
You are currently browsing the category archive for the ‘Conferences’ category.
New technology gets me very, very excited so it was with great interest that I sat through the Abbott symposium showcasing their new FreeStyle Libre glucose monitoring device. Two and a half hours later and I was desperate to get my hands on one of these new devices.
Abbott call this their ‘flash glucose monitoring system’. It’s not continuous glucose monitoring as we know it. There is no integration between pump and sensor device. This is different.
Click here to read about how this device works, but basically, there is a sensor worn under the skin (positioned on the upper arm). The sensor, a white little disc, is about the size of a twenty-cent coin. A ‘reader’ is scanned over the sensor to give a glucose reading. That’s it. And there is no calibration required. The sensor lasts 14 days and Abbott says that this system eliminates the need to do finger prick tests.
That’s right – no more jabbing a lancet into your fingers. No more inserting a strip into a device, taking a blood sample, wiping it on the strip and waiting five seconds for the meter to count down and give you your number. Instead, just a swipe of the reader for an immediate result.
I should point out that the reader does also double as a BGL and ketone meter. At the symposium, it was mentioned that a finger prick test is recommended during periods of high variability.
Okay – so that’s all the good stuff. But I do have a couple of concerns.
First up, let’s talk about how it looks. (Yep, this is where I am being shallow.) There is no doubt that the sensor in this system is small. In fact, it has a tiny profile – only millimeters high. However, it is white and noticeable and has to be worn on the upper arm. I know that if I were wearing it, I’d be spending a lot of time explaining what the little white disc stuck to my arm is all about, and that would start to annoy me pretty quickly. I didn’t get a chance to ask why it couldn’t be worn elsewhere, but plan do to that when I visit the Abbott stand during the conference.
The cost of this device is yet to be announced in Australia. In Europe, the sensors will be around the €60, which, using today’s exchange rate, equals about AUD$86. This is not affordable tech. This is not going to be within the reach of most people. And that means, that once again, we have a situation where people with diabetes don’t have access to the latest, most convenient technology.
Also yet to be announced is the release date for the Libre in Australia – again this is something that I will be asking about later this week, however I suspect that the team here won’t be able to give me much idea about that. I might need to wait until I get home to get a better idea of when it will be available for Aussies. I do want to point out that the Abbott EU team should be commended in having given a sneak preview of the device to a significant number of peer leaders. How fantastic to have people with diabetes talking about this – and talking about the real experience of using the device – rather than us having to rely solely on the glossy collateral and impressions of HCPs.
But despite any concerns, make no mistake – this is a game changer. This tech has the potential to redefine self-monitoring in ways that we’ve not seen yet. For me, the benefit of not having to prick my finger to check my BGL is a huge, huge bonus and I know that there are many people who find this the thing they hate most about diabetes management.
This is exciting. I want it, and, at the risk of sounding like Veruca Salt, I want it now!
DISCLAIMER
The symposium I attended was sponsored by Abbott. I was not paid to attend the Symposium nor to write about this product. Abbott has not supplied me with any products in the FreeStyle Libre range. This blog post is just my impressions based on what I heard at the Symposium I attended and from people with diabetes who have been using the device.
I sat in the Qantas Club Lounge fighting back tears as the kiddo sent me text messages saying she would miss me. There were tears when I left, but my mum assured me that she was okay within about five minutes. (There’s a double-edged sword for you – happy that she is okay, but, dammit, couldn’t she be upset a little longer?)
I was hoping to drown the sadness of three weeks without my little girl with the excessive food and booze on offer in the lounge, but a stupid BGL of 17.3mmol/l (hello stress) saw me nibble on some nuts, drink half a glass of sparkling wine and avoid the dessert table. Missed opportunity.
By the time I boarded, my CGM was showing a much nicer number and I settled in for the long flight. As usual, I was asleep before we took off and managed to get in five hours of sleep, waking only because my pump was vibrating. (At that point, I felt I needed to explain to the person next to me why the little box in my top was vibrating and what it was for and I have diabetes and it’s telling me that my blood sugar is above it’s high limit because I’m stressed when I’m in transit and I miss my nine year old daughter and I wonder when the wine cart will be around.)
I am not afraid of flying – never have been. But I loath being in transit. It stresses me out and that sends my BGLs soaring. I bolused a little and upped my basal rate a touch.
When food arrived, I took two mouthfuls of the chicken-rice-vegetable combination that seems to make up pretty much every airline meal and held on to the chocolate bar. My CGM graph was pretty stable for the remainder of the first leg.
At Dubai airport, I set of every alarm possible going through security and was escorted to a private room to be patted down by a female attendant.
‘I’m wearing two medical devices – one here (I patted my chest) and one here (this time, I patted my abdomen where my CGM is inserted). I can show you if you’d like.’
After playing diabetes show and tell, I collected my things and moved through the airport, finding somewhere to have a coffee and regroup before the final flight. (And avoid accidentally buying a Hermes bangle.)
A two hour lay-over and I boarded the plane for Vienna. Thirty minutes in and off went my alarm warning me that my BGL was dropping too fast. I treated the impending low and fell asleep for a couple of hours, waking for a meal (another two mouthfuls!) and rounded out the flight with a couple of movies.
Checking into the hotel, I realised it had been 26 hours in transit door to door.
Travelling with diabetes has it’s challenges. I never travel now without wearing CGM because I like being able to pull out my pump and see how I am tracking. I love that I can respond to arrows before the number becomes problematic. This is, of course, the beauty of CGM all the time, but being able to stop having to deal with a nasty hypo while cruising at 35,000 feet in a cramped space is convenient beyond belief. Equally, being warned about the ‘about-to-happen-in-transit-stress-highs’ before they become horrid, socks on teeth, needing to wee every five minutes hypers is fabulous – for me and the person I’d be climbing over to get to the loo!
So, now, I’m in Vienna. The first strudel and schnitzel have been consumed. I’m jet lagged beyond belief. But my BGLs are over their in-transit-stress. Everything is how it should be and I’m ready for EASD!
I’ve learnt many things at the diabetes conferences around the world I’ve been lucky enough to attend. One of those things is that Conference Hypo Syndrome (CHS) will get me every single time! (There may be no documented evidence that this is a real thing. But believe me. IT’S.REAL.)
The Melbourne Convention and Exhibition Centre is a huge venue – just like most similar conference facilities around the globe. As I rush between presentations, meetings, finding the speakers’ room and catching up with people for coffee, I inevitably run (okay, walk) what feels like the equivalent of a half-marathon. In heels.
Over the weekend, I went through some old photos from other conferences I’d attended. At just about each and every one of them, there is at least one photo of me downing juice, eating glucose tabs or throwing down jelly beans.
Last week at the ADS-ADEA conference I smugly thought I had it all worked out. On day one, I got up and straight away lowered my basal rate a little, as I anticipated a crazy day activity ahead. I had it spot on! Not a hypo to be seen for the whole day.
I even knowingly explained CHS to a colleague attending her first conference who was shocked at just how many times she’d gone low that day. ‘Of course!’ I told her. ‘You’ve been running around all day in between sessions.’ The next day, she lowered her basal rates which resulted in a much nicer day of BGLs.
On day two, I was presenting as part of a symposium at the rude time of 8.30am. I had it all planned. I would get up nice and early, alter my basal rates (this time with some consideration to the fact that I’d be running on adrenalin in the morning as I prepped for my talk) and then would re-adjust it after my talk. ‘I’ve got this CHS thing sorted’. I thought to myself.
Stupid, stupid, STUPID girl.
Actually, it probably would have all been clever and worked out perfectly had I not had a crashing hypo at 3am. Or the nosebleedingly-high rebound that woke me at 6am. By the time I got to the conference centre, my basal rate had indeed been adjusted – but to help with the post-hypo high to avoid me doing my presentation with what would feel like a pair of grubby sports socks in my mouth, and the need to run to the loo every two minutes.
With my presentation done, I was back in range. I thought about the day ahead – more running around the cavernous centre – and adjusted my basal rate accordingly.
I spent the next hour or so catching up with people; popping in to hear grabs of different sessions; traipsing around the Expo hall to check out the exhibitors and being interviewed by a news crew from Diabetes Educators Update.
After my interview, I realised I had hardly any recollection of what I said. I was assured by the interviewer that I had answered everything appropriately and confidently, but when someone asked me what I’d spoken about, I couldn’t really remember details. I checked my BGL and realised that CHS had struck again.
I spent the day catching hypo- and rebound-tails until I got home and managed to get things smoothed out. I slept through the night, woke in range and set my basal rate for the day ahead. And was pretty much fine for the final day of the conference.
I’m presenting at another conference next week back at the Melbourne Convention Centre. Fingers crossed that I wake on the day of my presentation after a restful night’s sleep, with an in-target BGL and can put my CHS cure into plan. Because I know that if diabetes behaves itself (ha!) then it works. It’s just when diabetes is being a little shit that it all goes rather pear-shaped!
Last week, I spent three days attending and giving presentations at the annual Australian Diabetes Society-Australian Diabetes Educators Association (ADS-ADEA) Scientific Meeting, here in sunny Melbourne. It was a huge week with record attendance and the conference ‘felt’ big. I’m being a little lazy here, but I think that the best way to capture everything I want to share is to use dot points. Here goes:
- Congratulations to the ACBRD team for their symposium on day 1 – Diabetes Distress and Depression – Facing Challenges, Bringing Solutions. Special shouts out to Professor Jane Speight and Dr Christel Hendrieckx who were able to really focus on the ‘solutions’ part of this session.
- Overall, it was really pleasing to see an increased focus on mental health and behavioural research at the conference. Finally, the message that diabetes is absolutely not just about numbers seems to be getting through.
- And for that reason, it’s terrific to see presenters giving really practical advice about how to address mental health issues. Huge, huge points to Christel (again), Jane (again) and Dr Carol Silberberg for not only stating what the issues are, but actually providing take-home tips for clinicians to actually use. Mental health can be a tough topic to broach – especially if HCPs feel they don’t have the tools to deal with it – but thanks to presentations by these three, there was some really hands-on advice that has the potential to help HCPs change their practise.
- I called it when it was launched, and I’ll say it again: The Enhancing Your Consulting Skills resource developed by ADS is going to change the face of educating HCPs (endocrinology trainees) about diabetes. The ADS Symposium on the Thursday morning highlighted again just how valuable this resource will be. I was honoured to be invited to present at this session, and once again would like to thank the team responsible for considering the ‘consumer perspective’ throughout the development of the resource, and continuing to do so.
- Further to that, I hope I wasn’t too rude to the GP who informed the panel that we had forgotten ‘the most important person in the team – the GP’. I was trying to be respectful when I reminded him that actually that title goes to the person with diabetes. I may have failed.
- We need to talk about Dr Silberberg’s slides about clinicians not liking their patients. It was so, so interesting and gave such an insight into the clinicians’ minds. But that’s a whole other blog post! (Stay tuned…..)

- Great presentation from Emma White and Jesuina Noronha from Monash Children’s about some research they’ve conducted on sexual health knowledge, attitudes and beliefs in adolescents and young adults with type 1 diabetes. Some very interesting findings were presented. And Emma finished off with a bit of Salt n Pepa’s Let’s Talk About Sex. That girl rocks.
- I was a little disappointed that at the Technology 101 session on the final day, there was not a single consumer presenting. I understand the importance of discussing how HCPs use technology in their practice and applications for e-health. But many consumers are way ahead of the curve here and could have provided some very interesting insights about how technology can be used to connect (with other PWD as well as our HCPs), communicate, and gather, collate and share information.
- Even though the Consumer Outreach day was held on the final day of the conference, this is really the first time that I have felt that there has been a real consumer presence for the entire conference.
- While we’re on this topic, a special shout out to OzDOC guru Kim Henshaw for her outstanding tweeting throughout the conference. I was unable to get to nearly as many sessions as I would have liked due to meetings, but following her tweets gave me a pretty good insight into what was going on in the sessions I missed.
- Congrats to the organising team for stepping up this year with social media exposure. It was great that in the lead up to the event, there was a section on the website about using SoMe at the conference, a dedicated hashtag that was promoted throughout and twitter walls around the conference facilities (usually showing the faces of the consumer advocates in attendance who were busy tweeting).

- It would, however, be great to see more HCPs tweeting. Most came from consumer advocates and the ACBRD team. Perhaps a couple of ‘tweeting 101’ sessions over lunchtime would work to get some more people on board?
- Why is this important? Because the reality is, if it wasn’t for the few of us tweeting at the conference, most people would not have a clue about the sessions. How many people with diabetes have time in their appointment to ask if their HCP attended the conference – and what they learnt?
- A tiny suggestion to the organising team that they look at programming. Frequently, there were two or three sessions on at the same time that I would have loved to attend, and then sessions where there was nothing of particular interest. I heard this complaint from quite a few people (so it’s not just me!!). Perhaps some more consideration about spacing of sessions and spreading out the topics of interest to attendees.

- The Exhibition Hall at conferences is always a treat. This year, the battle for most enticing exhibit (in my books, anyway) went to the Lilly team who not only had the best (free) coffee, but also a sweets stand where they were dishing out little cups of lollies to attendees who stopped by. Very useful for those of us experiencing Conference Hypo Syndrome.
- Also seen in the Expo hall were people handing out nuts . They got angry at me when I said I wouldn’t write about their product. ‘But they’re just nuts’, one of their reps said to me. Indeed they were.

- But the bestest thing of all in that hall was not the free coffee or free lollies. No. It was a French poodle called Gabrielle who was there with the Paws for Diabetics team. More on that to come too.
- Weirdly, on the first day I found myself in the wrong Expo hall looking at tractors. Not relevant at all; just weird.



Well. that’s ADS-ADEA for another year. I’m going to finish up with this slide that Dr Jennifer Conn used in her presentation during the Type 1 Diabetes Consulting Skills symposium where she used this perfect quote from Elliot Joslin.
If you jump on Twitter and search #ADSADEA2014 you’ll find all the tweets from the conference. GO!
I’ve been at the Australian Diabetes Society-Australian Diabetes Educators Association Annual Scientific Meeting this week. It’s been a big few days with some really interesting sessions, terrific opportunities to catch up with people, trying to avoid (unsuccessfully) Conference Hypo Syndrome, and a gorgeous poodle called Gaby.
Today is the final day of the conference and it’s the first ever Consumer Outreach day. I’m really pleased to be spending the day with some inspiring diabetes consumer advocates who are all about promoting the ‘patient voice’.
I’ll be writing about it next week. But in the meantime, it’s Friday and for some reason I’ve had this Tom Lehrer song going through my head. Enjoy!
Next month the annual ADS-ADEA Scientific Meeting will be held in Melbourme. This is the leading diabetes conference in Australia and attracts diabetes healthcare professionals from all over the country and boasts a program of outstanding local and international speakers.
This year, for the first time, there will be a consumer stream as part of the conference. This is really exciting because it seems that finally, after many years of petitioning (by petitioning, I mean whining), people with diabetes are actually involved and encouraged to attend.
Details of the Consumer Outreach day are below.
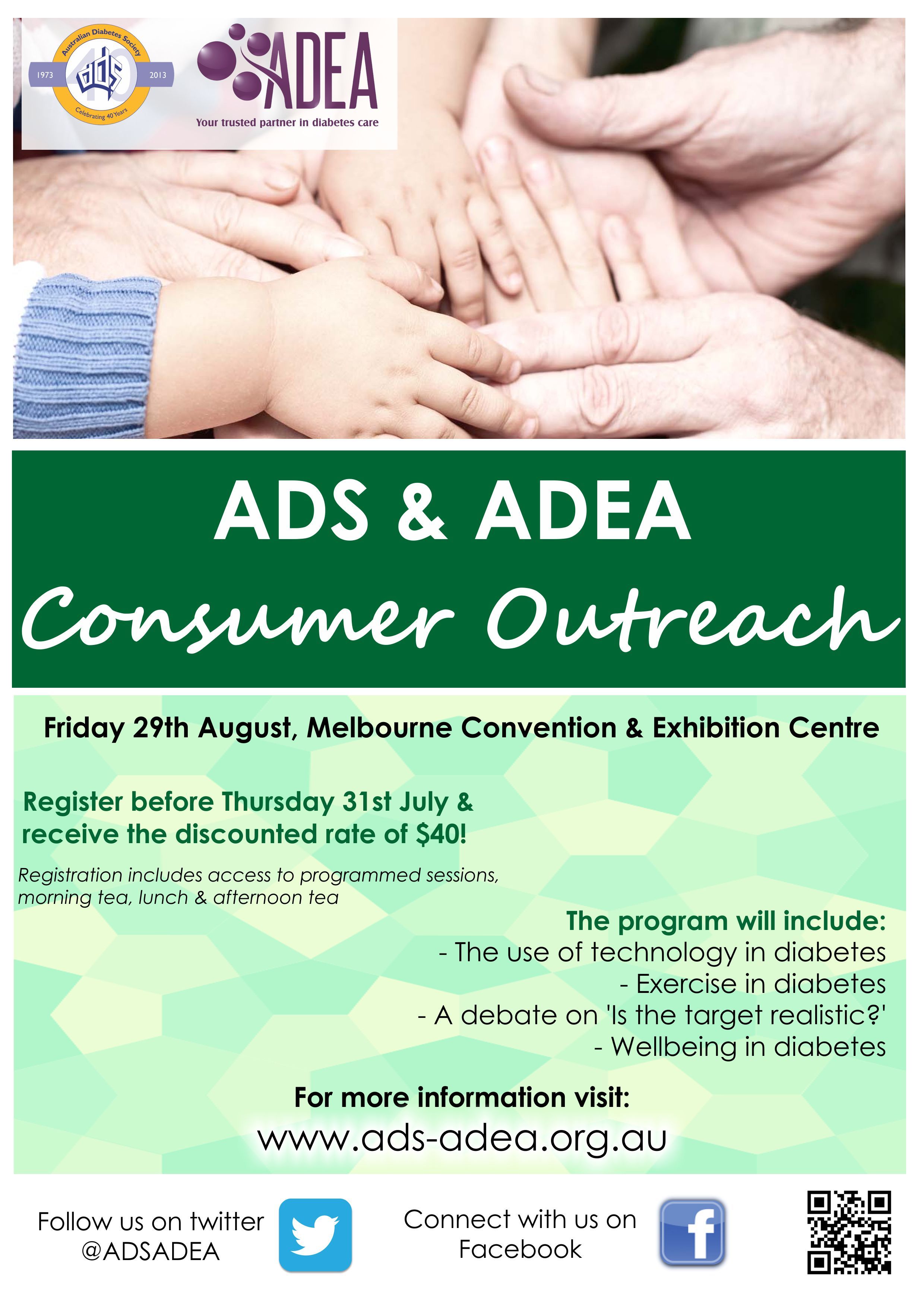
Someone has commented to me on Facebook that registration should be free for consumers and whilst I understand the reasoning behind that, I also know the costs involved in putting on a conference of this magnitude. I also know that sponsorship dollars are tight at the moment. I would urge anyone who wants to attend, but cannot afford it, to contact their local diabetes organisation and see if there is any way they can contribute to the costs.
I also know that having an event during the day on a Friday may not be ideal for many who work. But that’s the reality – conferences are held during the week. If you have any time in lieu owed, or an annual leave day you are prepared to take, this is a great way to spend it! Not only will you get to hear some interesting presentations, but it will be an opportunity to hang out with some incredibly awesome diabetes people.
Peer support for the win!
SCHOLARSHIPS AVAILABLE
#OzDOC will be providing two scholarships to cover the cost of registration for the event. To apply, jump on Twitter and send a direct message to @OzDiabetesOC. Make sure you include your email address in your message. You’ll then receive an application form. See you there!
DISCLAIMER
I am on the organising committee for the Consumer Outreach program. I am not receiving any payment for my involvement in this committee; however, my registration fee for the entire conference has been covered. I am also an invited speaker at the ADS-ADEA conference (at both the healthcare professional and consumer sessions and I have been involved in the submission of two abstracts that have been accepted for presentation at the conference).
At last year’s World Diabetes Congress (WDC), it was terrific to see a significant number of ‘consumers’ attending. For the first time in Australia, people with diabetes were directly encouraged to attend a scientific conference.
However, there was much disappointment that people living with diabetes who had registered to attend were unable to access the Exhibition Hall.
Expo Halls at conferences are an endless source of interest and excitement. I am usually registered as a speaker so I have full access to conference Expo Halls and it is during my wanderings that I find out about the latest and greatest in technology and treatment therapies. I get to speak with reps from the companies and ask questions that are usually not addressed in the glossy brochures, and, most importantly, I get to pick up and handle new devices to see how they feel in my hands, fit in my handbag (always returned!) or sit in my bra (it’s where I wear my pump; not trying to steal anything!).
The frustration at WDC was that as well as hosting the displays for pharma companies, the Expo Hall also accommodated device companies. Consumers couldn’t get in there to see the latest meters or pumps.
And here is the problem. In Australia, we have the Therapeutic Goods Act 1989 (the Act) which states that advertising of prescription-only medications to consumers is prohibited. However, it is okay for devices to be promoted directly to patients.
The Act is out-dated and it’s time that we revisit the current ban on promotion of drugs to people with health conditions. Why, as a person living with diabetes, can I not speak with the pharma company releasing a new insulin? Why can I not ask their reps about side effects and drug profiles and why the new medication is better or how it is different to what is already on the market?
The truth of the matter is I can find this information anywhere I want. A quick visit to Professor Google will provide me with the answers to any questions; patient blogs will explain the consumer perspective and an image search will even show me the packaging of the medication. When the Act was written, it was 1989 and the internet was not in the palm of everybody’s hand.
But today? Today such restrictions are ridiculous and only promote the idea that the people actually living with whatever health condition the medication has been designed to treat are too stupid/too ignorant/can’t be trusted with this hallowed information.
The ridiculous thing is that even if I can see and read about and ask questions to do with drugs and new therapies, I can’t simply go and buy them. I can’t rock up to Mae, my gorgeous pharmacist, and ask her for the large pack of whatever new drug I’ve just read about.
There is still the ‘middle (wo)man’, the doctor. But what is so terrible about me going to see my doctor and asking about a certain therapy? How is saying ‘I’ve read about this newly listed medication and I was wondering if it is something that would work for me?’ going to do anything other than empower me and encourage a balanced and consultative relationship with my HCP?
The current system reinforces all the things that patient advocates are trying to break down: out-dated ideas that the keepers of knowledge must only be healthcare professionals and that patients will be told what to do. And then do it. It forgets who is actually driving the bus that is my healthcare. Me!
Additionally, the Act as it stands now only serves to hold back real consumer involvement and engagement at scientific conferences. I don’t subscribe to the archaic ‘conferences aren’t a place for patients’ attitude held by many out-dated HCPs. We should be looking to events such as Doctors 2.0 and You for how to bring together patients and HCPs. We should be looking to the ADA conference which has a significant number of consumers in attendance – all of whom are freely permitted to wander the Expo Hall. We should be moving away from the ‘us and them’ approach so entrenched in Australia.
I first heard of the International Diabetes Federation’s (IDF) Young Leaders in Diabetes (YLD) Program when I attended the World Diabetes Congress in Dubai in 2011. There, I met some of the young leaders and heard about the program’s aims and intentions.

Alex Silverstein at the opening ceremony of the World Diabetes Congress in Melbourne last December. He’s usually less elaborately painted up!
I knew just how valuable and important this program would be when I first met Alex Silverstein in Chicago last year. Alex was the first President of the YLP and I could see why he had been selected to take on this role in the program’s early years. He’s smart, dynamic, passionate about the cause, funny and just a downright nice guy – I’m blessed to call him a mate. I’ve been lucky enough to meet up with him again at other conferences, including in Melbourne where he handed over the presidency to the equally awesome Keegan Hall.
In the lead up to the World Diabetes Congress in Melbourne last year, the YLD representatives spent some time together working with diabetes advocates and HCPs for their Leadership Training. They discussed global diabetes issues, how to effectively communicate and advocate were covered. I was invited to attend the session on social media use and was amazed at the enthusiasm and commitment in the room. The program involves 132 young people from 70 countries around the world, each with a different story about life with diabetes.
We need advocates with strong voices and the IDF should be commended for bringing together this group. Under the direction of Debbie Jones and Paul Madden and a smart and dedicated faculty, this program provides a voice for young people living with diabetes from around the world, many of whom would otherwise not have the opportunity to tell their stories and advocate the needs of their peers. Many are focusing their energies on highlighting issues such as access to insulin in countries where this life-saving drug is considered a luxury and the associated costs prohibitive.

The Aussie YLD contingent (plus an old bag).
Our Australian representatives on the YLD program are three of the most intelligent young women I’ve had the pleasure to meet. Ashley, Stephanie and Rachel did us all proud in Melbourne at the IDF Conference. They continue to be advocates for young people with diabetes in Australia through the YLD Program as well as the Diabetes Australia Young Leaders Program. Ashley is a regular blogger and has recently been involved in setting up a Facebook page to bring together young adults with type 2 diabetes.
See some of the young leaders in action in this great new video.
I am very fortunate that my job allows me to do a bit of interstate and international travel. Working for a not-for-profit means that while there are some opportunities for attendance at conferences, finding sponsorship is necessary if I want to attend all the conferences and meetings that are worthwhile and beneficial to my job.
Last month, Johnson and Johnson kindly sponsored my travel to Barcelona for the EASD conference, specifically to attend its second annual European Bloggers Summit. As the only person from Diabetes Australia lucky enough to be given an opportunity to attend the conference, I knew that I would be waving the Australian flag enthusiastically as I spoke about our experiences with diabetes social media and blogging. I searched out all the relevant, social media-focussed sessions and made sure I could get to them.
The day after arriving, I attended an IDF symposium about how social media can improve the lives of people with diabetes. The symposium was on the Sunday before the Tuesday start of the EASD meeting, so unfortunately, it wasn’t as well attended as I fell it should have been.
Given my recent presentation at the ADS/ADEA conference, I was very interested to hear this session – especially the presentation by Claire Pesterfield because as well as being a PWD, she’s also a diabetes nurse. Claire made some really interesting and valid points about how difficult it is for HCPs to jump on the social-media-as-support bandwagon when in most hospitals sites such as Facebook and Twitter are blocked by the hospitals’ IT people. It’s not really all that easy to tell people about great online support networks if the ‘red screen of death’ pops up every time you try to log on to one of them. I’ve been told that this situation is mimicked here in Australia.
We also heard Paul Buchanan (moderator the GBDOC tweet chats) speak about his recent (ridiculous, crazy, lunatic) arrival in Barcelona. From Brussels. On a bicycle. Paul and his group Team Blood Glucose were part of the Mobile Health Grand Tour – made up of a group of people who forgot that there are planes, trains and automobiles available to assist in the 2,400km journey from Brussels to Barcelona. Paul spoke about how social media and new diabetes technologies were employed on the ride. Interesting stuff!
 The Euro Bloggers Summit ran on the Tuesday and Wednesday. It was a couple of days of workshops and presentations which covered how we could improve the numbers of people reading our blogs and ensure that we have the right ‘look and feel’ to them so that they were attractive to readers.
The Euro Bloggers Summit ran on the Tuesday and Wednesday. It was a couple of days of workshops and presentations which covered how we could improve the numbers of people reading our blogs and ensure that we have the right ‘look and feel’ to them so that they were attractive to readers.
While the formal presentations were interesting and provided me with a lot to the think about, the thing that was the most valuable was the time spent speaking and networking with the other bloggers. There was a common theme in the room. While we like to think that there are people reading our blogs, it’s not really about the numbers. The real reason we all do what we do is because we are trying to connect with others who are going through the same things. We’re hoping that someone will read what we write and say ‘I thought I was the only one. But I’m not. I don’t feel so alone anymore’. We are telling our stories and sharing our fears and hopes while we look out for people who can share their stories with us.
Social media has the ability to remove all the things that get in the way of us feeling connected. We don’t worry about geography and thanks to translating software, language barriers can be broken down. Even pesky time-zones differences seem easily surmountable.
Being in the room with people who are doing the same things as me is an incredible privilege. Getting to hear about their work and their lives is an honour and I am grateful for every opportunity I get to learn from them. We need to start creating more opportunities like this in Australia. The World Diabetes Conference is the perfect chance for that to happen. Please take advantage of the fact that this significant diabetes meeting is being held in Melbourne and that there is discounted registration available to consumers. I’ll be there and I really hope to see some of you too!
Disclaimer
Johnson & Johnson covered my travel and accommodation costs so I could attend the Animas European Bloggers Summit. They were also kind enough to cover registration costs to the EASD meeting. There was no expectation that I would write about the Summit (or them). As part of this arrangement, I will be presenting for them at their booth at the World Diabetes Congress in Melbourne in December. You should come along and heckle me!
I attended the ADS/ADEA conference last week in Sydney just for one day to present at a technology and healthcare symposium (more on that soon).
It was one of those crazy days that started long before the sun rose. I can’t be chipper at 6.30am as my travel companion realised as he greeted me in a very cheery manner only to be met with a steely gaze and pronouncement of ‘I’m yet to have coffee’. It sounded like a threat!
After my presentation, I made the most of a couple of hours at the conference and caught up with as many people as possible. I’d arranged about eight ‘we’ll chat at the conference’ meetings and ended up seeing four people.
I only made it to one session apart from my Symposium and it was a debate.
I love a bit of debating. Those who know me won’t be surprised to know that I was in the debating team when I was at school (Renza nerd fact #3569). But the topic at the conference made me a little uncomfortable and that was before anyone even opened their mouths!
‘It’s our fault if our patients’ HbA1cs are too high’
I don’t like the word ‘fault’. Blaming people for being outside their diabetes targets rarely does anyone any good. As the people living with diabetes, we don’t like to be blamed or told off if we’re not meeting targets, so blaming our HCPs doesn’t make much sense to me either.
Nonetheless, I went along to see what was said.
First up for the affirmative – Cheryl Steele. Now, as far as I’m concerned, Cheryl Steele is wonderful. She was one of the first people I saw present about diabetes when I was first diagnosed with diabetes and she has inspired me ever since. She is a favourite speaker of the T1 Team at DA-Vic, not only because she does a brilliant presentation EVERY SINGLE TIME, but also because of her tell-it-like-it-is manner. And the fact that she is living with type 1 makes her even more awesome! She changed hats a few times yesterday whilst giving her presentation –sometimes speaking as a CDNE and other times as a PWD. And the confusion about anagrams was one of her points.
The affirmative team’s argument was that until HCPs stopped moving the goal posts, provided better tools for management and stopped disagreeing on what they were telling people with diabetes, then yes, they had to consider taking the blame for their patients higher than target BGLs.
The negative said there was no way that HCPs could be blamed – and were at great pains to point out that they weren’t blaming the PWD. Except there were times that they came pretty damn close – as evidenced by this tweet:
I felt a little uncomfortable at times during the debate. Although it was very tongue in cheek and there was great spirit throughout the session, there were moments that I wondered just how much truth was in the silliness. It is a little like the ‘oh-we’re-just-joking’ comments about patients lying about filling in BGL record books.
I know that by and large the HCPs in the room are there for the PWD (I was sitting next to my endo and I know that’s definitely the case with her), but I do get a little concerned at the lack of understanding about what life with diabetes is all about when the negative team thought that dealing with a life-long chronic health condition is kinda like taking a course of antibiotics.

Was I being a little too sensitive? Possibly. Am I expecting HCPs to get it wrong? Again, possibly. But as a consumer advocate, I am on heightened alert to make sure that there is compassion, understanding and respect being directed towards PWD at all times. I’m not sure that was necessarily the case throughout the debate last week.
Next time, I’d love to see a debate between HCPs and PWD. Now THAT would be worth paying money to see!






