Come fly with me…. (2015 to Orlando)
By the end of this year, I will have travelled overseas five times and interstate heaps more. And over the last few years, have done a lot of travel – for business and pleasure with my family. So with this recent experience under my belt, I decided to enter Diabetogenic into the Top Travel Tips competition run by Virgin Australia and ProBlogger with some tips and tricks that I have learnt on my travels.

Always visit the city public library. (Boston 2015)
‘Travelling with diabetes’ is just ‘travelling’ for me. It’s not like I can leave the diabetes at home – I asked and it refused. I have never considered diabetes as being a reason to not travel. It just takes some planning. But then, so does travel in general!

Steamboat Natchez (New Orleans 2013)
As I have said frequently, diabetes adds an extra degree of difficulty to life. And it is the same with travel. It’s not anything all that significant, just something to consider. So here are my fail-safe tips to travelling not only safely, but also ensuring that a wonderful time is had.

Camels in the Atlas Mountains (Marrakech 2013)
1. Have fun!

Lady Liberty (New York City 2010)
2. Don’t let diabetes be the reason that you don’t travel. And further to that, don’t let diabetes be the reason that you limit your travel to areas you consider ‘safe’.

Shoes in every possible colour combination. (Barcelona 2013)
3. Read points one and two again.

Ice skating in Central Park (New York City 2011)
4. Work out what diabetes supplies you need to take. And then double it. I know: diabetes paraphernalia add bulk and that is a pain – especially when you are trying to travel light (a concept completely alien to me, because: shoes). It is highly likely that you will end up coming back home with a lot of the extras, but that is a far better option compared with trying to work out how to access insulin/pump lines/BGL strips etc. when you are in the middle of a cooking with truffles tour of southern Italy. (Note to self: find and book cooking with truffles tour in southern Italy.)

The magic of a gondola (Venice 2009)
5. And again – I know it’s a pain, but carry things with you rather than packing them away with your stowed luggage. That way, you know where it all is, and the insulin won’t be subject to significant temperature changes. I do know of people who stowed their insulin and it froze, rendering it useless. And someone else whose luggage sat on the taxiway in direct sunlight for 6 hours cooking their insulin. It’s unlikely, but in rare cases, it can happen. You don’t want to be that person!

Mozart everywhere! (Vienna 2012)
6. To declare or not to declare? That is the question. I never walk up to security and announce that I have diabetes. But equally, if necessary, I am happy to answer any questions. I seem to set off security alarms with alarming (!) regularity. By the time my shoes have come off, and any jingly-jangly bracelets are removed, I still frequently set off the alarm. No idea why. At that point, with a pat down on the way, I do point out that I am wearing a couple of medical devices, pointing to them on my body. I am always relaxed about it and willing to pull them out for show and tell. It’s never ever been a problem. Ever. And I don’t assume that the security person will know what I am talking about, so I use simple terminology when explaining what they are for. Often, an interesting conversation ensues!

Dubai 2011
So on that: stuffed in with my travel documents is a letter from my endocrinologist stating that I have diabetes. That letter has never, ever come out – I’ve never been asked. However, it always there, because it is a piece of paper, weighs nothing and the day I decide I don’t need it will be the day I am asked for official documentation to prove my faulty beta cell status.
7. For pump users. Having an insulin pump undoubtedly makes travel easier. No need to do any sorts of tricky calculations for time zones and working out what time to take your long acting insulin. I always have the same procedure: once it’s wheels down at my final destination, I reach for my pump and reset to local time. That’s it! Done! I don’t do it earlier in case of any delays along the way.

Denmark Street for music stores (London 2014)
TAKE A PUMP BACK UP. Most pump companies offer loan pumps. Just make sure you give yourself enough time to organise one.

Oh, Paris. (2008)
Write down your pump settings. I save the settings in my phone and save a copy in the cloud as well. Because I seriously couldn’t tell you my insulin sensitivity factor (or anything else) if my life depended on it. Which it kinda does!
Pumps fail. It’s a reality. It’s crap. And even back up pumps fail. I know the likelihood is small, but it can happen. And if it does, you’ll still need insulin – both basal and bolus. So with that in mind, don’t forget long acting insulin. You can get pre-filled pens if that is your preferred option (don’t forget you’ll need needle tips!). I take syringes because they are easy to use, light, and do the trick!
8. Travel insurance. Don’t leave home without it. And don’t forget to disclose diabetes.

Apartment doorway. (Rome 2012)
9. Medical ID? Some people don’t go to the corner store without their medical ID. Other people rarely, if ever, wear something (guilty as charged). It is an incredibly personal decision as to whether or not you wear something identifying you as someone with a health condition. Think about where you are travelling, if you will be spending periods alone and if you think that having a medical ID would be the best thing for you.

Montmartre (Paris 2013)

The gorgeous seaside Honfleur. (Normandy 2009)
10. Frio packs are great if you are travelling to hot places and you are not sure the availability of a safe fridge. I have found (increasingly) that some hotel rooms don’t even have fridges in them anymore; in Boston, I spent 10 minutes looking for a cleverly hidden fridge in my room at the Hyatt only to realise that there wasn’t one! Having said that, insulin is a lot hardier than our pharmacists would like us to believe, and it won’t disintegrate before your eyes if it’s not refrigerated constantly.
11. One of the best things about travelling is exposure to new foods. Often what you are eating and its nutritional value are a complete mystery. Eat it anyway. You can always correct a high blood sugar or treat a hypo. Don’t let diabetes be the reason to not try the local delicacies.

So much delicious food. Carb counting is your friend!
And while we’re talking food – think about the food available while you are actually in transit. Aeroplane food will never be the best food you will eat. I have never, ever, ever ordered the meal for PWD, but I know others who do and say it’s fine. Don’t think you HAVE to order a special meal just because you have diabetes.

There seem to be some recurring themes in our travel photos. (Coffee everywhere)
I always make sure that I have my own hypo stash while on planes. But don’t worry if you don’t (or if you’ve already munched your way through). You can always get juice on flights. (Don’t forget – on some flights food and drinks are not included in the fee and you will have to pay on board.)

Ampelmann (Berlin 2012)
12. I don’t exercise, so when I travel, I spend the first couple of days low until I remember that I am walking miles and miles and miles. And then remember to alter my basal rates on my pump. (If I was smart, I would do this before the hypos start. I am hoping to become that person one day.) Same thing applies, of course, if you are usually super active and suddenly doing nothing but lying on a lounge chair, reading a book and doing nothing more than waving your hands at a waiter for another cocktail.
13. The Diabetes Online Community (DOC) is your friend! There are people with diabetes EVERYWHERE and we’re a helpful bunch! If you’re in a pickle, social media might just be the thing to connect you with someone to help you out. (And here is the famous Pumpless in Vienna story again.) And even if you are not having a diabetes crisis, travel is a great chance to meet up with people you’ve gotten to know in tweetchats and diabetes discussions online.

Bright (xmas) lights, big city (New York City 2014)
One of my favourite things when travelling is to do just that. I have spent countless hours all over the world getting to know people from the diabetes online community and they have moved from being wonderful cyber friends to truly wonderful in-real-life friends. Diabetes may have connected us, but there is much more that has secured that friendship!

Yankee Stadium (New York City 2013)
14. Shop for diabetes! (Yep, of course there is a shopping angle.) Shopping overseas gives you access to things you may not find at home – especially if you visit markets and fairs. I have found gorgeous little purses for my diabetes supplies while travelling and one of my favourite bags ever was bought on the Rialto Bridge in Venice from a man who makes all the bags in the store. (I justified the purchase by the size of the bag, telling myself it would carry everything I needed for my diabetes for the rest of the trip!)

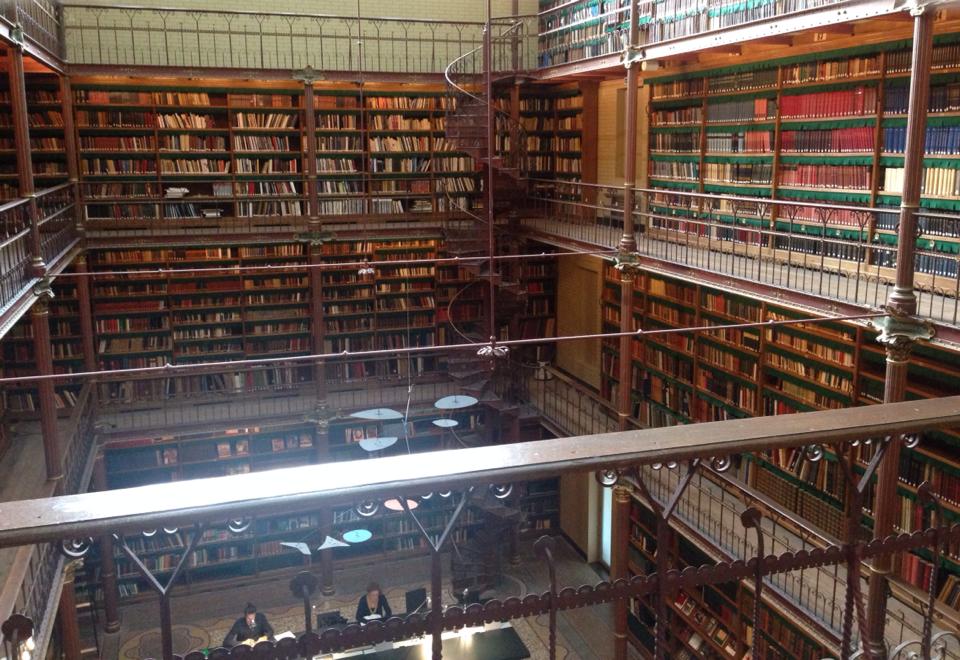
Rijksmuseum Bibliotheca (Amsterdam 2014)
Travelling should be fun and exciting and enlightening and enriching. It’s a chance to spread your wings, find new places, meet new people and discover new things about yourself. It’s an awesome ride, and diabetes – whether you like it or not – is there with you. Most of all, remember what I wrote in this post here:
The theory of travelling and diabetes is different for every person and every trip. And every trip I learn something new – and not everything I learn is about diabetes!

We have made a point of visiting somewhere new each year over the last five years.