The current COVID-19 situation in Australia is not great. We seem to be on the cusp of a major outbreak, centred on a growing wave of new diagnoses out of NSW. Watching it all unfold from Victoria is somewhat triggering, and eerily familiar. The difference in 2021, of course, is that we now have vaccines to help combat the virus. Admittedly, our vaccine rollout is nothing short of a disaster, and that’s a massive problem when there is an outbreak like the one we’re facing right now.
And so, that brings us to last night’s latest throw-shit-at-the-wall-and-hope-something-will-stick approach that seems to be the method preferred by the Australian Government. And the latest shit is a new advertisement with the aim of encouraging people to get vaccinated. For the record, it hasn’t stuck.
I’m not going to share the ad because it is traumatising. The general gist is that it shows a woman who appears to be under forty years of age in hospital with COVID struggling to breath. She is intubated.
It is terrifying.
Setting aside the fact that the woman in the ad probably couldn’t have been vaccinated even if she desperately wanted one (our rollout is still being managed by age, and under 40 year olds are certainly not anywhere near at the top of the queue yet), or that, according to healthcare professionals, there is no way that she would have been left untreated if she was struggling to breathe in that way, the way this advertisement has missed the mark is outrageous for a number of reasons:
It blames the individual for not doing the right thing rather than looking at the systemic issues that have hampered the rollout, which includes precuring enough vaccines, starting the rollout late, blundering the messaging, messing up distribution … and everything in between.
It terrifies people and is likely to not illicit a response other than fear.
There is no consideration for people who have COVID right now. How would family of someone currently in hospital feel seeing this? How traumatising would it be?
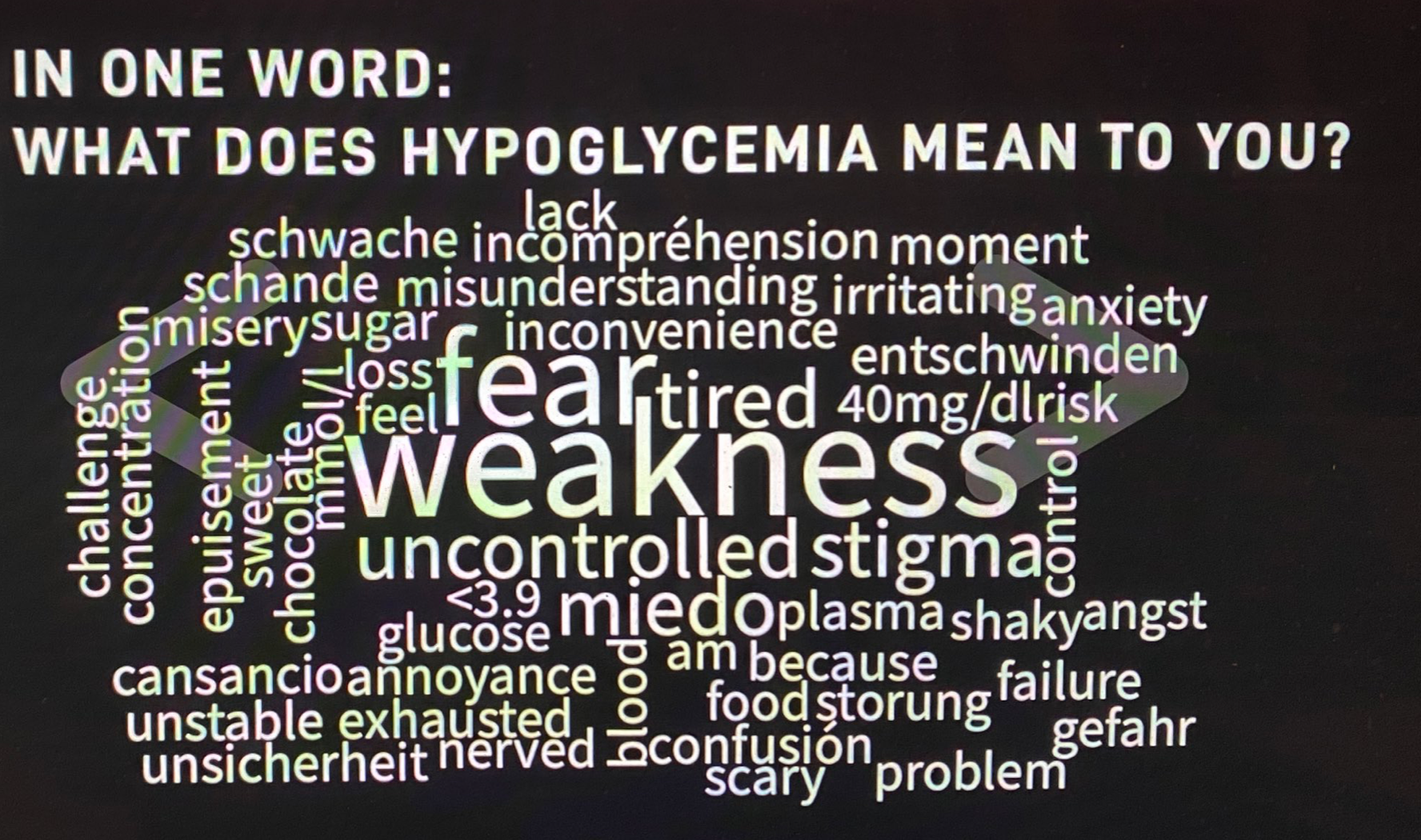
I watched the ad – once only and with the sound down after the first 4 seconds – and felt a ginormous sense of déjà vu. A fear-based ad campaign has been the basis of diabetes campaigns for many years, despite pleas from the diabetes community to do something better, and a realisation that the general community wasn’t bothering to pay attention.
Thankfully, in recent years here in Australia, we’ve moved away from scary ads, understanding that we can provide a hard-hitting message without using scare tactics. Diabetes Australia has absolutely nailed that in recent years, firstly with a three-year campaign raising awareness about the signs and symptoms of type 1 and type 2 diabetes. And we are now in year two of a campaign looking at the mental health aspects of diabetes. (As ever – my disclosures are important. I work at Diabetes Australia and have been involved in all these campaigns.)
Advertisements based on fear and blame don’t work. Last night, I kept seeing people online harking back to the Grim Reaper campaign that was launched in the 1980s to raise awareness of AIDS, some claiming that it was brilliant because they still recall it. I remember the TV ads. But what I know now, but didn’t know then, was that one of the major flow-on effects from this campaign was stigma directed towards gay men – added stigma, I should say. This stigma took many years to turn around. Notoriety doesn’t not equal an effective campaign.
But jeez, it sounds familiar!
Here we are this week talking diabetes-related stigma and how we undo it, and part of that stigma – the misunderstandings about diabetes – came from campaigns being run by diabetes organisations. While I’m thrilled that here in Australia we’re doing a better job at moving away from that (albeit with a hiccough here and there), not all people working in diabetes organisations got the memo. It was just eighteen months ago that I sat on a panel with the incoming IDF President and had to address his idea that ‘fear arousal’ was worth considering as a way to raise awareness of the seriousness of diabetes.
No.
Just. No.
And so, back to the disaster of the COVID vax ad. If only instead of terrifying, there was a focus on incentivising. If only instead of putting all blame on the individual, there was a celebration of communities coming together. If only instead of finger pointing at people desperately ready to get a jab there was acknowledgement of how difficult and confusing it’s been.
If only…