
I have written (frequently) before about T1 International and I am going to do it again this Diabetes Awareness Month.
Because the team at T1International have a new initiative: they are urging people to sign their Type 1 Diabetes Access Charter which outlines five rights that all people with diabetes should have:
- The right to insulin
- The right to manage your blood sugar
- The right to diabetes education
- The right to healthcare
- The right to live free from discrimination
None of these things are luxuries. These are basic human rights that should be afforded to every single person diagnosed with diabetes – not just those of us lucky to be born in a country such as Australia. Insulin is not a new-fangled, fancy drug. It has been around for 95 years. When talking about the right to the tools required to manage bloody sugar, we are not talking latest technology such as continuous or flash glucose monitoring or hybrid-closed loop systems that are entering the market. We are talking about basic blood glucose meters and strips.
The reality is that around the world, many people cannot access or afford insulin or diabetes supplies. Education is sporadic at best. People with diabetes are being forced to choose between buying insulin and buying food or other essentials. How do you make the decision between putting food on the table or buying the life-saving drug you – or your loved one – needs to stay alive? It’s a decision that most of us in Australia never have to even contemplate, but it is a reality for many, many people around the world.
I messaged T1 International founder, Elizabeth Rowley, yesterday to let her know I would be writing about the charter today, but I also wanted to comment on a Facebook post she had just shared.
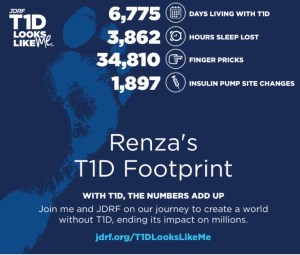
Elizabeth had used the JDRF diabetes stats calculator (as discussed in yesterday’s post) and shared her results. She had a very different take to how many others responded.
She reminded us that she is the one of the lucky ones because in her almost 25 years as a PWD, she has been able to access whatever she has needed to manage her condition.
When I did my diabetes numbers, I looked at the terrifying number of BGL checks I have done over the last 18 years: 34,749 (although Aaron did suggest that during pregnancy alone I would have done that many!). Not once have I ever had to wonder from where I would be getting my next box of strips. Not once have I thought about rationing strips or pump consumables for fear that I could not afford more when I ran out. Not once have I had to consider taking less insulin that I need.
The scary thing about the numbers generated by the JDRF calculator is not the huge numbers many of us are seeing tallied up. In fact, it is actually the small numbers in those people with diabetes who can’t access what they need to manage their diabetes.
T1 International is doing some amazing things – just as they have done since they started a yea few years ago. Please check out their website, click below to sign the charter and get your friends and family to sign too, and if you can, make a donation to this really important cause.




 Get logging for good karma. There’s even an app you can use to make it super easy. (And yes – I’ll be logging before and after I take the pups for a walk!)
Get logging for good karma. There’s even an app you can use to make it super easy. (And yes – I’ll be logging before and after I take the pups for a walk!)





 In the last ten days, I’ve visited houses from my childhood. By some weird coincidence, the house I grew up and lived in until I moved out at 21, and the house my dad grew up in and I spent countless Sunday afternoons with my extended family are both up for sale. I walked through the houses and memories flew around me, launching me back years.
In the last ten days, I’ve visited houses from my childhood. By some weird coincidence, the house I grew up and lived in until I moved out at 21, and the house my dad grew up in and I spent countless Sunday afternoons with my extended family are both up for sale. I walked through the houses and memories flew around me, launching me back years. It settled into my in-laws’ house in the country. We’d arrive at the farm in need of a cup of tea after a long drive and I’d open the fridge for milk to find insulin staring at me. And I’d sigh, slightly startled, as I checked to make sure it was still in date, replacing it with fresh vials from my bag if not.
It settled into my in-laws’ house in the country. We’d arrive at the farm in need of a cup of tea after a long drive and I’d open the fridge for milk to find insulin staring at me. And I’d sigh, slightly startled, as I checked to make sure it was still in date, replacing it with fresh vials from my bag if not.







