
You are currently browsing the category archive for the ‘Wellbeing’ category.
I made a commitment to do the #30DaysOfDex challenge at the beginning of the year. Actually, I have been wearing a sensor continually since the beginning of December; so really, I am at about day 45 now.
I have a love/hate relationship with CGM technology. I adore it far more than I dislike it, but still, there have been times that when I simply can’t face wearing it. But that actually has nothing to do with the actual tech. I wear a device that I truly believe I can rely on – and I know that because calibrations are spot on. Even though I’ve been using this particular type of CGM for about 3 years now, I am still surprised at just how accurate – just how often – the results are.
No, the reason I don’t wear it all the time is because I have found it too burdensome when headspace is not right. When there is too much else going on or I am feeling overwhelmed, I just can’t face alarms and numbers and a machine that demands I be responsive to it.
But through some trial and error, I have found ways to lessen those demands, yet still use the device effectively.
Firstly, I’ve had to identify what I hope to achieve from wearing a CGM. Really, there are two aims: have fewer wild BGL swings and pick up hypos as early as possible with a hope of avoiding.
I also identified what I didn’t really care about and that included having a BGL sitting at 5.5mmol/l the whole time. In fact, I am not even aiming for BGLs between 4 and 8 the whole time. I raised the upper limit to avoid some alarms. I don’t want to hear screeching every time I hit 7 or 8mmol/l. At this stage, I am not interested in that. I don’t mind if I hit 10 or 11 after a meal, as long as it doesn’t sit there all day.
It’s not about the number values – for me it’s about fewer variables, because when I am all over the shop, I feel like crap.
So what have I found after a month and a half with this attitude? By and large, it’s been a successful experiment – am far more responsive to the alarms that sound now and I don’t feel frustrated. And I am able to find patterns. It is incredible how I was low or high at the same time each day without knowing it. Or rather, I probably did think it was the case, but with the data and graphs, there is no way of hiding it. I don’t log – it’s been a long time since I had – so I was relying on memory. ‘Was I low at 3pm yesterday as well? Maybe…. Was I? Or was I high?’
The thing that I have come to understand about CGM (and I may be a little slow to the party here) is that the ability to customise it means that I can find a way to benefit from it, even when I am feeling totally burnt out and can’t be bothered with the minutiae of my diabetes.
I don’t need to have a perfectly straight line for CGM to be considered successful. It’s not a waste of a sensor (and therefore a waste of money) if my BGLs do hit and play around at 10 or 11 for a while. This is kind of a breakthrough for me – I’m feeling quite proud!
Something else that has become clear while wearing CGM is that my BGLs are actually not as unstable as I think they are. Oftentimes, I am sure that I am really high, or moderately high or really high. I know that if I wasn’t wearing CGM and was feeling unmotivated, I would use that as an excuse to not check. ‘I know I am high. I don’t want to see a high number because it will make me feel worse. So I am going to bury this head of mine in this sand over here and forget about diabetes.’ Diabetes? What diabetes? Let’s build a sandcastle!
The reality is that of course my numbers are not perfect, but they are actually, most of the time, okay-ish. And I am generally okay with okay-ish! Okay-ish keeps me sane and keeps me happy.
CGM makes me think about my diabetes more. It makes me in tune with it more and it does make it easier for me to manage. Perhaps I have taken a long time to work out how CGM works for me – maybe I have wasted some time or not worn it when I could have benefitted. But for now this is what works really well. And it’s a really good way to start the year.

This week is Jean Hailes for Women’s Health Women’s Health Week. (Yes, there’s a lot of women and health in that sentence, but given it’s the focus of the week, let’s work with it.)
I quite love the theme of the week which is Let’s Talk. The idea is that we get rid of the elephants in the room and talk about health issues that we sometimes find tough to discuss. It’s a great concept! Having people opening up – or at least being able to access information – about health issues that are sometimes not discussed is really important. Plus, there are gorgeous pink elephants all over the promotional materials and that can only be considered a good thing!
Now clearly, I don’t have an issue speaking about health issues. I very openly talk about my experiences living with diabetes. I have willingly and candidly spoken about fertility issues and miscarriage. I have also discussed the body image concerns that I have lived with for most of my life. Mental health is frequently discussed on my blog – usually in relation to diabetes.
But while I am happy to bang on about any health concern that I may be dealing with, that isn’t the case for everyone. That’s why this week is an important one.
And it is why we need people who are happy to share their stories out there. We need people to be discussing the things that are a little ‘underground’ or that make people squirm a little.
 Each day of the week has had a different focus. On Monday, the results of an online survey were released. The survey combined responses from 3,300 women aged between 18 and 87 years, and healthcare professionals including nurses, GPs and HCPs.
Each day of the week has had a different focus. On Monday, the results of an online survey were released. The survey combined responses from 3,300 women aged between 18 and 87 years, and healthcare professionals including nurses, GPs and HCPs.
Yesterday, the attention was directed towards natural therapies, looking at the safety and effectiveness of natural medications and treatments. There was great advice about questions to ask (yourself and your HCPs) before taking any natural therapies.
Today, it’s all about what is not being talked about. Starting with the difficult topic of domestic violence, the website provides advice about the issue and lists placed to go to for help. While there has been quite a bit of attention in the media given to domestic violence this year, the statistics are horrendous and we need to be doing more.
Also on the agenda for today is mental health and there are links to some valuable information about depression, anxiety and emotional health.
The rest of the week is about managing our health and healthy living.
I understand that not everyone is happy to share their story. And that is fine. But even those who prefer to stay silent and keep any health concerns to themselves still may look for information and advice. And shining a light on some of the less talked about health problems faced by Australian women with a bright and bold campaign does just that.
So. Let’s talk!
I frequently give talks about how to get the most of our healthcare professionals. One of the things I talk about is making sure that we find the HCPs that work best with us. I talk about interviewing doctors – something that I did years ago when I was looking for the right endo. It’s a two way street. One doctor told me that he didn’t think that we would work well together. He was completely right and I walked out of that appointment rather quickly!
I also talk about being really clear and upfront about things – what we need from our HCP, what we expect. And then give them the opportunity to do the same thing.
This is pretty much what I want to say to every HCP when I meet them for the first time.
Dear Doctor
Hi. You and I are on the same side. My side. We are both championing for me to be the best I can be with the cards I’ve been dealt.
I thought that we would start out by me telling you what I need from you and I would love it if you did the same. This is a relationship that works two ways. You need things from me and I need things from you. Let’s get all that out on the table from the beginning.
Mutual respect is really important. I come with mine ready to give to you. I won’t, however, be quite so generous if you don’t demonstrate the same thing.
Judgement is not welcome in our consultations. That message is actually for me as much as it is for you, because I am totally judging you. I expect you to be judgemental and not understand me or my condition. Show me that I’m wrong. And then don’t judge me for being such a pain in the arse!
My health condition is one that you know a great deal about. That is why I am coming to see you. I want to know everything thing you know that is relevant. But I need you to remember that I have a unique expertise in the field of Renza’s Diabetes. I am the world expert in this field and I will impart everything I have learnt and continue to learn about it to you. If you could then help me make sense of that, I’d really, really appreciate it.
I am not stupid. I have a really good understanding of the health system of which I am, unfortunately, a user. I also know a lot about the technical sides of my condition. I totally get that you need to make sure that I am clear about what you are saying, but please don’t dumb it down too much for me. I promise that I don’t care about looking stupid. I’ll ask if I don’t understand.
I use humour a lot to try to deal with what is, at times, a really scary thing to live with. Sometimes you may think that my humour is not particularly appropriate. A lot of the time you won’t find me funny (but for both of our sake, please pretend; I promise to ignore your fake laugh). I don’t make fun of the situation because I am making light of it. Or because I don’t care. I always care a great deal. But sometimes, it’s what I need to get me through.
I’m really not good at asking for help. But I am coming to see you because I need it. I may seem to be going the long way around getting to actually ask for what I need. Feel free to ask and prompt and even push a little.
I’ll say it again. I care a great deal about my health. I want to be healthy and well and on top of everything. There will be times – and they may be extended times – where it seems that I don’t care. The important word there is ‘seems’. I do care. Really. Sometimes though, it is just overwhelming and exhausting. But I really, really do care.
I have a beautiful family and a great job and a shoe collection that may make you jealous and really like to drink coffee. I bake a lot and love old black and white films. I have wonderful friends I spend time with – frequently over a meal somewhere. Exercise and I are not mates. I read voraciously and should probably seek some sort of therapy for my inability to stop buying books. I have a thing for bright red lipstick and have too many handbags. I love Nutella. And bacon. And doughnuts. You may wonder why I am telling you this. It’s because all of these things are part of my life. Just like diabetes. And it goes to explain why diabetes is not the most important thing in my life or the thing that I focus on all the time.
I’m terrified about my future. I am scared about diabetes complications, I lie awake at night worrying about the chance of my daughter getting diabetes and I fear becoming a burden on my loved ones. Diabetes is scary. It is not just a condition of numbers and lab results. It is (an unwelcome) part of my present and my future.
I solemnly swear that I will never, ever walk into your office asking you about some ridiculous cure I read about on the internet. Remember that bit about me not being stupid? But equally, the internet is where I get a lot of my support and information about living with diabetes. I have a support network of people living with diabetes from all around the globe. They build me up, tell me about new things, help me work through tough times. They are, to me, as important a part of my diabetes management as you are. Don’t treat them with suspicion.
So, did you know that cinnamon can cure diabetes? I’m disconnecting my pump and eating cinnamon doughnuts and nothing more for a week to see how it goes. Just kidding. (Pretend laugh. Now.)
And finally. I want you to remember all the time that I am doing the best I can at that very moment. It may not be as much as you would like, but this isn’t about you. It’s probably not as much as I would like either. Acknowledging what I am doing makes me feel really great. And frequently then makes me want to do better.
Thanks for reading. I really do hope this is the beginning of a beautiful doctor-PWD friendship.
Best
Renza
Friday tunes. Oh, Vinnie Barbarino!
National Diabetes Week is an important week for people living with diabetes in Australia. It is an opportunity to have all types of diabetes given attention and focus in the media and to talk about the significant health issue it is – for people living with diabetes, their families, and health systems.
And sometimes, messed up in the campaigns and the social media onslaught, we get sidelined by arguments and heated discussions, and we start to forget one of the real reasons this week is important: how diabetes affects those of us actually living with the condition.
Today, I helped launch a new report. The Diabetes MILES Youth survey was conducted last year and the results have now been published. The survey aimed to examine the impact of diabetes on young people living with diabetes and their families.
The report (which can be found here) shows that a quarter of young people living with type 1 diabetes experience moderate to severe depressive or anxiety symptoms. This image shows the top problem areas for girls and boys.
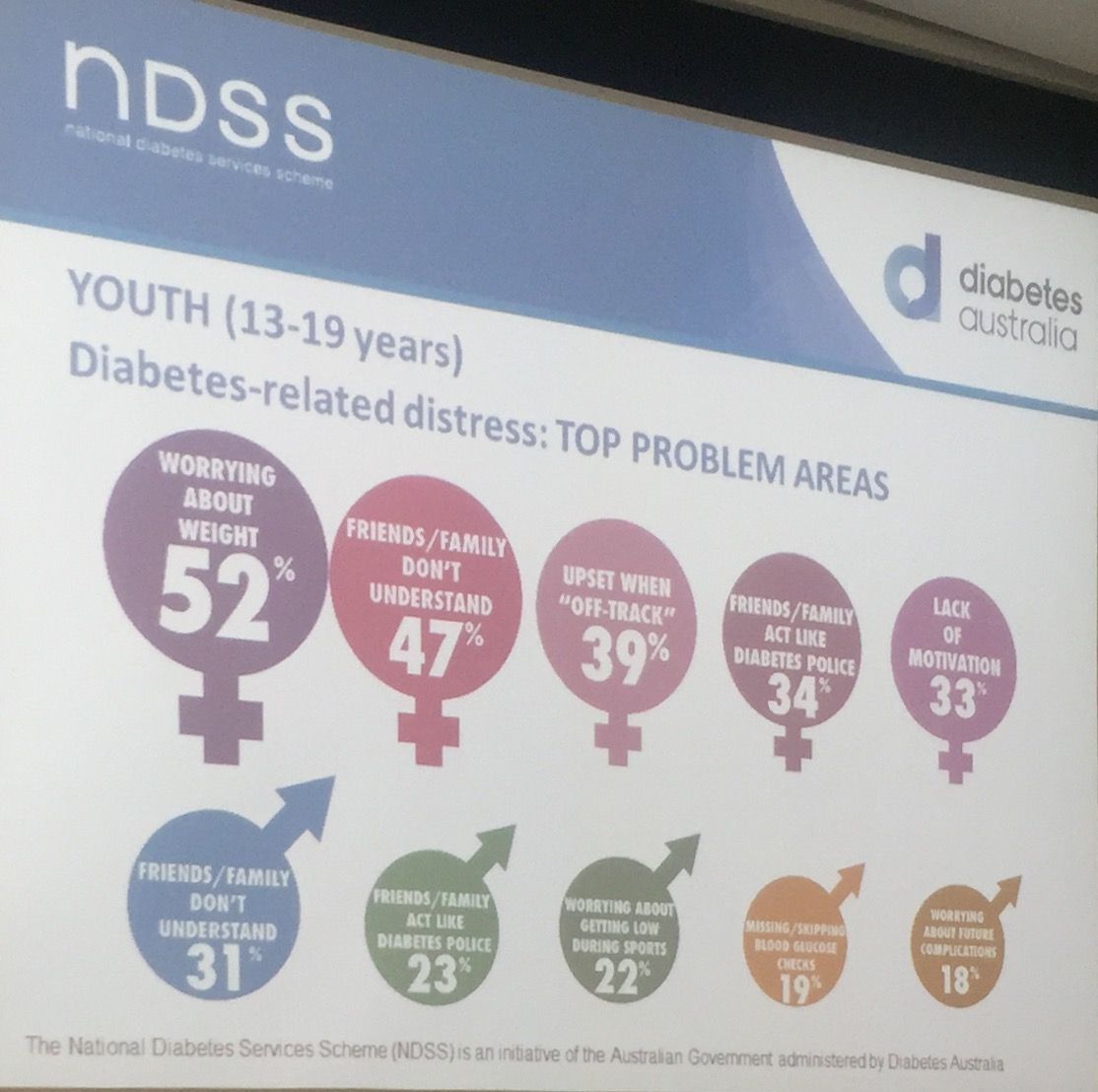
Today’s launch was incredibly powerful. Of course, we heard the statistics and heard how significant the problem is (a third of parents of children with diabetes reported impaired emotional well-being). And we heard about why this sort of work is important. But for me, and I suspect most people in attendance this morning, the most powerful moments were when we heard from Ryan Lange and Freya Wickenden, two young people living with diabetes. Both spoke beautifully about the role diabetes plays in their lives. Freya’s mum, Dallas, also spoke and shared some insights into parenting a child with diabetes.

As I said in my presentation at the launch – I can speak about this for hours and hours. I am a passionate advocate for all people with diabetes, but the vulnerability we see so often in young people with diabetes has meant that this has become a focus area of my work. But my words are insignificant and unimportant. It’s the words from young people living with diabetes that are central to understand what they are facing. Here is just some of what they told us.
The Diabetes MILES Youth report – was funded by the National Diabetes Services Scheme, and initiative of the Australian Government administered by Diabetes Australia. The study was conducted in collaboration with Australia Centre for Behavioural Research in Diabetes. The Diabetes MILES Youth project is part of the Young People with Diabetes National Diabetes Program for which I am Program Manager.
It’s fan girl here again. I want to talk more about Bill Polonsky’s talk at the ADA meeting – specifically this:
 This point had me thinking. A lot. We speak frequently about how diabetes is an invisible illness. And it is a lot of the time. This piece I wrote for The Glow last year really resonated with a lot of people with diabetes who thought that it was such a good representation of what life with diabetes is about that it was shared almost 4,000 times.
This point had me thinking. A lot. We speak frequently about how diabetes is an invisible illness. And it is a lot of the time. This piece I wrote for The Glow last year really resonated with a lot of people with diabetes who thought that it was such a good representation of what life with diabetes is about that it was shared almost 4,000 times.
It’s invisible – we can’t see it. We rarely point to it. And you can’t walk down the street identifying the people with diabetes. (Although I like to think we sparkle a little brighter than the average person and have an aura of brilliance surrounding us, a rainbow above our heads and ride around on a unicorn. Just me?)
But I’m not sure that as a person with diabetes that I have ever weighed up the management aspects of diabetes against the (for want of a better term) return on investment.
ROI is such a big thing in our world. We expect some sort of return or reward for work we put in. Whether it be in our friendships or relationships or work or play. We do something and there is an underlying need to see something come back at us. We seem to expect acknowledgement or compensation and pats on the back for what we have put in.
There’s a problem with that expectation when it comes to diabetes. Because sometimes it doesn’t matter how much effort we put into our diabetes, the ROI is negligible. Not always – sometimes we see results and we can point to our efforts for the improvements. But sometimes – and unfortunately, a lot of the time – we get nothing back.
That all makes so much sense, so I’m not sure why I have never seen that before. Bill Polonsky’s point was such an ‘Aha moment’ for me. I went away and kept thinking about it and started listing the reasons I give for eliminating self-care tasks of diabetes. And they all came down to versions of ‘Because it doesn’t matter what I do, I still get crap results.’
Is it an easy excuse? Maybe. But I ask those without diabetes this: how inclined would you be to keep doing something if you got nothing back in return? It’s why people leave jobs, or relationships or other situations. Not feeling that you are getting something in return for your work? You can walk away.
Of course, we can’t leave diabetes. So how do we keep going – keep up with the hassles of self-care – when the ROI can be so minimal. I don’t have the answers to that one, I’m afraid. I wish I did. I really do.
Throw back Thursday to this post from a few years ago with a meme – 30 Things About My Invisible Illness You May Not Know. Most of it is still applicable today.
One of the highlight sessions I sat in on at ADA was Dr William Polonsky. Bill is the Co-Founder and President of the Behavioural Diabetes Institute, which you can read all about here. He also wrote the book Diabetes Burnout which is on the shelves of many, many people living with diabetes. I refer to it ALL THE TIME, and my copy has become incredibly dog-eared and annotated in recent times. And there was a period of about 6 months where I carried it around with me like a security blanket. (If you don’t have it, you can order it here.)
I’ve seen Bill speak at other conferences I’ve attended – he is one of the speakers I always make a point to hear because he absolutely ‘gets’ diabetes. His talks are always informative, amusing and offer great take-home messages for the mainly-healthcare professional audience. And he is gentle, kind and completely and utterly non-judgemental.
Yes – I am a complete and utter fan girl! But I did manage to keep myself together when I spoke with him a couple of times at the conference. And only slightly squealed when I heard he would be coming to Australia later this year. (Watch this space!)
His session at this year ADA had the title ‘Caring for the patient who doesn’t seem to care’ and right off the bat, Dr Polonsky highlighted the word ‘seem’ in the title.
He started by asking the audience how many of them had, in the past year, seen a patient who didn’t seem to care about their diabetes. Just about every hand in the room went up. Of course they did. Because for many – most? all? – of us living with diabetes, there are times when it all gets too much and we seem to not care.
But then he reminded everyone that even those who seem to not care about their diabetes want to live long, happy, healthy lives.
I don’t know anyone with diabetes – feeling good or not so good about their management – who isn’t hoping to be healthy. No one wakes up in the morning and says they want to have a crappy diabetes day. No one says ‘Diabetes is too much for me at the moment. I hope I have a really bad hypo.’ No one.
In times of burnout, where I absolutely know it looks like I couldn’t give a toss about my health, I wish so hard that I could find ways to break through the exhaustion and lack of motivation and find a way – any way – to do better at managing my diabetes.
Other take home messages from Bill’s talk included the importance of talking about diabetes with a sense of urgency – however without threats. I loved how he suggested a reframing of the oft-quoted ‘diabetes is the leading cause of <insert complication>’, reminding us all of the following:
Dr Polonsky’s take home messages from this talk were many. He provided some strategies for what might work – and some that should be avoided.
I listen to talks like this and think they sound so logical and sensible, and wonder why it even needs to be said. But of course it does. Because sometimes – all too frequently – there is this idea that not managing diabetes as expected is a deliberate choice. Or that not getting the results that we all ‘should’ be getting is the fault of the person living with diabetes. Thank you to Dr Polonsky – and others like him, including Martha Furnell, Jill Weissberg-Benchell and our very own Professor Jane Speight – for understanding that there is no fault here. Just a need for better understanding and support.

Being a total fan girl here! Dr Polonsky is my hero.
I had a lovely dinner last night with a colleague and friend. We ate great food, drank terrific cocktails and didn’t shut up except for when the waiter was telling us the evening’s specials (and even then we ‘oohed’, ’aahed’ and ‘yummed’ our way through that).
At one point, my friend reminded me of a beautiful part of the book Captain Corelli’s Mandolin, a book I read when it first came out back in the mid-1990s.
As soon as I got home from our dinner, I searched for it so I could read the words again. Here they are:

When I first read the book, these words kind of washed over me. I was hearing them quoted a lot, and in the coming years I heard them read at weddings. They are beautiful words; read aloud it is beautiful prose.
But it wasn’t until last night that I read it and felt really understood it. The poem is an ode to enduring love, but that’s not what struck me. At least, not necessarily the love bit. But the endurance bit certainly did.
Over the last couple of years, things have been difficult. When I look at how I have been managing my diabetes, it has been a series of fits and starts. There are spurts of focus, then dips of almost denial. There are times of desperation and exhaustion and then periods of energy. It’s uneven. New devices see me get enthusiastic and motivated, but only for a short period. Then I return to the slump.
It’s not the exhilarating times that matter. Of course they are wonderful and enjoyable and sustaining and thrilling. Having a new pump or a new meter or a new CGM is a sure-fire way to get me thinking more about diabetes. But this doesn’t last. And it also doesn’t really count.
Equally, it’s not the slumps that matter.
What really matters is actually what you might call the boring times. It’s what comes before and after the flurry of interest of a new toy. Or the times around the ‘nosedives’. I feel best about my diabetes management not when I am stressed about how little I am doing or happy because I am so focused. It is actually the time when it is just there, plodding along, being considered at an ‘appropriate’ level. It’s not sexy. It’s not dramatic. But it’s so good because I feel relaxed and comfortable about it. It just is.
I am sure that there is something to be said about the fast-paced world we live in and this idea that we always need to be thrilled by something new. It’s too easy to get complacent and comfortable. That’s probably one of the reasons that I embrace new and emerging technologies with such zealousness.
However, if I was relying only on the new stuff to sustain me, it would never last. A new pump becomes just a pump very quickly. A new meter stops being new and shiny after a while and becomes just a meter. And a CGM may be magical and brilliant and life-changing until it become just another tool in the diabetes tool kit. That doesn’t make them any less important or valuable. But if I was relying on the excitement of the new, I would need a new toy every week or so!
The endurance of ‘just being’. That’s the sweet spot. That’s when I know I am getting it right. I just wish I could work out how to be there a whole lot more!
I am lucky that Aaron is always listening to new music. This CD was a recent purchase. Sometimes I hear something that makes me just so delighted. Like this live performance of my favourite track from the CD.
Today, I am at the Diabetes Victoria and Baker IDI Health Professional Symposium and the first session has me thinking – and sitting down the back of the auditorium banging out this post.
The keynote presenter for the Symposium is Professor Herzel Gerstein talking about hypoglycaemia. He made a wonderful point in the Q and A portion of his presentation, one that I think is frequently overlooked.

The language (yes, I’m talking language AGAIN) we use around hypoglycaemia is misleading at times. Generally, we have severe hypoglycaemia and mild hypoglycaemia.
Severe hypos refer to those we need assistance to treat. It may inolve unconsciousness or seizures. Severe hypos sometimes need paramedics’ assistance, or a trip to the hospital.
Mild hypos are those that we can manage ourselves without too much hassle.
The problem with using these two terms is that it makes it sounds as though mild hypos are nothing. They’re just a part of living with diabetes, deal with it, off you go.
That may be the case in practical terms. A so-called mild hypo may mean grabbing a handful of jelly beans, waiting a few minutes and then off you go. Or it might be slightly more than that and take longer. But whatever it is, it’s termed ‘mild’ because no assistance was required.
But the thing with ‘mild hypos’ is that they do have the potential to weed their way into your psyche and suddenly become very significant.
If those mild hypos mean that you are often running late for things, you start to wonder if others are questioning your reliability. If those mild hypos have you needing to sit things out for a moment, you worry your friends or your kids or your family think you are disengaged, not wanting to participate. If those mild hypos result in you being a little vague for a while in work meetings, you start to fear your boss or colleagues think that you are not paying attention, not interested, don’t understand.
These are not ‘mild’ things. These are really significant and mean worrying and stress and anxiety and anger and sadness and fear and guilt and all the other things that diabetes makes you feel. There is nothing mild about it!
I think this is a really important issue for healthcare professionals to remember. By brushing away mild hypos as just a short-term-complication-everyone-has-them notion, the actual impact on the person living with diabetes is ignored. it’s minimising just how big a deal mild hypos can be and not providing any strategies for coping and managing with the emotional side of these episodes.
A mild hypo may not necessarily be terrifying in the moment, it may be quite manageable at the time, it may not affect anyone else or draw too much, if any, attention to the person having the hypo. And this is good!
But don’t for a minute think that it doesn’t mean a silent feeling of dread (and possibly a silent word of thanks to the hypo gods that it was nothing more!) or feelings of significant distress afterwards.
This is my study.

It’s just one of the rooms in our home that is filled with books. There are books everywhere throughout our house. The front living room has shelves on either side of the fireplace and they are filled with our collection of music books. The kidlet has built-in floor to ceiling shelves in her room, almost completely full of her books – from her first board books to the books she is reading now. There are cookbooks on either side of the wood-fired stove in the kitchen and, in our bedroom, our bedside tables are piled high with books; another tower of books about New York is stacked on an antique cupboard; on the blanket box a pile of fashion books and illustrations sits, ready for a quick flick through.
I have a routine when I buy a new book. I open up the cover, and write my name and the month and year I bought (and usually then read) the book. This little tradition has provided me with a kind of living history of my reading habits.

New York-based (but raised in Melbourne) Lily Brett – one of my all-time favourite writers. I re-read this book just before we went to New York last year.
So with this life-long love of reading, it was with complete and utter confusion when, a couple of years ago, I found myself incapable of finishing a book. I would start a new book eagerly, and after a couple of chapters, I would stop. I found myself distracted, unable to concentrate. I would read the same paragraph over and over and lose track of what was happening. I couldn’t get a hold on the characters and was confused at the plot. I’d go to bed at night, anticipating reading a few chapters and then simply couldn’t focus. So I’d put the book down on the ever-increasing pile of half-read books on my bedside table. And not finish it, starting a new book, only for the same thing to happen.
I tried everything – pulling old favourites down from the shelves and trying to reread those. I tried different genres. I tried easy, brainless, fun chick-lit novels that didn’t take any real brain power or concentration to get through the enjoyable fluff. But I still could not make it through a whole book.
Instead, I would grab my iPad and mindlessly flick through social media sites, looking for and at I don’t know what. But whatever it was, it didn’t take attention. It didn’t take concentration. It didn’t take focus.
I was burnt out with reading. Just as I was burnt out with my diabetes. The lack of motivation I was experiencing when it came to managing my diabetes was flowing into other areas. I had never before lost the motivation to read and it was somewhat confusing and startling. I would buy new books but I stopped writing the date in the beginning of them because I knew that I would’t get through it and that the date would prove nothing.
It continued until the end of last year when I started to give a name to what was going on. I stopped making excuses for the burnout and tried to work through it; I looked at what else was going on and set up strategies to manage the situation.
Admittedly, these strategies haven’t worked on the diabetes burnout – it’s persisted (but I’m getting help for that now!) but naming it and owning it certainly did help in other areas.
And I started reading again.
Today, I’m back to the voracious, desperate reading that has been a character trait throughout my life. On sunny days, I can be found on the wooden bench under the front veranda, reading. As the days have gotten cooler, I am frequently curled up in front of the fire in our living room, or at the kitchen table, the room warmed with whatever is baking in the oven. I’ve been dealing with a relentless sinus-y cold the last week or so and have been taking myself off to bed to relax and read – even managing a couple of afternoon reading sessions followed by naps over the weekend.
I’m so glad I found my reading mojo! Being able to escape into a great book is one of life’s simple pleasures. One that I am enjoying once again.
Yesterday, as I sat in the waiting room to see my endo, I couldn’t help but feel that I was walking into a wasted appointment. I had seen her about six weeks earlier and left with promises to myself of being more engaged with my diabetes care. I promised I would have my blood work done. I thought about goals and how I could work to achieve them.
And yet, there I was, waiting to go in and wondering what the hell I had to say to her. There would be no discussion of lab results. I haven’t gone to pathology to have the checks done. There wouldn’t be any pulling out of data for me to show her – I hadn’t been logging anything. I was pretty much in the same state of mind about my diabetes as I had been last time I sat waiting to go in to see her.
I was wasting her time and I felt really bad about it. Not that she would ever tell me that. In fact, not that she would even be thinking that. But it’s how I felt. I have such respect for this endocrinologist, and I felt that in some ways I was actually being disrespectful in showing up so unprepared.
There were no tears yesterday. But there was an honest and open admission from me that I need help. I have tried everything I know to try and pull myself out of the motivation slump I have been in for so long. There are been periods where things seem to be better and I am able to make more of an effort, but they are fleeting and before long, I am back to feeling burnt out.
Let me be clear – I am not completely ignoring my diabetes. I am bolusing insulin at all the appropriate times; I check my blood sugar, albeit nowhere near as much as I know I need to – or that I would like to; I have started seeing my endo again. I eat well. At no time has diabetes completely fallen off the radar. But it certainly has deviated from being as much of a focus as I would like.
It’s not the mechanics of diabetes that is the problem. It is the trouble-shooting and problem solving and thinking about diabetes in a way that makes me feel confident that I am dealing with my health and wellbeing as much as my blood sugars. But I’m not doing that. I’m in a fog of burnout from which I now know I am unable to emerge without some real help.
I can pinpoint the source of the burnout; I can trace its progression; I can see why it happened. I understand all of that. I understand that dealing with the loss of our baby following a miscarriage and all the things that happened around it were often all I could deal with – both at the time and for periods since then too. But even though I have words to explain how this has happened, I don’t have actions to get me out of it.
I’ve tried. I’ve tried everything I could think of – all the techniques that have worked in the past. But I suspect that the combination of grief and the longevity of this burnout have resulted in me simply not being able to fix it alone. I need help.
I also believe that tied up in all of this is the way that I am feeling about my body and its failings. Because I do feel I have failed. Or at least my body failed me – again – when I miscarried. I really did think that I was ‘over’ it and was moving on, but not a day goes by where I don’t, in some way, feel sad and broken about it. I don’t know how to stop feeling this way. Again, I need help.
So, I asked for a referral to someone who can help me work though things – someone to help with strategies. I have been in therapy before; I know that it will help. It’s not a quick fix – I know that too.
I am trying to be all Pollyanna-ish about this and make grand ‘the first step is the hardest’ statements. And I am being positive and saying that it is certainly a step in the right direction. It’s going to take time. It’s going to take effort. Perhaps I am ready for that now. I know I certainly haven’t been to date. But maybe – hopefully – I am now.






