
You are currently browsing the category archive for the ‘DOC’ category.
I probably should stop thinking of my job as ‘my new job’. I’ve been at Diabetes Australia now for well over five years. But for some reason, I still think of it that way. And so do a lot of other people who often will ask ‘How’s the new job?’
Well, the new job is great, and I’ve enjoyed the last five years immensely. It’s a very different role to the one I had previously, even though both have been in diabetes organisations.
One thing that is very different is that in my (not) new job I don’t have the day-to-day contact with people with diabetes that I used to have. That’s not to say that I am removed from the lived experience – in fact, in a lot of ways I’m probably more connected now simply because I speak to a far more diverse group of people affected by diabetes. But in my last job, I would often really get to know people because I’d see them at the events my team was running, year in, year out.
Today, I got a call from one of those people. (I have their permission to tell this story now.) They found my contact details through the organisation and gave me a call because they needed a chat. After a long time with diabetes (longer than the 23 years I’ve had diabetes as an annoying companion), they have recently been diagnosed with a diabetes-related complication. The specific complication is irrelevant to this post.
They’ve been struggling with this diagnosis because along with it came a whole lot more. They told me about the stigma they were feeling, to begin with primarily from themselves. ‘Renza,’ they said to me. ‘I feel like a failure. I’ve always been led to believe that diabetes complications happen when we fail our diabetes management. I know it’s not true, but it’s how I feel, and I’ve given myself a hard time because of it.’
That internalised stigma is B.I.G. I hear about it a lot. I’ve spent a long time learning to unpack it and try to not impact how I feel about myself and my diabetes.
The next bit was also all too common. ‘And my diabetes health professionals are disappointed in me. I know they are by the way they are now speaking to me.’
We chatted for a long time, and I suggested some things they might like to look at. I asked if they were still connected to the peer support group they’d once been an integral part of, but after moving suburbs, they’d lost contact with diabetes mates. I pointed out some online resources, and, knowing that they often are involved in online discussions, asked if they’d checked out the #TalkAboutComplications hashtag. They were not familiar with it, and I pointed out just how much information there was on there – especially from others living with diabetes and diabetes-related complications. ‘It’s not completely stigma free,’ I said. ‘But I think you’ll find that it is a really good way to connect with others who might just be able to offer some support.’
They said they’d have a look.
We chatted a bit more and I told them they could call me any time for a chat. I hope they do.
A couple of hours later, my phone beeped with a new text message. It was from this person. They’d read through dozens and dozens of tweets and clicked on links and had even sent a few messages to some people. ‘Why didn’t I know about this before?’, they asked me.
Our community is a treasure trove of support and information, and sometimes I think we forget just how valuable different things are. The #TalkAboutComplications ‘campaign’ was everywhere a couple of years ago, and I heard from so many people that it helped them greatly. I spoke about it – particularly the language aspect of it – in different settings around the world and wrote about it a lot.
While the hashtag may not get used all that much these days, everything is still there. I sent out a tweet today with it, just as a little reminder. All the support, the connections, the advice from people with diabetes is still available. I hope that people who need it today can find it and learn from it. And share it. That’s one of the things this community does well – shares the good stuff, and this is definitely some of the good stuff!
Want more?
Check out the hashtag on Twitter here.
You can watch a presentation from ATTD 2019 here.
Read this article from BMJ.

I don’t know too many people living with diabetes who haven’t experienced stigma. I know I certainly have. In twenty-three years of living with diabetes, it’s come from all directions: the media, healthcare professionals, work colleagues and even family and friends. That’s because people outside the diabetes community often have pre-conceived ideas about what diabetes is all about, and a lot of those ideas are plain wrong.
But stigma doesn’t only come from outside the community. In fact, for some people with diabetes, some of the most harmful and hurtful experiences of stigma has actually come from other people with, or affected by, diabetes. [Click here to read more…]

DISCLOSURE
This piece was published today on the Diabetes Australia website, and I wrote it as part of the organisation’s National Diabetes Week campaign on diabetes stigma. I work for Diabetes Australia, and am sharing this because I’ve chosen to – not because I’ve been asked to. The words here are my own, and perhaps the only thing missing from the published text is some of the decorative language I often use when speaking about diabetes-related stigma. Bottom line – all stigma sucks. Let’s #EndDiabetesStigma now.
I generally don’t do my best work at 2am. I’m just not the spring chicken I used to be, and being awake, engaging and remotely coherent when I am usually in the middle of some decent REM sleep is a big ask these days.
But living in Australia, and wanting to remain as active as possible in global diabetes work and activities has meant that I have had to suck it up and learn to get on with it. I’ve become expert at stealthily getting up about so as not to wake my family, moving like a ninja about the house. I make a pot of tea, have hypo supplies handy, and layer on red lipstick to create the illusion of being alert and awake, completely together and impossibly glamourous (I fear I am only fooling myself) before settling into do whatever it is that I am needed to do in the wee hours.
Last night, it was a 1.30am call for a 2am event. I’d snuck in a couple of hours sleep ahead of the rude alarm that woke me. When I logged onto the event platform, I still had my ‘morning voice’ on, but the hot tea helped lubricate – and wake up – my vocal cords. Thankfully I was only required to speak and not sing an opera. (Silver linings!)
But despite grumbling about the hour, I’m glad I did it. Because the following couple of hours was a discussion about hypoglycaemia that combined lived experience stories from people with diabetes, peer support, all articulated with fabulous input from clinicians and researchers. It really was an exercise in how to put together an online diabetes event!
The event was the Lilly Hypo Summit, and I co-hosted with Bastian Hauck who is an absolute pro in any hosting seat. When I was asked to be involved, I had visions of a very staged and scripted event. I have worked with industry enough to understand that their compliance rules often means that events are required to be defined to the nth degree with all content being scrutinised by legal eyes, leaving little room for spontaneity or free discussion. How could we possibly get the true experience of hypos across if we were constrained by needing to stick within a pre-planned programme? I mean, hypos don’t do that, so discussions about them surely shouldn’t have to – and simply couldn’t if we were to do it justice.
Amazingly, we managed to put together an engaging and somewhat impulsive and free-formed event with full support from the global engagement team. They trusted the PWD who were shaping the event enough to understand that what we were trying to do was be respectful to the people telling their stories by not in any way censoring them. Plus we promised no one would throw caution to the wind, and talk about replacing their traditional diabetes management with bathing under a full moon and dancing to the beat of an inner drum (or something), which considering last night was a full moon, was a pretty important promise to make. We created a space for PWD to share their stories and highlight the incredibly complex challenge that is hypoglycaemia, and we punctuated those stories with research and clinical advice.
I knew that it was going to be a good event, because the speakers were remarkable. When it was over, I had dozens and dozens of messages from people congratulating me on my hosting, but there is a secret that I feel I should share. Hosting is impossibly easy when you are interviewing brilliant people. And it was programme overflowing with brilliant people. The PWD who spoke had fascinating tales to tell, and told them in wonderfully disarming ways. I’d not met them all and it was great to be just as surprised as the audience when hearing their stories. And then we had two remarkable researchers who I respect greatly, and I know to be incredible communicators.
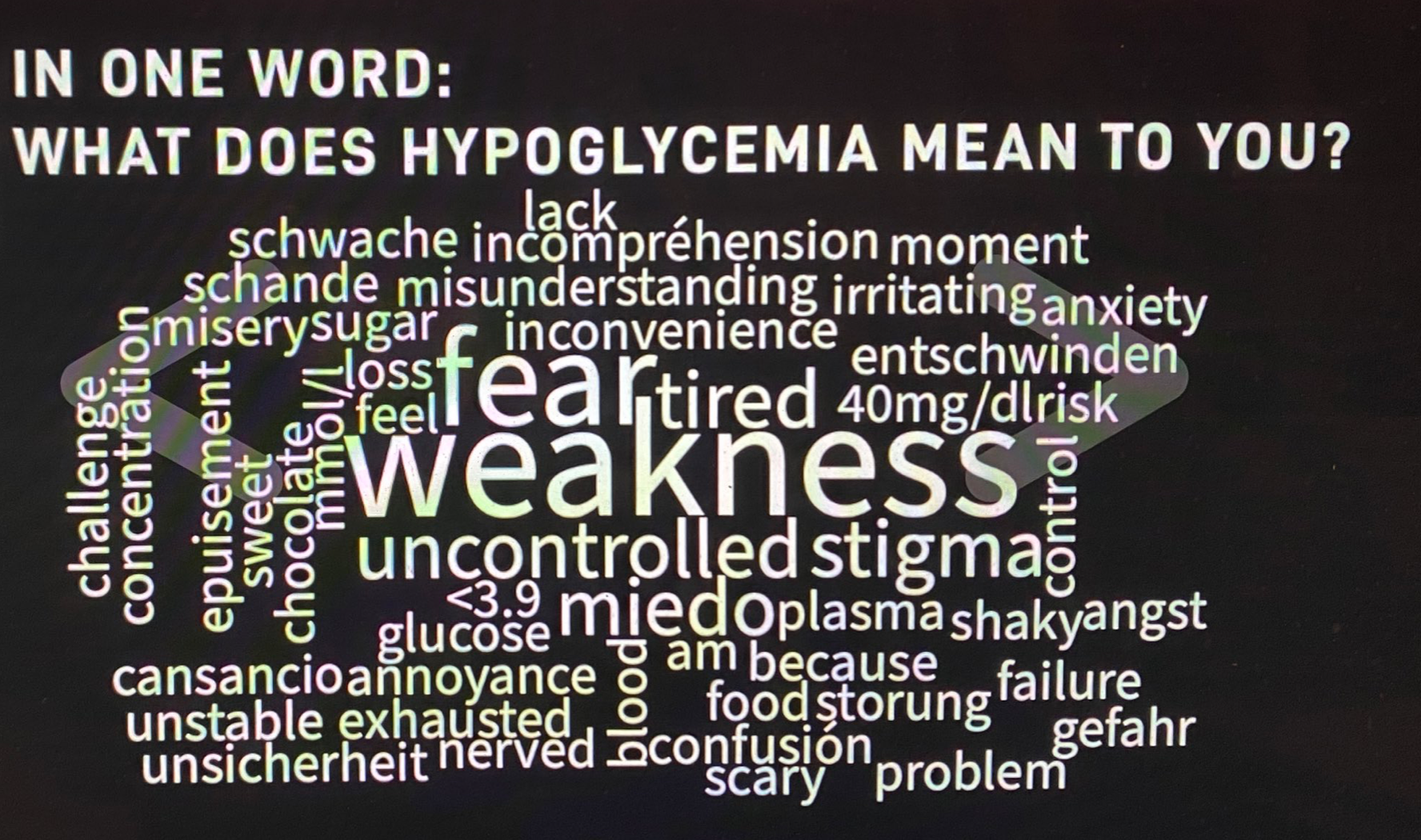
I really want to write more about what was discussed at the event, and will try to do that in upcoming posts, but for now, I just want to share this world cloud. We asked people to describe their hypos in one word. I’ve done exercises like this before and they never, ever reveal the same words. This is what the group came up with last night:
But to finish this post, I want to ask the question that one of last night’s HCPs, Pratik Choudhary, from the Leicester Diabetes Centre in the UK, asked us: ‘Do you see hypos as a slope or a cliff face?’ I can’t stop thinking about this, because I’ve never been asked about hypos this way, but it makes so much sense to consider them in this context. Of course, there are so many factors at play, but this either / or scenario does perfectly capture the in-the-moment way that I feel about hypos. I wonder what you might think about your hypos. Does it fit in here, or is it something completely different?
DISCLOSURE
I was an advisor to Lilly Diabetes for the Hypo Summit. I have been paid for my time. I have not been asked to write anything about the summit, but am sharing because there was so much amazing content at the event. No one has reviewed this post prior to publication.
Last night, my gorgeous friend Andrea tweeted how she had seen someone wearing a CGM on the streets of Paris. When she rolled up her sleeve to show him her matching device, he turned and walked away. ‘Guess you can’t be best friends with every T1D’, she wrote. ‘Diabetes in the Wild’ stories have been DOC discussion fodder for decades – including wonderful stories of friendships being started by a chance encounter, and less wonderful stories such as Andrea’s most recent encounter. I was reminded of the many, many times pure happenstance of random diabetes connection has happened to me.
There was the time I was waiting for coffee and another person in line noticed my Dexcom alarm wailing, and the banter we fell into was so comfortable – as if we’d known each other forever!
And that time that someone working the till at a burger flashed her CGM at me after seeing mine on my arm and we chatted about being diagnosed as young adults and the challenges that poses.
Standing in line, queuing for gelato, is as good as any place to meet a fellow traveller and talk about diabetes, right? That’s what happened here.
And this time where I spotted a pump on the waistband of a young woman with diabetes, and started chatting with her and her mother. The mum did that thing that parents of kids with diabetes sometimes do – looking for a glimpse into her child’s future. She saw that in my child, who was eagerly listening to the exchange. But I walked away from that discussion with more than I could have given – I remember feeling so connected to the diabetes world in that moment, which I needed so much at the time.
I bet that the woman in the loos at Madison Square Garden wasn’t expecting the person who walked in at the exact moment she was giving herself an insulin injection to be another woman with diabetes. But yeah, that happened…
I’ll never forget this time that I was milliseconds from abusing a man catcalling me out his car window, until I realised he was yelling out at to show me not only our matching CGMs, but also the matching Rockadex tape around it. My reaction then was ridiculous squealing and jumping up and down!
Airports have been a fruitful place to ‘spot diabetes’, such as the time my phone case started a discussion with a woman whose daughter has diabetes, except we didn’t really talk about diabetes. And the time another mum of a kid with diabetes was the security officer I was directed to at Amsterdam’s Schiphol Airport. She was super relaxed about all my diabetes kit, casting her eyes over it casually while telling me about her teenage son with diabetes.
The follow up to this time – where I introduced myself to the young mum at the next time who I overheard speaking about Libre, and saying how she was confused about how it worked and how to access it – but not really being all that sure about it, is that she contacted me to let me know that she’d spoken with their HCP about it, had trialled it and was now using it full time. She told me that managing diabetes with toddler twins was a nightmare, and this made things just a little easier.
Sometimes, seeing a stranger with diabetes doesn’t start a conversation. It can just an acknowledgment, like this time at a jazz club in Melbourne. And this time on a flight where we talked about the Rolling Stones, but didn’t ‘out ourselves’ as pancreatically challenged, even though we knew …
But perhaps my favourite ‘Diabetes in the Wild’ story is one that, although I was involved, I didn’t write about. Kerri Sparling wrote about it on her blog, Six Until Me. Kerri was in Melbourne to speak at an event I was organising, and one morning, we met at a café near my work. We sat outside drinking our coffees, chatting away at a million miles an hour, as we do, when we noticed a woman at the next table watching us carefully. We said hi, and she said that she couldn’t help listening to us after she heard us mention diabetes. She told is her little girl – who was sitting beside her, and was covered in babycino – had recently been diagnosed. I will never forget the look on the mother’s face as two complete strangers chatted with her about our lives with diabetes, desperately wanting her to know that there were people out there she could connect with. I also remember walking away, hoping that she would be okay.
Five years later, I found out she was okay – after another chance encounter. I was contacting people to do a story for Diabetes Australia and messaged a woman I didn’t know to see if she, along with her primary aged school daughter would be open to answering some questions. Turns out, this was the woman from Kerri’s and my café encounter. She told me how that random, in the wild conversation made her feel so encouraged. She said that chance meeting was the first time she’d met anyone else with diabetes. And that hearing us talk, and learning about our lives had given her hope at a time when she was feeling just so overwhelmed.
I know that not everyone wants to be accosted by strangers to talk about their health, and of course, I fully respect that. I also know there are times that I find it a little confronting to be asked about the devices attached to my body. But I also know that not once when I’ve approached someone, or once when someone has approached me has there been anything other than a warm exchange. I so often hear from others that those moments of accidental peer support have only been positive, and perhaps had they not, we’d all stop doing it. It’s a calculated risk trying to start a conversation with a stranger, and I do tread very lightly. But I think back to so many people in the wild stories – the ones I’ve been involved in, and ones shared by others – and I think about what people say they got out of them and how, in some cases they were life changing. A feeling of being connected. The delight in seeing someone wearing matching kit. The relief of seeing that we are so alone. The sharing of silly stories, and funny anecdotes. And in the case of that mum with a newly diagnosed little kid, hope.
Today’s post is dedicated to Andrea whose tweet kicked off this conversation in the DOC last yesterday. Thanks for reminding me about all these wonderful chance meetings, my friend.
There have been a number of times here on this blog and in other online platforms that I have been critical about the low carb community. Actually, let me be more specific. I have been critical of the response from certain corners of that community, particularly the corners that are free with their fat shaming, and accusing people with diabetes who choose not to eat low carb as not caring about their health, and attacking others for daring to suggest that there could possibly be more than one way to eat. This has come from a long list of incidents I’ve either seen or have been involved in, such as the time I was fat shamed for saying that intermittent fasting is great for some, but not for everyone, and the time that people in the LC community got angry at the idea of saving the lives of children with diabetes from developing countries.
I guess I shouldn’t have been surprised really at what happened earlier this week just before I published a post on diabetes and menopause. As I often do, I look to the community for others’ experiences. And so, I tweeted (and shared on Facebook) this:

The responses were many and great. One aspect of the generosity of the DOC is the willingness and openness to share not only experiences, but to offer tips and tricks for what has worked for them. I’ve always found that so amazing, especially when addressing issues that are considered a little taboo. Menopause is one of those issues. But even so, there were so many replies from people who have either gone through menopause, or started to think about it.
And then, out of the blue, came a reply from a nutritionist. A nutritionist I have never encountered before. I don’t follow him on Twitter, I have no idea who he is. Which is all fine. My Twitter is public and if I ask a question everyone is free to offer their input. Here is his reply:

I replied that I am not a healthcare professional. And then came this:
Followed by this from me:

(I’m not going to share anymore of the tweets in what turned out to be a rather long back and forward thread, but if you click on any of the tweets above you will be able to find the whole mess.)
He kept going, demanding to know why I am critical of low carb diets and health professionals who promote them (which he apparently had deduced from reading through my Twitter feed). I’m not. Which is what I repeatedly tweeted to him in responses to his continued demands that I explain my stance on diets and diabetes, and, as a healthcare professional, I must stop giving ‘personality-driven healthcare advice’. I reminded him that, a) I am not a HCP (which I had already stated), and, b) I share my experiences, not give advice. He helpfully suggested that my blog posts read that way.
I had asked about menopause. I asked people with diabetes who had either been through menopause, were going through it now, or thinking about going through it. I asked whether it had been a topic of conversation with their HCPs.
This bloke – who doesn’t have diabetes and has never experienced menopause – had nothing to offer, other than attacking me for my choices. And my choice is that I believe in choice.
It’s not okay for a healthcare professional to enter into a discussion with a person with diabetes seeking peer support, and telling them what it is that they do and don’t do in that community. I am so over this sort of paternalism in healthcare. I’m over HCPs bullying their way into our community and trying to shape it into what they want.
I’d also add that a man hijacking a conversation started by a woman about menopause is pretty shitty behaviour. I’m also over misogyny and the way male healthcare professionals centre themselves in discussions that are not about them. It happens all the time. It happened on Monday.
A tweet about menopause. And not even about food and menopause! It sounds somewhat ridiculous really. I don’t look for this sort of reaction, and I certainly have never baited anyone from the LC community. I don’t post photos of high carb meals accompanied by a ‘dare you to say something’ comment. (But I should say, that even if people are doing that, there is still no valid reason to criticise what another person is eating** or criticise the way they choose to eat.)
I understand that there will always be difficult people in any community. Unfortunately, it is people like this who are often the most seen from the LC community. And it’s why I am critical. But be clear – I am not critical for the advice they are giving, or the eating plan they are following. I am critical of, and will continue to call out, this sort of behaviour.
**Okay, I know that I said that there is no valid reason to criticise what another person is eating. But I am adding a caveat to that because I do (and probably will continue to) criticise anyone who wants to drink flavoured coffee. Or instant coffee. Or coffee from a bag. I fully acknowledge and accept my status as a Melbourne coffee snob and will not be entering into any discussions that caramel, pumpkin spice or unicorn flavourings are okay. They are not. Don’t @ me.
I went to my first international diabetes conference back in 2011. It was the IDF World Diabetes Congress in Dubai. In a slightly convoluted way in, I was there as a guest of the City of Melbourne. The next Congress was to be held in my home city, so the tourism arm of our local government attended the conference, talking up all that Melbourne has to offer. I was invited to go and spruik the city I love so much, encourage people to make the (very) long haul trip Down Under… and hand out little clip-on koalas while standing next to giant koalas.

After attending and getting a taste for what was on offer at one of these large-scale conferences, I realised that I wanted to be able to be involved in others moving forward. Undoubtedly, it was great professional development for me – as someone working in advocacy in a diabetes organisation – but it was also a great way to network and meet others in the advocacy space, learn about what they were doing, and work out how we could collaborate. I can’t begin to think of all the terrific projects that started in the corridors, running between sessions! And most importantly, I realised that having PWD at diabetes conferences meant that what was on show was being shared with our peers in a way that made sense.
The struggle, of course, was getting to these conferences. Australia is a long way from anywhere and with that comes expensive travel costs. The organisations I have worked for cover maybe a max of one event per year as part of my professional development, so the rest of the time it was up to me to find a way in. Good thing I know how to hustle! In fact, that’s the way that most other PWD who attend these meetings get there.
My disclosure statements at the end of posts detail the support I’ve received. Sometimes I’m an invited speaker so that makes covering costs easy. In recent years, research projects I’m involved with, or ad boards I’m a member of, often run meetings alongside international conferences, so my travel and some accommodation are covered. I was informed early on by other advocates that there are often satellite events run by device and pharma companies, and I became very good at begging asking for an invitation, and then following that with more begging asking for help to cover accommodation and travel costs. I know that it doesn’t come easy for lots of people to ask for money, especially when most of the time the answer is going to be no, but I’ve developed tough skin in 20 years of advocacy, and can take rejection. It just propels me to the next ask! (For the record, HCPs also do this hustle to help cover their costs. It’s not just advocates!) Another thing that has helped is my growing conviction about how critical it is – and non-negotiable – that people with diabetes are at these meetings. #NothingAboutUsWithoutUs may have started as a whisper, but now it’s a roar that comes with an expectation that we must be there, and we must be supported to get there!
Pretty much every single time I have travelled overseas to one of these meetings, I am out of pocket. Some of the costs are always borne by me. I am fortunate to be able to cover those costs, but I am fully aware that it is one of the many reasons that advocates don’t pursue attending.
I get that there are myriad reasons that getting to these meetings is difficult. It can seem that there is no way in; there are costs to cover; time needs to be taken from work; it means leaving family; getting registration can be difficult for non-healthcare professionals. And for many, they simply have no idea how to actually make the first move to attend. It can seem daunting. I know that it can seem that it’s always the same people at these events, and I think that’s partly because once people have found out the process of getting in, they keep doing it, because they realise it’s not as daunting as they first thought!
And so, that’s why initiatives like #dedoc° voices are so magic. It is an opportunity for all PWD to apply for a scholarship which will offer an access-all-areas pass to professional diabetes meetings. Want more details about this great program from advocacy group #dedoc°? Try here and here. The pilot for this was at ATTD in Madrid, just before the world turned upside down. It was a brilliant showcase of just how an open application process works, breaking down barriers that prevent people from attending.
While the #dedoc° voices at ATTD in Madrid offered travel and accommodation costs, as well as registration to the conference, the other two times the initiative ran (ISPAD and EASD) were virtual events, so only registration was covered.
And that brings us to 2021, and the first global diabetes conference for the year, ATTD, which kicks off next month. Applications for #dedoc° voices is open to PWD from all around the world now, but closes on Friday. It’s been a super short timeframe for this event, but it won’t take you too long to apply. You’ll find all the details right here.
Run don’t walk, and apply now, for your change to not only get to ATTD, but also to meet diabetes advocates from across the globe. It’s your way in. What are you waiting for?

Disclosure
I am an advisor to the #dedoc° voices program. I do not receive any payment for this role.
There are a lot of words that get thrown around the diabetes space to describe people involved in advocacy and support. These include (patient) leader, influencer, advocate, supporter… the list goes on. Some people prefer certain terms; others don’t. Some people don’t want to be labelled.
I had no idea the word ‘advocate’ was a loaded word in some places. I sprinkle it around like glitter – because I see it as a term that typically describes people doing really great things – and not just in diabetes.
It’s a word I’m comfortable with for myself.
It’s a word that I connected with others when I first started volunteering in diabetes – before I was working in it – because I could see that there were people with diabetes making a real difference to the lives of others with the condition.
It’s a word that I attach to people standing up, showing up and being counted. I asked on my FB page about the word, and someone said they like it because it not only refers to the person, but also the actions they are taking (thanks for that gem, Cathy).
But while it’s a word that I feel relaxed with, it doesn’t seem to be sit all that comfortably with other diabetes folks around the globe. (Which is, of course, fine. We can use whatever words we want to describe ourselves and what we do.)
I’m not sure if it is a cultural thing, or if it is just a preference. I’ve learnt that some languages don’t have a word that literally translates to advocate, but someone from Sweden told me she uses the English word, because it most adequately describes what she does. And in some places, people are very reluctant to use the word to describe themselves. After I asked about it, a number of people contacted me privately to say that they would like to use it for themselves, but they are worried about what others may think. Interestingly, they were all from the same part of the world.
Last month, I was an invited speaker at an event for people with diabetes in South Africa, and I was asked to speak about how the DOC has been a source of support for me in my years with diabetes. The event was titled Diabetes Influencers Summit. Now THAT’S a word I’m NOT comfortable with! I spent the first few minutes of my talk explaining why I’m prickly about the word and how I see what I do as advocacy, not influencing, and that I consider myself an advocate, not an influencer.
In my mind – and of course this is just my own assessment – influencers are building a brand for themselves, while advocates are more focussed on community. There is NOTHING wrong with building a brand – we all do it to a degree. But the advocates that I met and followed when I first started hanging out in the DOC were the ones that were truly all about community. They’re the ones I engage with now.
I don’t know any advocates who have made a squillion from their advocacy work. I don’t do sponsored posts here (or on any other of my socials). If I have been given product and then choose to write about it, I mention that in my wordy disclosure statements at the end of posts (and frequently throughout them as well), but I have never received money for what I have written, even though I am contacted almost daily with offers. I am a freelance writer, so I get paid to write elsewhere, but that’s my side hustle, writing is my job, and I should be paid for that.
No one has to call themselves an advocate – because of course that’s fine! – but I am saddened when those of us who do use the word are criticised, or considered to be ‘above our station’. (Ugh – just writing that makes me feel sick. Aussies baulk at class systems.)
Being an advocate doesn’t mean that I think I speak for others. I have never heard another diabetes advocate share their story with the message that they are representative of everyone. It also doesn’t mean that the issues that are important to me MUST be important to others – or that they’re the most important issues. I like to think that many of those issues that I’ve spent 20 years advocating for – access to healthcare, drugs and technology; PWD being recognised as experts in our care; respect from HCPs; the importance of using language that builds us up, rather than tears us down; working to diminish diabetes stigma; the philosophy of ‘Nothing About Us Without Us’; highlighting the need for more research about women’s health and diabetes – are universally acknowledged as issues that, if addressed and improved, can mean better outcomes for others with diabetes. But, these are my things and #YDA(dvocacy)MV.
Last week, I attended the Shifting Gears Summit which was coordinated and hosted by the Consumers Health Forum of Australia*, and the word ‘patient leader’ was used a lot. I realised that I was bristling with the term leader, not necessarily because I object to it, but more because I know how others would react if we started using it widely. I wonder why I feel that way. I happily and easily acknowledge many diabetes (and other health condition) advocates as leaders in what they do, knowing that they too may cringe with the label.
And yet, others working in the healthcare space are considered leaders – and usually, quite rightly so. We recognise HCPs, policy makers, hospital administrators, researchers and industry representatives as leaders in what they do, however the term seems to not be quite so comfortably applied to those of us with lived experience. But surely our experience and our role should be equal when all stakeholders are engaged. Otherwise, are we just there as window dressing? When an HCP offers their opinion on a diabetes issue, it does not necessarily mirror that of all HCPs, and yet no one questions their right to share that opinion. But despite this, they will be identified as leaders in their field. Why is that not also afforded to diabetes advocates?
It is definitely worth noting that I have rarely, if ever, seen, heard or had pushback from the HCPs I’ve worked with at the term advocate, or even leader. In fact, on a number of occasions I have been horribly embarrassed with the words – the very kind words – that have been used to introduce me. I’m always very touched that they see me in that light, but I am horrified at how other people with diabetes might react to their words. Why do some people with diabetes (myself included) want to distance ourselves from these descriptors?
Is it because in most cases people who are doing the sort of work we do are unpaid volunteers? Or is it because the status of the ‘patient’ is considered below that of others working in the healthcare space? Is it because there is no formal qualification needed to become an advocate?
Whatever it is, I don’t think we do ourselves any favours, or any favours in the endeavour to ensure the lived experience voice is considered as important – if not THE most important – in discussions about diabetes. In fact, that sort of rhetoric does nothing more than keep us in our place – that of a measly patient who can do no more than share their own tales of woe. When we say, or are told, ‘You’re only telling your story’, that devalues the contribution of advocates. It’s already hard enough to be heard, but then to be told that our story doesn’t mean much is offensive and harms us. I would never think to tell another PWD that, and it saddens me that others do.
We don’t have to label ourselves in any way we don’t feel comfortable, and we can describe ourselves and what we do in diabetes how we would like. I’ll keep throwing around the word advocate, and use it to describe myself. And continue to elevate the people with diabetes in the community who I see as being advocates, too.
*DISCLOSURE
I received a scholarship to attend the CHF Shifting Gears Summit after applying through an open submission process. Registration was paid for by CHF. I was not paid to attend.







