
You are currently browsing the category archive for the ‘Stigma’ category.
Imagine a community where people come together to make things happen. You don’t have to look far, really. Just look at the diabetes community!
Here’s something new from some folks (Jazz Sethi, me and Partha Kar) who are desperately trying to reshape the way diabetes is spoken about, and how fortunate I feel to have been involved in this project!

The thinking behind these particular language resources is to truly centre the person with diabetes when thinking about communication about the condition. In this series, we’ve highlighted three groups where we know (because these are the discussions we see in the diabetes community) language can sometimes be stigmatising and judgemental. This isn’t a finger-pointing exercise. Rather it’s an opportunity to highlight how to make sure that the words, images, body language – all communication – doesn’t impact negatively on people with diabetes.
A massive thanks to Jazz and Partha. Working together, and with the community, to create and get these out there has been a joy. (As was sneaking into the ATTD Exhibition Hall before opening time so we could get a coffee and find a comfortable seat to work before the crowds made their way in!) And a super extra special nod to Jazz who pulled together the design and made our words look so bright pretty! And a super, super, super special thanks to Jazz for designing my new logo which is getting its first run on the back of these guides.
You can access these and share directly from the Language Matters Diabetes website. These don’t belong to anyone other than the diabetes community, so please reach out if you would like to provide any commentary or be involved in future efforts. There’s always more to do!

On Sunday, one of those annoying diabetes things happened – a kinked insulin pump cannula, subsequent high glucose levels followed by a little glucose wrangling tango where, instead of rage blousing, I tried to gently guide my numbers back in-range. I thought about how frustrating diabetes can be – unfairly throwing curve balls at us even when we are doing ‘all the right things’. And so, I used this little story for a post on LinkedIn to illustrate why I am so dedicated to making sure that stories like this are heard and lived experience is centred in all diabetes conversations.
Meanwhile, anyone who has even the barest of little toes dipped in the water of the diabetes community would have heard about Alexander Zverev being told by French Open officials that he was not permitted to take his insulin on court. He was expected to inject off court and, according to Zverev, was told ‘looks weird when I [inject] on court’. Insulin breaks would be considered as toilet breaks.
What’s the connection between this story and my LinkedIn story? Absolutely none. Except there kind of is.
I’m not about to write about sports or try to connect my story with that of a top-ranking tennis player. That would be totally out of my lane. (The couple of years of tennis I took when I was in grades five and six give me no insight into life of a tennis player.)
However, when it comes to discussing diabetes and the stigma surrounding it, I’m definitely in my lane. I understand and am very well-versed when it comes to talking about the image problem diabetes faces and how that fuels the stigma fire.
The response from the diabetes community when the Zverev story broke. Most people were incredibly supportive of the tennis player and rightfully indignant of the incident. JDRF UK responded swiftly with an open letter to the French Open organisers, eloquently highlighting why their ruling needed to be changed. And changed it was.
My LinkedIn post was shared a few times and there were comments from people saying that these stories help others better understand our daily challenges and work to cut through a lot of the misconceptions about diabetes.
And then there was this direct message:
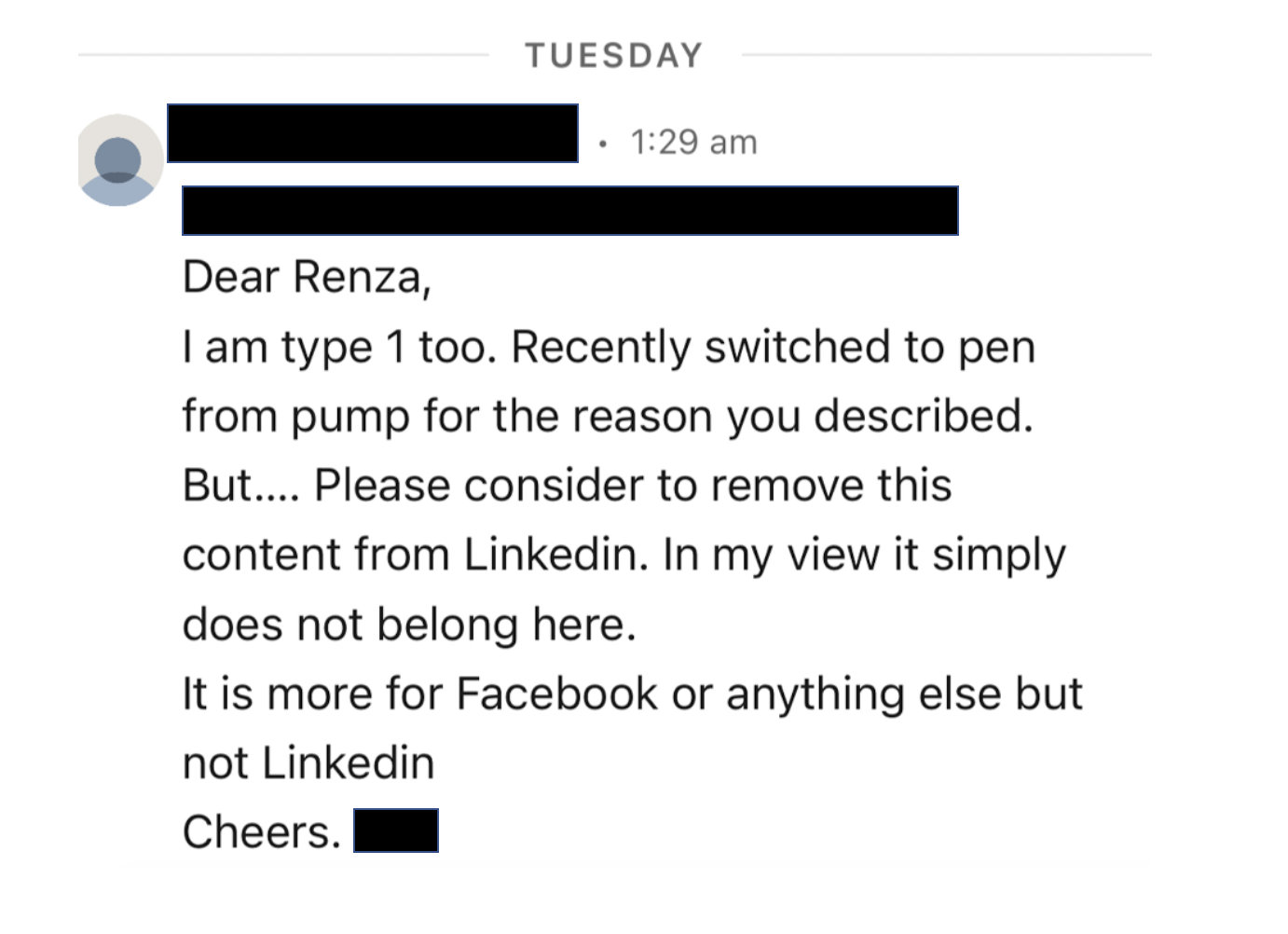
I bristled as I read it. My initial response was ‘How dare this man try to tell me what I can and can’t post on LinkedIn. Who is he to tell me what I can and can’t share?’ I snapped a reply back to him where I pointed out: ‘…I am a diabetes advocate, working to change attitudes and raise awareness about living with diabetes. My post belongs here on LinkedIn as it very much aligns with the work I do.’
But I haven’t been able to stop thinking about it because as problematic as it is for someone trying to silence what people with diabetes share online, there was more that was troubling me.
The idea that diabetes is a topic only appropriate in certain contexts and should be hidden away from others reinforces shame. Suggesting work settings are not the place to talk diabetes plants that seed that diabetes, and people with diabetes, could be liabilities in the workplace. Talking about diabetes on LinkedIn – a platform for business and workplace networking – is relevant because people with diabetes exist in business and workplaces, and the reality is that diabetes sometimes interferes with our work. Which is perfectly okay. Last week, I needed to refill my pump during a meeting. So, I let others on the call know what I was doing and carried on. On another day, I was recording a short video about a research program and after take 224 realised I needed to treat a hypo and did so. I shouldn’t need to feel that these aspects of daily life with diabetes are only allowed to happen out of view.
Essentially, this is what Alexander Zverev was being asked to do at his workplace: hide away when he needed to perform a task that keeps him alive, as if there is something shameful and disgusting about it. In my mind, this top ranked tennis player playing in a Grand Slam competition should be commended. I mean, any tennis player who does that is remarkable. Zverev does it and then goes about performing the duties of a pancreas. His opponents don’t have to do that! Their pancreas doses out the perfect amount of insulin without any help. Talk about an unfair advantage!
Not everyone wants to talk diabetes with others and that’s fine. But those of us who are happy to speak about and ‘do diabetes’ wherever we are shouldn’t feel that we are doing anything wrong. Diabetes stigma exists because there are so many wrong attitudes about diabetes. It’s insidious and it’s damaging. It erects barriers creating a climate of shame and perpetuates misconceptions that lead to ignorance. And it pressures us to hide away the realities of diabetes, as if there is something to be ashamed of. But there is nothing shameful about living with diabetes. There is nothing shameful about injecting insulin on Centre Court at Roland-Garros, or sharing frustrations on LinkedIn. Or anywhere else. Diabetes has a place wherever your workplace might be. Stigma, however, does not.

I woke up (at 4am thanks to a hypo, but that’s another story all together) and scrolled through a variety of social media feeds and, because I seem to follow a lot of diabetes-related pages and people, was bombarded with the below. And so, these are my very early morning musings, a stream of consciousness mess, the logic and rationality of which is most likely influenced by low blood sugar. (The typos, however, are all mine.)
So, let me begin by saying that this is important work – of course it is. The DiRECT trial has really put the idea of diabetes remission on the research agenda, encouraging further research into the issue, provided another potential diabetes treatment option for people with type 2 diabetes, and supporting people with type 2 diabetes looking at this way of managing their diabetes. Choice. It’s a good thing!
Today we have some follow up data (after the initial two years of the trial), providing updates on how research participants are going. Again. It’s important research, and it is helping increase knowledge and understanding of type 2 diabetes. Good stuff!
But one of the things I am all about is accuracy in reporting and this, my friends, isn’t it.
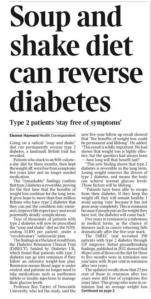
I wasn’t going to even touch the heading of the article, because surely the inaccuracy of it doesn’t need highlighting at all, but let’s go there anyone. The DiRECT trial is researching people with type 2 diabetes, and it probably would be good to mention that. I guess that nugget is in the sub-heading, but it might be good to not relegate it there.
But let’s look at that sub-heading. ‘Stay free of symptoms’ is an interesting thing to highlight when we know that in many cases, people with undiagnosed T2D don’t have any symptoms anyway. Surely focusing on what it means in terms of day-to-day life with diabetes (i.e. medication, monitoring requirements, daily burden of ‘doing diabetes’, frequency of HCP visits) would be more meaningful.
Back to the heading and we have the word reverse which is pretty much incorrect in all ways possible. The word they’re looking for is remission. Why? Because even if the result from those in the study is that they don’t require diabetes meds, and their glucose levels are back in range, they still do have diabetes.
I’m not a statistics person. Data hurts my head and numbers make me cry, and I get the complete and utter irony of saying that considering that I live with a condition that depends on me understanding data and numbers, but now is not the time to come at me and my 2.9mmol/l self. Please and thank you.
But there is a number in this research that seems to be jumping out at me and it’s this number: 23%. Let me clarify (this is from the Diabetes UK press release): 23% of participants who were in remission from type 2 diabetes at two years in the original trial remained in remission at five years.
It’s important to also point out that this isn’t 23% of the total people who started in the DiRECT trial five years ago – not all participants were in remission after two years. At two years, 36% remained in remission. Or 53 out of the original 149 research participants in the intervention group (plus a additional 5 people in the control group).
So that 23% is of 58 people who remain in remission now at five years. That’s 13 people. Or about 8% of the starting number. That’s a very different story to what is being presented in news stories, media releases and cross socials today, isn’t it?
And that matters. Big time. Because there is real danger that many people will read the media reports today and in their minds that will mean that remission from type 2 diabetes is a far more likely outcome than reality and is the likely outcome for everyone.
I’m not here to argue whether remission is a thing or not – it is. FOR SOME PEOPLE with type 2 diabetes. Adding pieces to help understanding of the giant puzzle that is diabetes is brilliant for everyone. Research helps us do that. Sharing that research so that people living with diabetes better understand the options available and learn more about how our particular brand of diabetes works is gold!
But I am here to argue that publishing grand sweeping statements about how to ‘reverse’ type 2 diabetes, or telling only part of the story about the research, without the necessary nuance, is inaccurate and will further stigmatise type 2 diabetes and those living with it, especially those who are not able to achieve remission of their condition. The very idea that they could be made to feel that they are not trying hard enough or that they have failed is not being sensationalist.
The stigma associated with type 2 diabetes is considerable and everyone has a responsibility to making it better and not add to it. And surely an even heavier burden of that should fall to those who are working in diabetes. If my 4am, glucose-starved brain is able to grasp how stigmatising something like this could be to people with type 2 diabetes, then it should be glaringly obvious to anyone who has even a passing interest in the condition.
Throughout ATTD I got to repeatedly tell an origin story that led us to this year’s #dedoc° symposium. I’ve told the story here before, but I’m going to again for anyone new, or anyone who is after a refresher.
It’s 2015 and EASD in Stockholm. A group of people with diabetes are crowded together in the overheated backroom of a cafe in the centre of the city. Organising and leading this catch up is Bastian Hauck who, just a few years earlier, brought people from the german-based diabetes community together online (in tweet chats) and for in person events. His idea here was that anyone with diabetes, or connected to the conference, from anywhere in the world, could pop in and share what they were up to that was benefitting their corner of the diabetes world. I’ll add that this was a slightly turbulent time in some parts of the DOC in Europe. Local online communities were feeling the effects of some bitter rifts. #docday° wasn’t about that, and it wasn’t about where you were from either. It was about providing a platform for people with diabetes to network and share and give and get support.
And that’s exactly what happened. Honestly, I can’t remember all that much of what was spoken about. I do remember diabetes advocate from Sweden, Josephine, unabashedly stripping down to her underwear to show off the latest AnnaPS designs – a range of clothing created especially to comfortably and conveniently house diabetes devices. It won’t come as a surprise to many people that I spoke about language and communication, and the work Diabetes Australia was doing in this space and how it was the diabetes community that was helping spread the word.
I also remember the cardamom buns speckled with sugar pearls, but this is not relevant to the story, and purely serving as a reminder to find a recipe and make some.
So there we were, far away from the actual conference (because most of the advocates who were there didn’t have registration badges to get in), and very separate from where the HCPs were talking about … well … talking about us.
Twelve months later EASD moved to Munich. This time, Bastian had managed to negotiate with the event organisers for a room at the conference centre. Most of the advocates who were there for other satellite events had secured registrations badges, and could easily access all spaces. Now, instead of needing to schlep across town to meet, we had a dedicated space for a couple of hours. It also means that HCPs could pop into the event in between sessions. And a few did!
This has been the model for #docday° at EASD and, more recently, ATTD as well. The meetups were held at the conference centre and each time the number of HCPs would grow. It worked! Until, of course COVID threw a spanner in all the diabetes conference works. And so, we moved online to virtual gatherings which turned out to be quite amazing as it opened up the floor to a lot of advocates who ordinarily might not be able to access the meetings in Europe.
And that brings us to this year. The first large international diabetes conference was back on – after a couple of reschedules and location changes. And with it would, of course, be the global #dedoc° community, but this time, rather than a satellite or adjacent session, it would be part of the scientific program. There on the website was the first ever #dedoc° symposium. This was (is!) HUGE! It marks a real change in how and where people with diabetes, our stories and our position is considered at what has in the past been the domain of health professionals and researchers.
When you live by the motto ‘Nothing about us without us’ this is a very comfortable place to be. Bastian and the #dedoc° team and supporters had moved the needle, and shown that people with diabetes can be incorporated into these conferences with ease. The program for the session was determined by what have been key discussions in the diabetes community for some time: access, stigma and DIY technologies. And guess what? Those very topics were also mentioned by HCPs in other sessions.
There have been well over a dozen #docday° events now. There has been conversation after conversation after conversation about how to better include people with diabetes in these sorts of events in a meaningful way. There has been community working together to make it happen. And here we are.
For the record, the room was full to overflowing. And the vast majority of the people there were not people with diabetes. Healthcare professionals and researchers made the conscious decision to walk into Hall 118 at 3pm on Wednesday 27 April to hear from the diabetes community; to learn from the diabetes community.
If you missed it, here it is! The other amazing thing about this Symposium was that, unlike all other sessions, it wasn’t only open to people who had registered for ATTD. It was live streamed across #dedoc° socials and is available now for anyone to watch on demand. So, watch now! It was such an honour to be asked to moderate this session and to be able to present the three incredibly speakers from the diabetes community. Right where they – where we – belong.
DISCLOSURE
My flights and accommodation have been covered by #dedoc°, where I have been an advisor for a number of years, and am now working with them as Head of Advocacy.
Thanks to ATTD for providing me with a press pass to attend the conference.
Gosh, it’s been a hot minute since I last did one of these. The whole point of Interweb Jumble posts on Diabetogenic is to highlight anything that has caught my interest in the online diabetes world, write about initiatives I’ve been involved in, and, most importantly, to elevate the great work being done by others living with diabetes. Building folks up and promoting their amazing efforts has been at the heart of what I do, so I’m always happy to share what others are doing.
Grab a coffee, tea or shandy, (Don’t. Don’t grab a shandy), and read on.
Diabetes Chat
YES!! There is a new place to congregate online, in a different format, and with this one, you get to hear people’s voices. (Sorry to everyone who had to endure my 7am Aussie accent last Tuesday!). This is a new initiative that’s been set up by three DOC folks – Tom from the UK, and Chris and Sarah from the US, utilising a new feature on Twitter called Spaces. It’s a terrific way to host an online peer meeting, creating yet another time and place that is BY people with diabetes, FOR people with diabetes. There is a weekly guest who gets put through their paces with terrific questions from the hosts and those listening in, and an open mic chat time as well.
It’s super impressive to see people from all over the globe participating. It reminds me a little of the DSMA tweetchats which are very welcoming and open to all, regardless of where you live around the world.
Search #DiabetesChat on Twitter for more.
dStigmatize
The team at diaTribe has once again tapped into one of the important issues, and much spoken about topics in the diabetes community and developed a terrific new website addressing diabetes stigma. It’s called dStigmatize and you can find it here.
I’m delighted to see Diabetes Australia’s work on stigma and language highlighted so prominently on the site (disclosure: I work at Diabetes Australia and have been involved in this work), including the videos from last year’s Australian National Diabetes Week campaign, which have been viewed hundreds of thousands of times.

Seasons of…diagnosis
New research out of Finland asked if more people were diagnosed with type 1 diabetes during colder months. You can read the paper here.
And a discussion on Twitter about it here.
HypoRESOLVE podcast
The HypoRESOLVE comms team created a new podcast to showcase the incredible work of this researchers involved in the project, with a strong emphasis on how people with diabetes are involved in the project. I was delighted to host this podcast and speak with some truly remarkable clinicians and researchers as well as other people with diabetes who are on the projects Patient Advisory Committee. (Disclosure – I am on the HypoRESOLVE PAC. PAC members are now paid an honorarium for our time working on this project, however we were not at the time of recording or working on this podcast.)
Here is the most recent episode (on Spotify).
Better engagement with PWD = better services
Great paper from a team out of the UK looking at how connecting with the lived experience expertise of people with diabetes, health professionals and diabetes health services can improve service delivery.
One of the co-authors is one of the GBdoc OG, Laura (@Ninjabetic1 on Twitter), and it’s great to see her name back in the diabetes world, contributing to this important discussion.
And the DDA podcast…
The Danish Diabetes Academy developed a podcast out of their Winter School that featured Postdocs who had participated in the academy speaking with others in the diabetes world to discuss who academic researchers work to ensure their research reaches and benefits those they are researching. I was so honoured to be invited to be interviewed for their first episode and answered questions about how communication is important when engaging people with diabetes to be part of the research process. You can listen here.
Language Matters for Portuguese speaking friends with diabetes!
The latest in the Diabetes #LanguageMatters stable is this document out of Brazil. Always terrific to see more and more statements coming out, highlighting the importance of language and communication in diabetes.
Thinking of starting on an insulin pump?
If so, the awesome Grainne at Blood Sugar Trampoline has you covered with this post. It is truly one of the most measured pieces I’ve read about things to consider if you are on the path to starting an insulin pump. The gushiness and superlatives that many of us resort to when banging on about how much we love our pumps are replaced with sensible, and practical advice and suggestions. If this is where you’re thinking of taking your diabetes management, Grainne’s piece is a must read.
Who doesn’t want to come to ATTD!?
#dedoc° voices is back and heading to ATTD in April this year, and applications are still open if you would like to be considered as part of the program. Successful applicants will be granted access to the entire ATTD program, giving them an opportunity to share what they see and learn with their networks. Make your submission count – this is a competitive process and success is more likely for those who take the time to provide details of how they will be involved in the program. Details here.
(Disclosure: I am an advisor to the #dedoc° voices program. I do not receive any payment for this role.)

World Health Organisation
In March, the World Health Organisation, through the Global Diabetes Compact, is hosting a two-day focus group for people with lived experience of diabetes. If you’re interested in getting involved, there is an expression of interest process you can complete here.
Also from WHO is this survey which is asking people with diabetes how to improve messaging and communication. You only have until 28 Feb, so get onto it now! (Disclosure: I was a volunteer consultant in the development of this survey)
Massive kudos to the Global Diabetes Compact team who are doing an absolutely stellar job engaging with the community. Always so terrific to see!
A diabetes sea shanty…
You’re welcome.
(Follow @TypeWonDiabetes on Instagram here.)
People with diabetes and their involvement in research
An end of year delight was this article that I co-authored making it to publication. The article is about how to better involve people with health conditions in research (which really seems to be something I’ve been very focussed on recently!).
Spare a Rose – last push
February still has a last few days which means that Spare a Rose isn’t over yet. You can still donate and contribute to this year’s total and support people with diabetes in under-resourced countries through the Insulin for Life program.

A week out from National Diabetes Week, and this piece has been sitting in my ‘to be published’ folder, just waiting. But the post-NDW exhaustion coupled with lockdown exhaustion, plus wanting to make sure that all my thoughts are lined up have meant that I haven’t hit the go button.
In the lead up to NDW I wrote this piece for the Diabetes Australia website. That piece was a mea culpa, acknowledging my own contribution to diabetes-related stigma and owning it. I also stand by my thoughts that the stigma from within the community is very real and does happen.
But what I didn’t address is just where that stigma comes from. Those biases that many people with type 1 diabetes (and those directly affected by it) have towards type 2 diabetes come from somewhere, and in a lot of cases that is the same place where the general community’s bias about diabetes comes from. It is all very well for us to expect people with type 1 diabetes to do better, but I’m not sure that is necessarily fair. I think that we should have the same expectations of everyone when it comes to stamping out stigma.
And so, to the source of stigma and, as I’ve said before, it comes from lots of places. As someone who has spent the last twenty years working in diabetes organisations, I know that the messaging my orgs like (and including) those that have paid my weekly salary has been problematic. I still am haunted by the ‘scary’ campaign from a few years ago that involved spiders, clowns, and sharks. (If you don’t remember that campaign, good. If you do, therapy works.)
For me personally, I don’t think much stigma I have faced has come at the hands of other PWD. Sure, there’s the low carb nutters who seem to have featured far too frequently on my stigma radar, however, the most common source of stigma has undoubtedly been HCPs.
It’s not just me who has had this experience. The majority of what I have seen online as a response to experiences about stigma involves heartbreaking tales of PWDs’ encounters with their HCPs.
While I will call out nastiness at every corner, and no stigma is good stigma, it must be said that there is a particular harm that comes when the origin of the stigma is the very people charged to help us. Walking into a health professional appointment feeling overwhelmed, scared, and frustrated only to leave still feeling those things, but with added judgement, shame and guilt is detrimental to any endeavours to live well with diabetes. In fact, the most likely outcome of repeated, or even singular, experiences like that is to simply not go back. And who could criticise that reaction, really? Why would anyone continually put themselves in a situation where they feel that way? I wouldn’t. I know that because I didn’t.
It’s one thing to see a crappy joke from a comedian who thinks they’re being brilliantly original (they never are) or the mundane, and almost expected, ‘diabetes on a plate’ throwaway line in a cooking show, but while these incidents can be damaging, they are very different to having stigmatising comments and behaviours directed at an individual as is often the case when it is from a HCP.
Of course, HCPs aren’t immune to the bias that forms negative ideas and opinions about diabetes. In the same way that people with type 1 diabetes form these biases because those misconceptions are prevalent in the community, HCPs see them too. Remember this slide that I shared from a conference presentation?
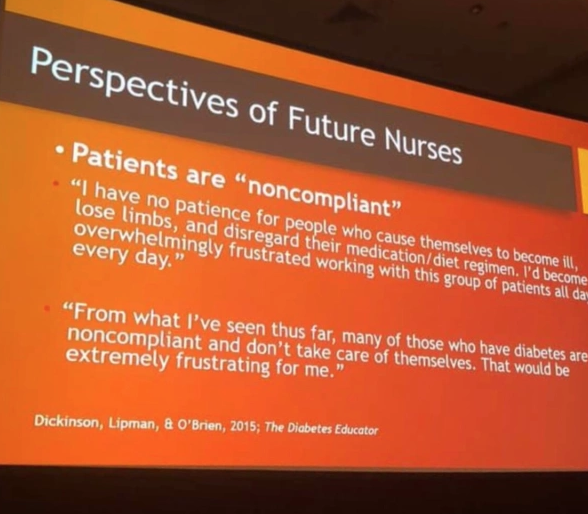
This came from student nurses. Just think about that. Students who were training to be HCPs who would inevitably be working with people with diabetes. A I wrote at the time:
‘They hadn’t even set foot on the wards yet as qualified HCPs. But somehow, their perceptions of people with diabetes were already negative, and so full of bias. Already, they have a seed planted that is going to grow into a huge tree of blaming and shaming. And the people they are trusted to help will be made to feel at fault and as though they deserve whatever comes their way.’
Is it any wonder that, with these attitudes seemingly welded on, that people with diabetes are experience stigma at the hands of their HCPs?
The impetus can’t only be on PWD to call this out. And the calls to fix stigma can’t exclusively rest on the shoulders of PWD – we already have a lot of weight there! It must come from HCPs as well – especially as there is such a problem with this group. Perhaps the first step is to see real acknowledgement from this group of their role here – a mea culpa from professional bodies and individuals alike. Recognising that no one is immune to the bias is a good step. Owning that bias is another. And then doing something about it – something meaningful – is how we make things better for people with diabetes. I really hope we see that happening.
More about this:
Becoming an ally – how HCPs can show they’re really on our side.
Ask a group of people with diabetes about their experiences of stigma, and for examples of the sorts of things they’ve heard and before long you’ll be able to compile a top ten list of the most commonly heard misconceptions that have contributed to diabetes having an image problem. When I’ve asked about this recently, the main perpetrators of these seemed to be healthcare professionals. More on that later this week.
This year, in the Diabetes Australia National Diabetes Week campaign about diabetes-related stigma, two videos have been produced and they’re almost like a highlight reel of some of the stigmatising things people with diabetes hear.
Let me tell you something I found really interesting. As part of the testing of these, I showed them to a heap of people with diabetes and a heap of people without diabetes. The reaction from people with diabetes varied from sadness (including tears), to anger and frustration, and mostly, recognition in everything they saw.
The reaction from a number of people without diabetes was disbelief that this really happens. They simply couldn’t believe that people would be so insensitive; so cruel, so shaming.
However, for so many people with diabetes, this is our reality.
Here’s one of the two videos we produced. (You can watch the second one here.) Already, this is being shared widely in our own diabetes community. I’ve lost count of the places online I’ve seen this shared. Keep doing so, if you can. Because clearly, we need to get the message out to those without diabetes so they understand that not only is this sort of stigmatising behaviour harmful, but it is also horribly common. And it needs to stop.
DISCLOSURE
I work for Diabetes Australia, and I have been involved in the development of the Heads Up on Diabetes campaign. I’ve not been asked to share this – doing so of my volition, because I think the messaging is spot on. The words here are my own, and have not been reviewed prior to publication.
I don’t know too many people living with diabetes who haven’t experienced stigma. I know I certainly have. In twenty-three years of living with diabetes, it’s come from all directions: the media, healthcare professionals, work colleagues and even family and friends. That’s because people outside the diabetes community often have pre-conceived ideas about what diabetes is all about, and a lot of those ideas are plain wrong.
But stigma doesn’t only come from outside the community. In fact, for some people with diabetes, some of the most harmful and hurtful experiences of stigma has actually come from other people with, or affected by, diabetes. [Click here to read more…]

DISCLOSURE
This piece was published today on the Diabetes Australia website, and I wrote it as part of the organisation’s National Diabetes Week campaign on diabetes stigma. I work for Diabetes Australia, and am sharing this because I’ve chosen to – not because I’ve been asked to. The words here are my own, and perhaps the only thing missing from the published text is some of the decorative language I often use when speaking about diabetes-related stigma. Bottom line – all stigma sucks. Let’s #EndDiabetesStigma now.
Gosh, I love baking a cake! It’s excellent therapy, super relaxing and is one of my favourite stress busters. I can pretty much guarantee to turn out something that not only looks Instagram-pretty but will also taste divine. I’ve written before that one of the reasons I love baking so much is because it is the exact opposite of diabetes: I know precisely what I’m going to get when I follow the steps of the recipe, and know enough that when I’m making things up as I go along what works, what doesn’t and what will yield the best results. Which is the polar opposite of diabetes, where following a ‘recipe’ guarantees nothing but confusion, frustration, and a completely different result to yesterday, and making it up can mean winding up with a rollercoaster or a straight line on the CGM. No one knows. It’s a mystery. It makes no sense to anyone.

Next week is National Diabetes Week here in Australia, and focus is going to be on diabetes-related stigma. I’ve spent a lot of time in recent weeks involved in the preparation of our campaign, listening to people with diabetes share their stories. You can check out this post on the Diabetes Australia Facebook page to see people sharing some examples of stigma they’ve experienced. It’s heartbreaking. It shouldn’t be happening.
I am very conscious that in the past I’ve probably contributed to stigma associated with type 2 diabetes. I’m horrified by it, and ashamed. I should have known better, and maybe if I’d bothered to learn from people with type 2 diabetes, I would have been more sensitive. When we blame and shame diabetes, we are blaming and shaming real people living with diabetes. I seemed to have forgotten that when I thought it was okay to demand that my diabetes was seen as the more serious diabetes, and that people make sure that they get my type of diabetes right.
And that brings me back to my cakes. And cakes in general. And comments about cakes. Especially comments about cakes being ‘diabetes on a plate’. They’re not. We all know that, right? And we all know that they are not any type of diabetes on a plate. Right?

And we know that when some idiot on a cooking show refers to a delectable, rich dessert as ‘diabetes on a plate’ that demanding clarification about ‘WhAt TyPe Of dIaBeTeS yOu MeAn’ is only contributing to the stigma. Right?
Right?
Stigma sucks. It really does. It makes people just want to curl up and hide from others, and hide their diabetes. It makes people feel ashamed and guilty and, really, that’s just not fun at all.
We don’t all need to love each other in the diabetes world – god knows that there are people who steer clear of me, and I am more than happy to return that favour – and we don’t need to align our advocacy efforts. But maybe we can all agree that all stigma associated with any type of diabetes is pretty nasty. That actually seems like a pretty simple thing upon which to agree.

That time I wrote about this (and then a HCP misread it as me saying PWD don’t need to know what type of diabetes they have. It doesn’t say that…)
That time I owned my own shitty behaviour.
That time I wrote about how heavy diabetes stigma is.







