard basket. In fact, I believe, we should probably give more attention to it until it becomes something that is routinely discussed and assessed.
MORE INFORMATION
Eating Disorders Foundation of Victoria






