
You are currently browsing the category archive for the ‘Hypo’ category.
I’ve been unwell.
And so, I’ve had time to think. Mind you, I’ve found it difficult to form thoughts properly, thanks to the brain fog that is impacting my attention span and ability to think things through to a conclus…oh look! The leaves on the trees in the garden are changing. I should buy the last plums when I go to the fruit and veg shop, and bake a plum cake. That would be delici… Are mandarins in season yet? Ooh, a puppy!
Anyway, back to trying to focus on what I’ve been randomly and messily thinking about.
On my last day at ATTD in Amsterdam, I wound up with a very weird pain flare that meant I could barely move. I put two and two together, came up with the wrong answer and decided it was thanks to arthritis and spent the day before my flight desperately trying to sleep it off so I would be okay to navigate Schiphol Airport and get myself home. I did make it home, but not without wheelchair assistance at each airport, and in excruciating pain for the entire long trip home.
Turns out, it wasn’t arthritis. It also wasn’t diabetes, but that didn’t stop me from trying to connect non-existent dots.
The day before the paralysing pain flare, I woke at 3am with my Dex alarm wailing. I was low. Very low. For five hours. You know, one of those lows that just won’t quit. One of those lows that simply won’t respond to massive quantities of glucose. I ended up throwing up after force feeding myself jellybeans and guzzling juice from the minibar, which was all just lovely. (And yes – I realised I had some inhalable glucagon with me AFTER the fact … but in my low fog, forgot as I was just trying to stay alive with sugar.)
Of course, I was exhausted when I finally came back in range and felt like I’d been hit by a truck. But sure enough, I got up and had a frantic day at the conference centre, in meetings, giving talks and trying to appear functional while feeling absolutely wrecked.
The next day, when I woke up unable to move because I was in pain, I thought that perhaps it was a result of overdoing things the day before, when I should have perhaps taken the morning off to recover from the hypo and the exhaustion that came with it. But of course I didn’t. Because when have I ever taken time off for diabetes? One time I had an evening black out hypo in a park requiring paramedic attention and I was in at work at my desk by 8.30am the next day. Because why wouldn’t I be? My weird and illogical attitude is that if I was to take time off to recover every time diabetes doesn’t play nicely, I’d be taking hours off each week. No one has time for that. At least, I certainly don’t.
And how very messed up that thinking is. I realise that. And I know what I say to friends with diabetes who tell me about their particularly crappy hypos, or when diabetes is kicking their arse/ass: ‘Take the time and let your body rest,’ I’ll say. ‘You’ve just been dealt a pretty shitty blow to your body and mind. Don’t overdo it,’ I’ll remind them.
And what do they do? They don’t rest. They don’t listen to their body. They overdo it. It’s what we do.
It’s messed up and we keep doing it, even though we know better. Of course we know better: because we give good advice to others. But we then do that ridiculous thing where we think resilience is strength, where actually, resilience would be listening to what our bodies need and then doing it. We ignore symptoms and give ourselves imaginary gold stars for ‘pushing through’.
It took some weird virus that literally hampered my ability to walk for me to take time off work. Sleeping 20 hours a day was all I could manage. But you know what? I should have slept 20 hours the day after the five-hour low to recover too, but of course I didn’t.
Who am I trying to impress by soldiering on as though there’s nothing wrong? What am I trying to prove? Do I think we get extra points in some bizarre Hunger Games-like challenge? Is it that I worry what others will think of me if I say, ‘I need to stop for a bit’? Am I afraid of seeming weak? Lazy? Or am I – twenty-seven years later – trying to live up to the ‘diabetes doesn’t change anything’ line I was fed the day I was diagnosed, even though it changes everything?
I’ve been back home now for two weeks now and really just getting back to regular programming now. On Sunday I was able to stand up for long enough to bake a cake. That was a win. I also was able to walk to our local café – a five-minute walk away – but needed a lift home. Slowly, but definitely better.
I’m not pushing myself – partly because I can’t, but also because I refuse to and that is something that is very weird for me. I’m home this week instead of flying to Bangkok to speak at the IDF Congress – the first time I have ever cancelled a work trip. Usually I push through. Usually I suck it up and pretend all is fine. Because I drank the ‘diabetes-won’t-stop-me’ Kool Aid when instead, I should have recognised that there is no shame in stopping to rest. I need to be better and do better about this. And listen to the advice I would give everyone else. Permission to take time out for diabetes.
This post is dedicated to my darling friend and #dedoc° colleague Jean who also doesn’t know when to stop. Let this be a reminder to put down the Kool Aid!

So often, there is amazing work being done in the diabetes world that is driven by or involves people with lived experience. Often, this is done in a volunteer capacity – although when we are working with organisations, I hope (and expect) that community members are remunerated for their time and expertise. Of course, there are a lot of organisations also doing some great work – especially those that link closely with people with diabetes through deliberate and meaningful community engagement.
Here are just a few things that involve community members that you can get involved in!
AID access – the time is now!
It’s National Diabetes Week in Australia and if you’ve been following along, you’ll have seen that technology access is very much on the agenda. I’m thrilled that the work I’ve been involved in around AID access (in particular fixing access to insulin pumps in Australia) has gained momentum and put the issue very firmly on the national advocacy agenda, which was one of the aims of the group when we first started working together. Now, we have a Consensus Statement endorsed by community members and all major Australian diabetes organisations, a key recommendation in the recently released Parliamentary Diabetes Inquiry and widening awareness of the issue. But we’re not done – there’s still more to do. Last week I wrote about how now we need the community to continue their involvement and make some noise about the issue. This update provides details of what to do next.
And to quickly show your support, sign the petition here.
Language Matters pregnancy
Earlier this week we saw the launch of a new online survey about the experiences of people with diabetes before, during and after pregnancy, specifically the language and communication used around and to them. Language ALWAYS matters and it doesn’t take much effort to learn from people with diabetes just how much it matters during the especially vulnerable time when pregnancy is on the discussion agenda. And so, this work has been very much powered by community, bringing together lots of people to establish just how people with diabetes can be better supported during this time.
Congratulations to Niki Breslin-Brooker for driving this initiative, and to the team of mainly community members along with HCPs. This has all been done by volunteers, out of hours, in between caring for family, managing work and dealing with diabetes. It’s an honour to work with you all, and a delight to share details of what we’ve been up to!
Have a look at some of the artwork that has been developed to accompany the work. What we know is that it isn’t difficult to make a change that makes a big difference. The phrases you’ll see in the artworks that are being rolled out will be familiar to many people with diabetes. I know I certainly heard most of them back when I was planning for pregnancy – two decades ago. As it turns out, people are still hearing them today. We can, and need to change that!
You can be a part of this important work by filling in this survey which asks for your experiences. It’s for people with diabetes and partners, family members and support people. They survey will be open until the end of September and will inform the next stage of this work – a position statement about language and communication to support people with diabetes.
How do I get involved in research?
One of the things I am frequently asked by PWD is how to learn about and get involved in research studies. Some ideas for Aussies with diabetes: JDRF Australia remains a driving force in type 1 diabetes research across the country, and a quick glance at their website provides a great overview. All trials are neatly located on one page to make it easy to see what’s on the go at the moment and to see if there is anything you can enrol in.
Another great central place to learn about current studies is the Diabetes Technology Research Group website.
ATIC is the Australasian Type 1 Diabetes Immunotherapy Collaboration and is a clinical trials network of adult and paediatric endocrinologists, immunologists, clinical trialists, and members of the T1Dcommunity across Australia and New Zealand, working together to accelerate the development and delivery of immunotherapy treatments for people with type 1 diabetes. More details of current research studies at the centre here.
HypoPAST
HypoPAST stands for Hypoglycaemia Prevention, Awareness of Symptoms and Treatment, and is an innovative online program designed to assist adults with type 1 diabetes in managing their fear of hypoglycaemia. The program focuses on hypoglycaemia prevention, awareness of symptoms, and treatment, offering a comprehensive range of resources, including information, activities, and videos. Study participants access HypoPAST on their computers, tablets, or smartphones.
This study is essential as it harnesses technology to provide practical tools for better diabetes management, addressing a critical need in the diabetes community. By reducing the anxiety associated with hypoglycaemia and improving symptom awareness and treatment strategies, HypoPAST has the potential to enhance the quality of life for individuals with type 1 diabetes.
The study is being conducted by the ACBRD and is currently recruiting participants. It’s almost been fully recruited for, but there are still places. More information here about how to get involved.
Type 1 Screen
Screening for T1D has been very much a focus of scientific conferences this year. At the recent American Diabetes Association Scientific Sessions, screening and information about the stages of T1D were covered in a number of sessions and symposia. Here in Australia. For more details about what’s being done in Australia in this space, check out Type 1 Screen.
And something to read
This article was published in The Lancet earlier in the year, but just sharing here for the first time. The article is about the importance of genuine consumer and community involvement in diabetes care, emphasising the benefits and challenges of ensuring diverse and representative participation to meet the community’s needs effectively.
I spend a lot of time thinking a lot about genuine community involvement in diabetes care and how people with diabetes can contribute to that ‘from the inside’. And by ‘inside’ I mean diabetes organisations, industry, healthcare settings and in research. I may be biased, but I think we add something. I’m grateful that others think that too. But not always. Sometimes, our impact is dismissed or minimised, as are the challenges we face when we act in these roles. I don’t speak for anyone else, but in my own personal instance, I start and end as a person with diabetes. I may work for diabetes organisations, have my own health consultancy, and spend a lot of time volunteering in the diabetes world, but what matters at the end of the day and what never leaves me is that I am a person living with diabetes. And I would expect that is how others would regard me too, or at least would remember that. It’s been somewhat shocking this year to see that some people seem to forget that.
Final thoughts…
Recently when I was in New York at Breakthrough T1D headquarters, I realised just how many people there are in the organisation living with the condition. It’s somewhat confronting – in a good way! – to realise that there are so many people with lived experience working with – very much with – the community. And it’s absolutely delightful to be surrounded by people with diabetes at all levels of the organisation – including the CEO. But you don’t have to have diabetes to work in diabetes. Some of the most impactful people I’ve worked with didn’t live with the condition. But being around people with diabetes as much as possible was important to them. It’s really easy to do when people with diabetes are on staff! I first visited the organisation’s office years ago – long before working with them – to give a talk about language and diabetes. One of the things that stood out for me back then was just how integral lived experience was at that organisation. From the hypo station (clearly put together by PWD who knew they would probably need to use the supplies!) to the conversations with the team, community was in the DNA of the place. As staff, I’ve now visited HQs a few times, and I’ve felt that even more keenly. Walking through the office a couple of weeks ago, I saw this on the desk of one of my colleagues and I couldn’t stop laughing when I saw it. IYKYK – and we completely knew!

DISCLOSURES (So many!)
I was part of the group working on the AID Consensus Statement, and the National AID Access Summit that led to the statement.
I am on the team working on the Language Matters Diabetes and Pregnancy initiative.
I was a co-author on the article, Living between two worlds: lessons for community involvement.
I am an investigator on the HypoPAST study.
My contribution to all these initiatives has been voluntary
I am a representative on the ATIC community group, for which I receive a gift voucher honorarium after attending meetings.
I work for Breakthrough T1D (formerly JDRF).
Gosh, it’s been a hot minute since I last did one of these. The whole point of Interweb Jumble posts on Diabetogenic is to highlight anything that has caught my interest in the online diabetes world, write about initiatives I’ve been involved in, and, most importantly, to elevate the great work being done by others living with diabetes. Building folks up and promoting their amazing efforts has been at the heart of what I do, so I’m always happy to share what others are doing.
Grab a coffee, tea or shandy, (Don’t. Don’t grab a shandy), and read on.
Diabetes Chat
YES!! There is a new place to congregate online, in a different format, and with this one, you get to hear people’s voices. (Sorry to everyone who had to endure my 7am Aussie accent last Tuesday!). This is a new initiative that’s been set up by three DOC folks – Tom from the UK, and Chris and Sarah from the US, utilising a new feature on Twitter called Spaces. It’s a terrific way to host an online peer meeting, creating yet another time and place that is BY people with diabetes, FOR people with diabetes. There is a weekly guest who gets put through their paces with terrific questions from the hosts and those listening in, and an open mic chat time as well.
It’s super impressive to see people from all over the globe participating. It reminds me a little of the DSMA tweetchats which are very welcoming and open to all, regardless of where you live around the world.
Search #DiabetesChat on Twitter for more.
dStigmatize
The team at diaTribe has once again tapped into one of the important issues, and much spoken about topics in the diabetes community and developed a terrific new website addressing diabetes stigma. It’s called dStigmatize and you can find it here.
I’m delighted to see Diabetes Australia’s work on stigma and language highlighted so prominently on the site (disclosure: I work at Diabetes Australia and have been involved in this work), including the videos from last year’s Australian National Diabetes Week campaign, which have been viewed hundreds of thousands of times.

Seasons of…diagnosis
New research out of Finland asked if more people were diagnosed with type 1 diabetes during colder months. You can read the paper here.
And a discussion on Twitter about it here.
HypoRESOLVE podcast
The HypoRESOLVE comms team created a new podcast to showcase the incredible work of this researchers involved in the project, with a strong emphasis on how people with diabetes are involved in the project. I was delighted to host this podcast and speak with some truly remarkable clinicians and researchers as well as other people with diabetes who are on the projects Patient Advisory Committee. (Disclosure – I am on the HypoRESOLVE PAC. PAC members are now paid an honorarium for our time working on this project, however we were not at the time of recording or working on this podcast.)
Here is the most recent episode (on Spotify).
Better engagement with PWD = better services
Great paper from a team out of the UK looking at how connecting with the lived experience expertise of people with diabetes, health professionals and diabetes health services can improve service delivery.
One of the co-authors is one of the GBdoc OG, Laura (@Ninjabetic1 on Twitter), and it’s great to see her name back in the diabetes world, contributing to this important discussion.
And the DDA podcast…
The Danish Diabetes Academy developed a podcast out of their Winter School that featured Postdocs who had participated in the academy speaking with others in the diabetes world to discuss who academic researchers work to ensure their research reaches and benefits those they are researching. I was so honoured to be invited to be interviewed for their first episode and answered questions about how communication is important when engaging people with diabetes to be part of the research process. You can listen here.
Language Matters for Portuguese speaking friends with diabetes!
The latest in the Diabetes #LanguageMatters stable is this document out of Brazil. Always terrific to see more and more statements coming out, highlighting the importance of language and communication in diabetes.
Thinking of starting on an insulin pump?
If so, the awesome Grainne at Blood Sugar Trampoline has you covered with this post. It is truly one of the most measured pieces I’ve read about things to consider if you are on the path to starting an insulin pump. The gushiness and superlatives that many of us resort to when banging on about how much we love our pumps are replaced with sensible, and practical advice and suggestions. If this is where you’re thinking of taking your diabetes management, Grainne’s piece is a must read.
Who doesn’t want to come to ATTD!?
#dedoc° voices is back and heading to ATTD in April this year, and applications are still open if you would like to be considered as part of the program. Successful applicants will be granted access to the entire ATTD program, giving them an opportunity to share what they see and learn with their networks. Make your submission count – this is a competitive process and success is more likely for those who take the time to provide details of how they will be involved in the program. Details here.
(Disclosure: I am an advisor to the #dedoc° voices program. I do not receive any payment for this role.)

World Health Organisation
In March, the World Health Organisation, through the Global Diabetes Compact, is hosting a two-day focus group for people with lived experience of diabetes. If you’re interested in getting involved, there is an expression of interest process you can complete here.
Also from WHO is this survey which is asking people with diabetes how to improve messaging and communication. You only have until 28 Feb, so get onto it now! (Disclosure: I was a volunteer consultant in the development of this survey)
Massive kudos to the Global Diabetes Compact team who are doing an absolutely stellar job engaging with the community. Always so terrific to see!
A diabetes sea shanty…
You’re welcome.
(Follow @TypeWonDiabetes on Instagram here.)
People with diabetes and their involvement in research
An end of year delight was this article that I co-authored making it to publication. The article is about how to better involve people with health conditions in research (which really seems to be something I’ve been very focussed on recently!).
Spare a Rose – last push
February still has a last few days which means that Spare a Rose isn’t over yet. You can still donate and contribute to this year’s total and support people with diabetes in under-resourced countries through the Insulin for Life program.

Last night, when my Dexcom was in the middle of its two-hour warm up, I had a hypo. A nasty, horrible, come-out-of-nowhere, almost-passed-out, who-the-fuck-am-I hypo. You know the type.
‘That was a pretty bad low last night, wasn’t it?’ Aaron commented this morning while we were in the kitchen drinking coffee. After I I nodded he said, ‘I know, because you were doing that fast talking thing.’
‘That fast talking thing.’ It’s one of my weirder low symptoms. I speak very quickly at the best of times, so I this particular low symptom sends me turbo-charged!
So, today I’ve revisiting this post from 2016 which perfectly captured one of those fast talking lows. We were in New York, I was all over the shop and Aaron, the person who has had more front row seats to more hypos than either of us would care to remember, was his ever-patient self. The fast talking was about green apple flavour, because what else is there to talk about when scraping the bottom of glucose numbers while on a New York subway platform?
I still talk fast when I’m low. I still love green apple flavouring. And Aaron? He still listens to me as I blabber at breakneck speed through hypos. He still doesn’t like green apple Mentos. The weirdo.
__________________________________
On our last full day in New York, we walked down some stairs to the subway. My phone started vibrating and beeping and I knew that I was heading low.
I hadn’t really managed to get the whole hot-weather-walking-a-lot thing sorted out on this trip. I dealt with insane Conference Hypo Syndrome from literally the second I stepped foot into the conference centre in New Orleans, and just managed by setting a lowered temp basal rate and drinking a lot of juice.
And then, we were on holidays and while I know diabetes is for life, not just for X-mas, I couldn’t be bothered ‘doing diabetes’ and being smart about making some changes and addressing the lows properly.
For the most part, I was right. I responded to the rapid fall warnings on my Dex and avoided any super-nasty lows.
But this day in the New York subway, I was already firmly in ‘Deal With Me Now’ hypo territory. I had a bottle of juice in my bag, but walked into a little kiosk on the platform to see what I could use instead. And there before me I saw these:

I squealed.
‘Oh my god. Babe. BABE. LOOK!’ I said to Aaron as I grabbed a couple of packs and started to open them before paying. I think he fished out a couple of dollars from his pocket to pay the guy who was watching me carefully. ‘I love these,’ I announced loudly. ‘Green apple Mentos! I LOVE these!’
Aaron corralled me back to the platform and we sat down waiting for our train and I started to munch my way through the pack.
‘Want one?’ I asked him, pushing the tube into his face. ‘No thanks. I don’t like green apple flavour.’
This was a fact I knew well because every time I mention how much I love green apple flavour, he reminds me he doesn’t.
‘What? WHAT? Of course you do!’ I said. ‘It is the best flavour ever. EV-ER! Remember? It is everywhere in France. Remember, babe? Remember? And there was that time that I found green apple Mentos in Melbourne at a servo and got so excited that I bought, like, 40 tubes. Remember? Have one… Have one babe.’
‘No, I’m okay,’ Aaron said. He went back to reading something on his phone.
‘Babe. Do you remember that time at the servo? I told you, right? I was really low and I went in and saw them and got excited and was ranting and raving to the poor attendant about how excited I was and how I’d never seen them in Australia. Do you remember? The guy thought I was really weird because I couldn’t stop talking about how excited I was and how much I love green apple flavoured lollies. Do you remember?’
Aaron shut off his phone and turned to me. ‘I guess I’ll read this later,’ he said smiling.
I ignored him and continued. ‘So I told him how green apple flavour was EVERYWHERE in France, but not here in Australia and how you could get green apple gum and soft drinks and heaps of other stuff and how I love it. LOVE. IT! Remember how it is everywhere in France? Yeah? And then I asked him how many packs of Mentos they had and I dumped them all on the counter and bought them. I spent, like, sixty dollars on lollies. Green apple lollies. I was so excited and speaking really quickly. Like, super quickly. Almost ranting. Like the fast talked in Seinfeld. Remember Jackie the lawyer in Seinfeld? I was talking really, really fast. Like that.’
‘Kind of like now?’ Aaron asked.
‘Am I? Am I? I am… Aren’t I?’ I said. ‘Yeah – I guess. Maybe it’s the green apple. Do you think that’s what it is? Do you, babe? Could it be the green apple? I LOVE green apple flavour! I should have bought more. Will I go back?’
‘I think it could be because you are low. And I think maybe you should eat a few more of those Mentos instead of just speaking about them.’ Aaron said gently.
‘Do you want one? They are great! I love this flavour!’ I asked.
The train pulled into the station and we found a seat. I checked my iPhone and saw that I was no longer dropping. I took a deep breath and looked around the carriage.
‘I really like green apple flavouring,’ I murmured to Aaron. He reached over and took my hand.
‘I know. And you’re really funny sometimes when you are low.’
I rested my head on his shoulder and concentrated on my heart rate, which was slowing down. By the time we got off the train I was feeling fine. And happy. Because tucked away in my bag was a yet to be opened packet of green apple Mentos.
I generally don’t do my best work at 2am. I’m just not the spring chicken I used to be, and being awake, engaging and remotely coherent when I am usually in the middle of some decent REM sleep is a big ask these days.
But living in Australia, and wanting to remain as active as possible in global diabetes work and activities has meant that I have had to suck it up and learn to get on with it. I’ve become expert at stealthily getting up about so as not to wake my family, moving like a ninja about the house. I make a pot of tea, have hypo supplies handy, and layer on red lipstick to create the illusion of being alert and awake, completely together and impossibly glamourous (I fear I am only fooling myself) before settling into do whatever it is that I am needed to do in the wee hours.
Last night, it was a 1.30am call for a 2am event. I’d snuck in a couple of hours sleep ahead of the rude alarm that woke me. When I logged onto the event platform, I still had my ‘morning voice’ on, but the hot tea helped lubricate – and wake up – my vocal cords. Thankfully I was only required to speak and not sing an opera. (Silver linings!)
But despite grumbling about the hour, I’m glad I did it. Because the following couple of hours was a discussion about hypoglycaemia that combined lived experience stories from people with diabetes, peer support, all articulated with fabulous input from clinicians and researchers. It really was an exercise in how to put together an online diabetes event!
The event was the Lilly Hypo Summit, and I co-hosted with Bastian Hauck who is an absolute pro in any hosting seat. When I was asked to be involved, I had visions of a very staged and scripted event. I have worked with industry enough to understand that their compliance rules often means that events are required to be defined to the nth degree with all content being scrutinised by legal eyes, leaving little room for spontaneity or free discussion. How could we possibly get the true experience of hypos across if we were constrained by needing to stick within a pre-planned programme? I mean, hypos don’t do that, so discussions about them surely shouldn’t have to – and simply couldn’t if we were to do it justice.
Amazingly, we managed to put together an engaging and somewhat impulsive and free-formed event with full support from the global engagement team. They trusted the PWD who were shaping the event enough to understand that what we were trying to do was be respectful to the people telling their stories by not in any way censoring them. Plus we promised no one would throw caution to the wind, and talk about replacing their traditional diabetes management with bathing under a full moon and dancing to the beat of an inner drum (or something), which considering last night was a full moon, was a pretty important promise to make. We created a space for PWD to share their stories and highlight the incredibly complex challenge that is hypoglycaemia, and we punctuated those stories with research and clinical advice.
I knew that it was going to be a good event, because the speakers were remarkable. When it was over, I had dozens and dozens of messages from people congratulating me on my hosting, but there is a secret that I feel I should share. Hosting is impossibly easy when you are interviewing brilliant people. And it was programme overflowing with brilliant people. The PWD who spoke had fascinating tales to tell, and told them in wonderfully disarming ways. I’d not met them all and it was great to be just as surprised as the audience when hearing their stories. And then we had two remarkable researchers who I respect greatly, and I know to be incredible communicators.
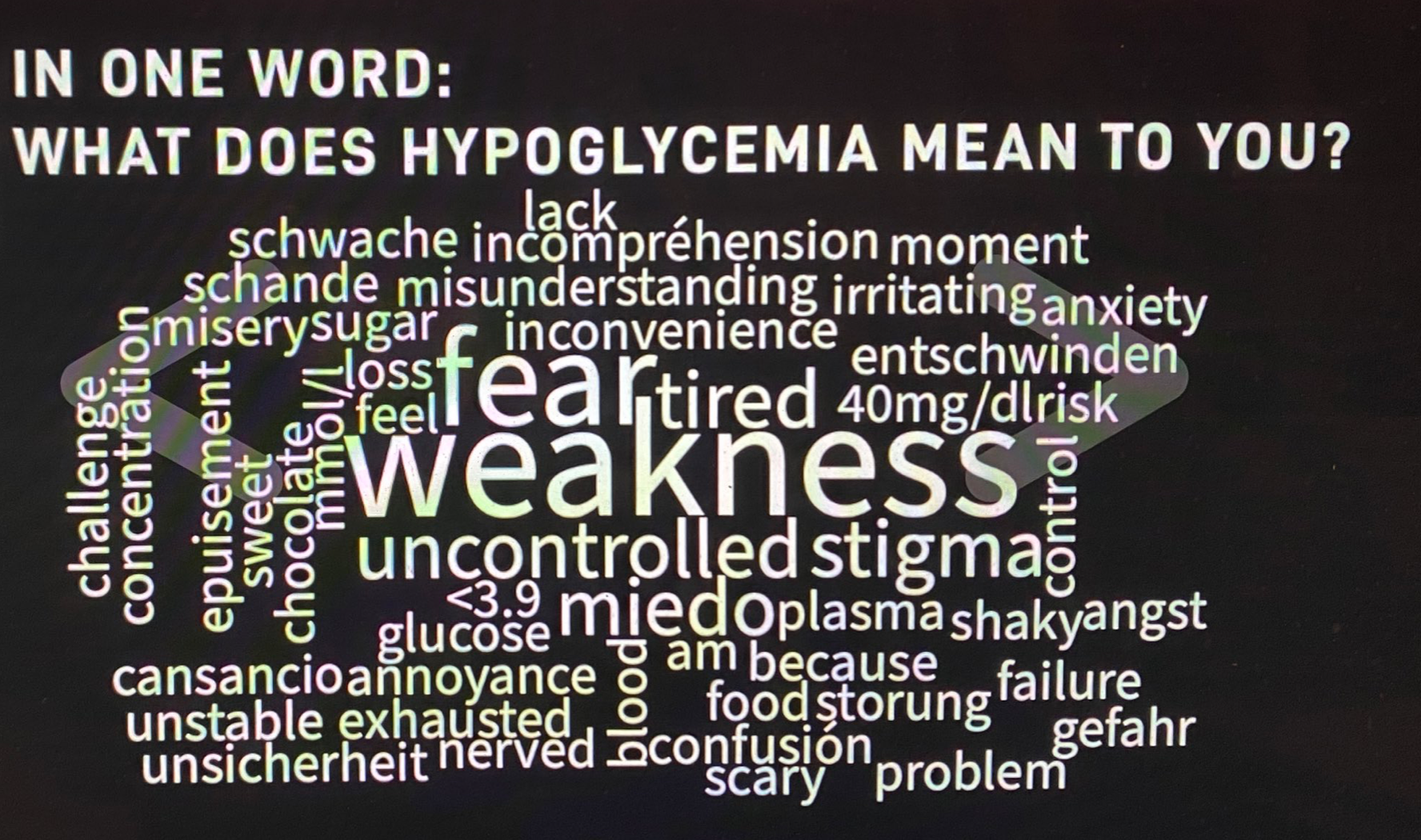
I really want to write more about what was discussed at the event, and will try to do that in upcoming posts, but for now, I just want to share this world cloud. We asked people to describe their hypos in one word. I’ve done exercises like this before and they never, ever reveal the same words. This is what the group came up with last night:
But to finish this post, I want to ask the question that one of last night’s HCPs, Pratik Choudhary, from the Leicester Diabetes Centre in the UK, asked us: ‘Do you see hypos as a slope or a cliff face?’ I can’t stop thinking about this, because I’ve never been asked about hypos this way, but it makes so much sense to consider them in this context. Of course, there are so many factors at play, but this either / or scenario does perfectly capture the in-the-moment way that I feel about hypos. I wonder what you might think about your hypos. Does it fit in here, or is it something completely different?
DISCLOSURE
I was an advisor to Lilly Diabetes for the Hypo Summit. I have been paid for my time. I have not been asked to write anything about the summit, but am sharing because there was so much amazing content at the event. No one has reviewed this post prior to publication.
Two years ago today, I was at Melbourne airport, getting ready to board a plane to get to Nijmegen, via Amsterdam, for the second AGM for the HypoRESOLVE project. I have been part of the Patient Advisory Committee (PAC) since the project’s start, and am honoured to be included amongst such a terrific and passionate group of people with type 1 and type 2 diabetes to lend the lived experience perspective to the work. (Disclosure statement at the end of today’s post.)
A project this big has a lot of moving parts and there is a constant stream of work being done. Right now, one of the most exciting things that we are seeing is a survey for people with diabetes to share their experiences of how hypos impact the quality of life of people with diabetes and our loved ones.
I love that this project is looking at more than simply the clinical side of hypoglycaemia. I’d like to think that the PAC has been influential in this, however one of the things that made me so keen to get involved in the project was that, from its inception, the psychological burden was an integral part of the research. Work package 6, led by Jane Speight and Frans Pouwer, aims to provide just what the impact of hypos are on the quality of life of PWD and our families. I know that in the presentations I’ve given for this project (including at the launch meeting in May 2018), my focus has certainly been on how hypos make me feel emotionally, rather than physically. (I’ll link to pieces I wrote about these presentations at the end of the post today.)
Right now, it’s time for more than just the PWD on the PAC to have a say – to have Your SAY – by taking part in this new survey. It takes about 30 mins, although I’m seeing heaps of people saying they’re whizzing through it much quicker than that. To complete the survey, you need to:
- be 16 years of over
- be able to complete the survey in English
- have type 1 diabetes, diagnosed over six months ago
- have type 2 diabetes, and use insulin
- live with and be in a relationship with someone with diabetes.
Click below to go to the survey, and to find out more information.

The more people who provide their experiences, the more rounded and richer the research will be. Throughout the project, the PAC has repeatedly advocated for the voices of as many PWD as possible to be included (this certainly isn’t the first time a group extending beyond PAC members has been consulted), so please, if you can, take the time to do the survey.
Hypos are a tricky beast; trying to get a really good picture about how they affect our quality of life is essential in developing treatments to make them more manageable.
More about HypoRESOLVE?
This post, explaining all about the project’s launch meeting.
This post about a talk I gave at a satellite meeting at EASD which addressed the differences between how PWD define hypos and the official categories.
This post, about the difficulties of defining hypoglycaemia in ways that are meaningful for everyone.
Here’s a little video that we recorded at the kick-off meeting.
And stay tuned for the podcast!
DISCLOSURE
I have been a member of the HypoRESOLVE PAC since the project started. Until the beginning of this year, PAC members were volunteers on the project, with all flights, accommodation, meals and expenses covered from the project budget. Since the beginning of 2021, PAC members have been paid an honorarium for time worked on the project. I have not been paid to write this post, and my words here have not been approved (or read) by anyone on the project before publication.
I was speaking with someone who is thinking about starting to Loop the other day. I explained my own experiences – how simple the set-up had been (even after I’d delayed it for six months because I thought I wouldn’t be able to do it), how it is completely changed the way I think about diabetes, how much less time I have to dedicate to dealing with the daily frustrations of diabetes, how the highs and lows have been evened out and how glucose rollercoasters are a thing of the past.
‘So, you never have highs and lows? Ever?’ he asked me.
‘No; that’s not completely true,’ I said. I am frequently guilty of being evangelical about diabetes technology, and wanted to be sure that I wasn’t overselling DIYAPS. ‘After all, I still have diabetes!’
I have my range set to 4mmol/l – 8.0mml/l. It’s the mythical range that was presented to me as the ultimate goal the day I was diagnosed. It’s quite a tight range – I know that – and I probably could afford to ease up on that upper range. My target is 5.0mmol/l (it used to be 5.5mmol/l – another mythical number).
The reality is that for the very vast majority of the time, I am within that range, and hovering around that target number. If I was to check my Dex as soon as I woke up each morning, it would be boringly somewhere between about 4.8mmol/l and 5.3mmol/l.
But I still do spent time outside of the target range. The thing about Loop is that in most cases, I can explain the reasons when that happens.
I had a hypo the other night. A pretty terrible one, actually. I can’t remember the last time my Dex read LOW, but that was what I was staring at when I checked the app after my phone started screaming at me. I double checked with a finger prick and sure enough I was low. Really low. I treated (over treated) and was fine a short time later, albeit with a rebound leading to numbers I’ve not seen in a very long time.
How did that happen? Well, let’s start with the double bolus I gave myself. For some reason, I decided that the chicken soup with noodles I was eating for dinner needed not one, but two boluses. That was mistake number one. Mistake number two was not eating as much as I thought I was going to because I had a teleconference starting, so I left about half of my dinner in the bowl. Mistake number three was not realising mistake number one. And mistake number four was not doing anything to address mistake number two.
Following? Diabetes is fun!
The low resulted in an ‘eat-the-kitchen’ hypo that saw me eat six jelly beans, wait fifteen minutes and then recheck my glucose levels. Just kidding. I drank half a litre of juice, ate three bowls of breakfast cereal, chomped on a tube of fruit pastilles and then started attacking a homemade fruit bun my mum had delivered earlier in the day.
Because I was dying and all the carbs in the kitchen were the only way to prevent that happening.
The high that followed could be easily explained (see: juice, cereal, pastilles, fruit bun).
Other highs on Loop can usually also be explained quite simply. If I under bolus, I know pretty quickly, and Loop has already started doing its thing anyway to remedy that.
Stubborn highs generally mean one thing and one thing only: Renza, change your cannula. And as soon as I do, numbers come back into range fairly quickly.
Out of range numbers these days aren’t due to the unpredictability of diabetes. These days, they come down to one thing and one thing only: human error. My human error.
I trust Loop more than I trust myself. It is way smarter, completely and utterly unemotional, and an absolute workhorse, making adjustments every five minutes as required. It doesn’t get tired or busy or distracted. It understands numbers better than I ever will.
This is the cool tech I need to help me keep my diabetes moving. Of course, I still need the warm touch – the human connection – to help me make sense of my life with diabetes. But not having to think or do the diabetes numbers nearly as much gives me time and headspace I didn’t know I had. It keeps my numbers in range for the vast, vast majority of each day. And it means far fewer errors. Errors that I used to make all the time.
I am, after all, only human. Loop, on the other hand, is not.

I am not really the type to analyse reports of glucose data. I’ve never been like that, except for a brief period where I was overly obsessive. Or, as it is more commonly known: when pregnant. Then, I was all about entering numbers into Excel spreadsheets, (hey – it was the early 2000s), and I searching for patterns in the 15-20 BGL checks I was doing every day, circling anything even closely resembling a common theme in green. (Oh – green circles may always have been my thing…!)
These days, even with reports and graphs and all sorts of other fancy pants data at my fingertips, I don’t really do any analysis.
The reason I love Loop is because of how it makes me feel in the here and now. By reducing so many of the tasks I do, and my diabetes needing less urgent attention, plus dealing with fewer lows, fewer highs and fewer pretty much all the other shitty stuff, it means that my in-the-moment diabetes is far easier to manage.
Sure – I occasionally have a look at what my Clarity app is telling me, but it’s only ever the snapshot page: TIR, average glucose level and hypo risk.
Since being on Loop, my hypo risk has always looked like this:

Minimal risk. Take that in for a moment.
Diabetes – the condition that demands so much of us in terms of being able to complete highly complicated calculations factoring in pretty much every single variable imaginable and a million more, dosing a potentially lethal drug and really, no room for error.
Diabetes – the definition of a high-risk health condition.
And my personal risk of lows? Minimal.
So, remind me again: How is Loop (or other DIYAPS options) unsafe?
The other night, I cancelled going to a party – a cousin’s kid’s 18th– at the last minute. I seriously never do this. And I absolutely hated doing it.
But I’d had a couple of hypos during the day (Fiasp is absolutely kicking my arse) and I was feeling exhausted. These hypos weren’t what I’ve become used to dealing with (i.e. Loop hypos for me generally look like an alert telling me I’m going to head low, me ignoring it, alert saying I am really about to be low – but not really low because Loop is doing its thing, me having a couple of fruit pastilles, and that’s it). These were the types of hypos that spin me around, turn me upside down and resettle me feeling completely discombobulated. It had been a while.
After the second one, I was so knocked out that I lay down for a bit and ended up getting an hour’s sleep. It was mid-afternoon and when I woke up, I felt no more refreshed.
I contemplated going to the party – I had a shower and started to put on some make up. I looked fine – no different to how I usually look. If I’d gone, no one would have known any different.
Earlier in the day, after I’d already had the first hypo, Aaron had posted a photo of me online. The next day, when I mentioned to someone that I had cancelled plans the evening before thanks to a lousy diabetes day, said ‘Oh. I saw a photo of you online in the morning and you looked great.’
They didn’t mean this in a nasty way, or that they thought I had just cancelled because I couldn’t be bothered going out. It was just a comment. And they were right – I looked exactly the way I would look any other weekend morning when I was having breakfast with family and friends
The next day I was messaging a friend with diabetes and mentioned I’d cancelled my plans at the last minute the night before. ‘Oh babe,’ she said. ‘How’s the hypo hangover?’ and then she detailed all the things that are the inevitable fallout of nasty (and nasty-ish) lows; the things I’d not mentioned to others who’d asked after me.
I told her she had nailed exactly how I was feeling. I told her what had happened, and I didn’t hold back, and I didn’t minimise it. I knew she wouldn’t worry or be unnecessarily concerned or wonder if it was anything more than what it was. I knew she would know – because those feelings are wound into the DNA of diabetes and the people living with it.
Plus, she would know just how I felt about the last-minute cancellation, and feeling that I’d let people down.
‘So, I bet you’re feeling even more crap about cancelling that about the hypos now, right?’ she said.
I laughed. ‘You know it!’ I said to her
‘Don’t you sometimes wish that when you were having a shitty diabetes day it couldn’t be covered up so easily with lipstick and a smile?’ she said, hitting me right in the guts with that comment.
Because she was so right. Lipstick and a smile. That’s every diabetes day. It’s there when I’m feeling great and all is going well; when diabetes is behaving and not impacting on me much at all. And it’s there when I’m feeling crap and diabetes is casting far too large a shadow over my existence for that day. But for most people, they couldn’t tell the difference.

Managing this hypo with iced coffee…and lipstick and a smile.






