
You are currently browsing the category archive for the ‘Awareness’ category.
I am always interested to hear from friends overseas about how they access their diabetes supplies. In some places, discussions, negotiations and, it seems, arguments with insurance companies are required before product is delivered; in other places, people with diabetes require a prescription from their HCP to purchase consumables as well as medications. And, in other places, access is so limited and sporadic there are no processes in place to guarantee supply of the things we need to manage diabetes.
In Australia, the process is actually quite simple. A diagnosis of diabetes means that a person is eligible to be registered on the National Diabetes Services Scheme (NDSS). Once registered, PWD can use the NDSS to access most diabetes (non-drug) consumables.
The supply of insulin (or other diabetes medication) here is part of the Pharmaceutical Benefits Scheme (PBS). A prescription is required from a doctor and that is taken to a pharmacy to be filled.
In my experiences, insulin is not always kept in stock, so I make sure to call ahead and have it ordered in for me. Most people with diabetes I know do the same thing – many have been caught out thinking that we could simply show up, hand over our prescription and be given the insulin (after being warned about how it needs to go into the fridge NOW – RIGHT NOW).
The NDSS is an initiative of the Australian Government. Diabetes Australia has, for the last 28 years, administered all aspects of the NDSS, which apart from product supply and delivery also includes information and support services for people registered on the Scheme.
When I need BGL strips or pump supplies or needles, I can access whichever products I choose to use by either ordering over the phone, online, or at an NDSS outlet, which could be downstairs at work (see disclaimer), at a hospital, community health centre or, most commonly, a pharmacy.
Sounds easy-peasy-lemon-squeezy, and for me, generally it is.
The NDSS rules and regulations are all set out by the Department of Health and then carried out by those actually distributing products. It’s for that reason that there are limits on the quantity of product you can purchase in one hit. Again, I’ve not had a problem with that. I had a form filled in by my endo a number of years back that stated I use above the upper limit of strips. I am therefore able to order more than the 900 strips per 180 days that is standard. (For those doing the maths at home, that is five strips per day. This is what is recommended as a guide by many HCPs. Of course, diabetes does not operate to a guide, which is why there is the flexibility to order more if required.)
I have recently noticed quite a few people online complaining that they are having difficulty accessing the quantity of product they require.
So, what do you do if you have this problem? The first thing to do is to remember where the rules and regulations come from. Of course it is frustrating to be faced with someone telling you that you are unable to have as much product as you need – especially if you are ordering within the limits, but even if you are ordering outside of that quantity. But don’t shoot the messenger. A pharmacy assistant telling you that you can only order 180 days of strips or needles is just doing their job. (It’s a completely different issue if they are telling you that they will only give you one or two boxes – that is not okay!)
You can write directly to the NDSS or even better, to the Commonwealth Minister of Health. Be clear and concise about why you need to be able to order the quantity you require.
This is also the time to remember that your local member is there to serve you.
Remember that if you are writing to an MP, they may not have the understanding of diabetes that you do, so use generic terminology – and don’t use ‘diabetese’. Keep it simple and try not to get bogged down in detail.
If you believe that you are not able to access what you need – the actual product and/or the product in the quantity you require – there is something you can do about it. That something is not bitching and moaning on social media, by the way. It’s taking action and actually doing something that will result in change.
I have written before that there are going to be some changes in the next twelve months with NDSS product supply. There is absolutely no reason to believe that the subsidised scheme is under threat, however the changes will certainly mean that the way we have accessed diabetes supplies in the past will change.
FUN BIT! Disclaimer
I work for Diabetes Victoria and Diabetes Australia. The majority of the work I do is funded from the Registrant Support Services part of the NDSS. This is a different funding stream to Product Supply and Delivery.
It was a lovely morning – a lazy weekend sitting in a local café, drinking fabulous coffee, skimming through the papers and discussing the Amy Winehouse doco we’d seen the night before. The kidlet was still being spoilt by her grandparents, and Aaron and I were making the most of a leisurely breakfast.
We were at one of our favourite cafes in our area. The coffee is consistently excellent, the food is great and the owner is one of the nicest people I have ever met. Being in his café is one of my favourite things to do on the weekend. (Plus they make the most amazing home-made marshmallows. Totally bolus worthy!)
We finished up after sneaking in a second round of coffees, and meandered to the front of the store to pay.
‘They look awesome,’ the guy ahead of us was saying to the barista, pointing at the delicious-looking fudge-y, chocolate brownies on the counter.
‘Yeah; they are really great. So sweet. You get diabetes just looking at them.’
The next noise was the sound of my head spinning and my hair whipping around.
‘No you don’t,’ I said – loudly enough for them both to hear. The customer turned around and the barista looked at me. I was a little terse, but not rude.
‘I mean it. Really, they are so sweet,’ said the barista.
‘Doesn’t matter how sweet they are. You still won’t get diabetes eating them. You really shouldn’t say that. It’s not true.’ I turned to Aaron. ‘I’ll be outside. I’m done here.’
And there it is. Again. The stupid, ignorant, insensitive, offensive, throw away comments about diabetes. Comments that also happen to be untrue.
At Nova the night before, we watched the heartbreakingly sad story of Amy Winehouse in the brilliant, but harrowing, documentary Amy.
This incredibly talented young woman was hounded by the media as she dealt with addiction. And at the moment when she most needed support and help, late-night television show hosts thought it was amusing to make fun of her. They thought it was hilarious to comment on her alcoholism or weight loss or drug abuse. They thought that a vulnerable young woman who was falling apart was a great target for their cheap jokes.
And apparently, diabetes is too.
It is not funny. People who are living with health conditions are not a punch line. Diabetes is not here to use as a material for a cheap joke. The condition that I work so bloody hard to keep in check – every minute of every single day – is not a chance for you to try to be witty (which, incidentally, you are most likely not!).
All of that came flooding to my caffeine-fuelled mind as I stood there, waiting to pay the other morning. ‘Am I overreacting?’ I asked Aaron when he walked out of the cafe. ‘No. Not at all.’
People who are dealing with health issues – no matter what they are – need support. We need people to try to understand what we are doing. We occasionally need to be reminded that we are doing the best we can.
It’s actually quite simple. Diabetes is not a joke. Stop thinking it is.
Amy Winehouse singing The Girl from Ipanema is a thing of beauty. Here it is.
I recently gave a short presentation on wearable medical devices that provide constant, real time data, and what that means for people on a day-to-day, minute-to-minute basis.
I had a slide that was a word cloud, including some of the (non-sweary) words I use regularly.

Being conscious that the crowd were not all necessarily diabetes-savvy, I focused on the data aspect and what that means for me emotionally more than the technicalities of the technology.
Afterwards, over tea and Arnott’s cream biscuits (Kingstons FTW!), I spoke with a (non-diabetes) healthcare professional – a GP who had never seen either an insulin pump or CGM before.
‘What great technology! It’s like you don’t have diabetes anymore,’ the GP said to me, clearly not having listened to any of my talk – especially the bit where I said sometimes tech could actually be more overwhelming and a constant reminder of my diabetes. Or the part where I said that as much as I love the devices, I still need to drive them and do a lot of work.
I shook my head gently and smiled. ‘I wish. And one day, I hope it will be like that. But this tech, whilst terrific, is part of my arsenal in the significant self-management tasks I do each day to manage my diabetes.’
He looked far less impressed.
‘Oh,’ he said. ‘So it’s not all that great?’
‘No, no. I’m not saying that.’ I wondered if he had actually heard anything I said. Because as much as I talked about the overwhelming side of the technology and all the data, I spoke a lot about how useful it is too.
‘It’s complicated,’ I said. ‘Sometimes I love this tech; other times I hate it. But mostly, I am glad I can use it the way I want.’
I munched on my Kingston biscuit, thinking. ‘I guess it’s kind of how I feel about my mobile phone. I love it – it means that I can reach everyone I want to whenever I want to and they can reach me. It means I can check Twitter and Facebook to see what everyone is up to. I can check the weather. I can receive emails and reply to them all the time. It’s great, right?’
‘And it’s a pain in the arse as well. Pretty much for all the reasons that it is great. But regardless, I wouldn’t be without it.’
He nodded. ‘I think I get it now. That’s an analogy that makes sense to me. Diabetes is so huge. A lot of it doesn’t make sense.’
It was my turn to nod. ‘So much of the time I am guilty of forgetting that not everyone gets the intricacies of life with diabetes. I try not to have expectations that people know about it, but find it difficult to explain. Maybe I need to come up with non-diabetes explanations.’
‘Like ‘life is like a box of chocolates?’ Forrest Gump managed to do it.’
I laughed. ‘Actually, that’s a pretty good analogy for diabetes too,‘ I said.
He thanked me and walked away, promising to learn more about diabetes technology.
I spoke with a few other people, ate another (couple of) Kingstons and got ready to leave. As I was collecting my things, I heard the GP speaking with someone else. ‘The technology is great,’ I heard him say. ‘But it can be frustrating at times. Kind of like the frustration from having a mobile phone and being reachable all the time.’
I smiled to myself and left the room.
(Well, yesterday, but whatever.)
There has been lots of discussion about what happened 94 years ago yesterday – on 27 July 1921. University of Toronto scientists Fredrick Banting and Charles Best successfully isolated the hormone insulin. Today, that means that I am alive and kicking, 17 years after my islets stopped making any.
It means that type 1 diabetes treatment moved from being a starvation diet and not much else, to injecting a drug that was life giving and life saving.
It means that I take a drug that while giving me life, is also lethal and if not dosed carefully and with great consideration can cause terrible side effects.
It means that people with diabetes don’t die terrible, agonising deaths simply because they were diagnosed with diabetes.
It means that I need to be able to do crazy calculations to ensure what I put into my body completely and utterly imperfectly mimics what those with functioning islet cells do completely and utterly perfectly.
It means that there is a treatment therapy that gives us hope and life and allows us to live – sometimes very long, long lives.
It means that each and every day I feel fortunate to have been born when I was and not 100 years earlier.
It means I take for granted that I have access to a drug that keeps me going.
It means that there are far too many people around the world who still do not have access to the drug I take for granted. And 94 years later, that is not good enough.
It means that it was 94 years ago – 94 years ago – since the discover of insulin to treat diabetes and we are still without a cure.
And it means that I wonder when there will be the next breakthrough that is as significant and meaningful and life changing and life saving as what those two Canadian scientists discovered 94 years ago.
But mostly. It means that I live with hope. Hope that those scientists are somewhere working away, and perhaps – just perhaps – are about to find that next big breakthrough.

Any day that sees a BGL of 32.4mmol/l is not going to be fun.
It happened around midday on Saturday. It came from nowhere. In range BGLs at waking. Trip to a new café for a breakfast of delicious coconut-y porridge and milky coffee. A quick trip into the city to buy a birthday present for one of the kid’s friends who was having a party that afternoon.
So far, so fun.
And then, suddenly, nausea hit.
At that point, I realised just what a bad diabetes day it was about to become. I’d changed handbags that morning and my BGL meter hadn’t made the transfer. I was CGM-less as well, so apart from the nausea and a slightly dry mouth, had no idea if I was high – or just how high I was.
Thankfully, we live less than a ten minute drive from the city. We got home, me holding the bag that had contained the present close by in case the feeling of nausea became the real deal.
We made it home. I checked my BGL. Oh yes, I was high. So, so, so high.
I calculated a bolus does of insulin and used a disposable syringe to jab it into my stomach. I changed out my cannula, line, cartridge and insulin, inspecting the old one I’d just removed. It looked absolutely fine. And I’m sure it was fine. I set a slightly elevated temp basal, resisting the urge to set it at 200% – effectively giving myself double the usual dose – and sternly told myself that I needed to let the bolus do its thing. Slow and steady was the way!
Then the vomiting started. Then it ended.
And then I fell asleep. And a couple of hours later, I awoke feeling fine. Well – as close to fine as one can be after a couple of hours of unexplained, very high BGLs and the muscle pain that comes from throwing up.
My BGLs returned to range gradually. The nausea was gone. The mild ketones I’d had earlier disappeared, flushed out with lots of water.
Not fun. At all. But I did what I planned to do that night, brushing off the looks of surprise from my friends when I mentioned the day I’d had. They probably wondered why I was up and out and not curled up in a ball under the doona. There were moments I wondered that too.
If I was to stop every time I had a diabetes thing happen, I’d never get up I thought, but didn’t say it out loud because it doesn’t really make sense to people who don’t have diabetes.
It’s what we do. We get on with things. Because diabetes throws so much our way that we just learn to accept it and push forward. We do it without much fanfare. But sometimes – sometimes – I kinda do feel like I deserve a medal. And yesterday I got one after I did the 5km in Run Melbourne!

Medals for the family!
Can you think of any other medical condition where removal of a treatment is threatened?
I was thinking about that question a couple of nights ago, in my hotel room in Sydney, at 2.30am, getting over a hypo, after chugging OJ, messaging people, tweeting and reading pages of my book. I couldn’t fall back to sleep.
In diabetes, we (still; STILL?) hear of HCPs threatening to remove pump therapy from people who are considered to not be meeting expected results.
Let’s not even open the can of worms asking who actually has set those results, or if the PWD had any input into the decision making process around targets, or if too much focus is being given to a number.
No. Let’s instead just focus on the fact that some PWD are (still; STILL?) being told that their chosen treatment option for their life long health condition will be removed from them as punishment because they are being ‘bad’.
Now, I love my insulin pump, but let’s remember what it is. It’s a little box that delivers insulin. Okay – a little, highly-sophisticated magical box that delivers insulin, but nonetheless, it’s an insulin delivery device.
It would be the same as saying to someone who is using insulin pens that because their A1c has increased, (often the reason behind the threat of pump removal), their pens were being confiscated and they would have to use disposable syringes. Or, people using disposable syringes would have to use glass syringes with needles needing to be sharpened.
Crazy, right? There is no way that we would consider that okay. It’s actually laughable.
Of course, people with type 2 diabetes are not immune to the threats of diabetes management, however in this case, it is threatening to add treatment rather than take it away. People with type 2 are often told that if they require insulin injections to treat their diabetes it is because they have failed with other treatments.
Making threats about diabetes management options is bullying. Holding the tools we need to live well with the condition over our heads as rewards or punishment is not okay. It is scary and unfair and sends the wrong message.
Earlier this week, Aaron and I saw the Melbourne Theatre Company’s production of the play ‘Death and the Maiden’. It was fabulous – amazing performances – and if you are in Melbourne and looking for a night at the theatre, get tickets! Here is the Schubert string quartet by the same name, which is providing my background music in the office today. Have a lovely weekend.
‘Really?’
How many times have I heard that response when people find out I have diabetes. An upwards inflection, a little surprise, a lot of confusion. I know that it is an involuntary response – perhaps because people weren’t expecting that to be the explanation to their question about the pager-like device I have just pulled from under my clothes, or the little beeping machine on my lap, or why I am guzzling jelly beans like a woman possessed.
We know that it is because diabetes is an invisible condition. Unless you look for the signs, who can tell that my beta cells stopped working over 17 years ago? And even if you did look for the signs, what exactly would you be looking for?
We talk a lot about how frustrating it is to have a condition with limited visible signs. It means that people say things that annoy and frustrate us, or that people have limited knowledge and understanding of just how much work goes into living with a condition that has such limited visible signs.
But sometimes, I am grateful for the invisibility. Sometimes, it is nice to be able to package up all the diabetes things and keep them hidden away – to tuck my pump more securely in my bra and make sure that there is no tubing poking out and to hide away my BGL meter and jelly beans and glucose tabs. It’s nice to not give people a reason to ask.
I know how exhausting it can be answering the myriad questions people have about diabetes. Of course, a lot of the time they are downright rude, but most of the time, they are borne from nothing more than human curiosity. Sometimes it’s great to try to explain what living with diabetes is about to someone who genuinely wants to know, or to share my diabetes story.
How we each deal with our diabetes is highly personal. We can shout about it from the rooftops, we can whisper about it amongst only those we choose or we can remain silent and not share with anyone. And it’s all okay – it’s okay to change how we want to speak about it.
This last week, a lot of people have asked me about the green band around my wrist. I explain that it is from a conference I attended for people with diabetes.
‘You have diabetes? Really?’
I nod. And sometimes I sigh. Or smile. But I answer their questions. I gently point them to kind ways to talk about diabetes. I highlight how there is no one way that people with diabetes look. I bust some myths and ask them questions about their diabetes knowledge.
And frequently, I hear them say, ‘I had no idea about that. I had no idea that there was so much involved in diabetes management.’
I look at them and take it in. ‘Really?’ I ask. Because I wonder how they could NOT know.
This time last week, I was sitting on a plane, flying back from Friends for Life. As we’d booked this trip at the last possible moment, I was not travelling the long LA – Melbourne leg with Aaron and the kidlet. We hadn’t managed to all get on the same flight and my trip (booked though work) and theirs didn’t coincide.
So I had a lot of thinking time and kept trying to put into words what the Friends for Life (FFL) experience was for me. I found myself tearing up quite a bit, and kept touching the green bracelet that was wound around my right wrist. It’s still there, and I find myself glancing at it when I am sitting in meetings, or as my fingers fly across the keyboard typing these words.
I had an idea of what I was going to experience at FFL. I have spent enough time with FFL alumni and read a lot about it to have formed an impression about what the week would hold.
I knew what to expect.
Excect I absolutely didn’t. I had no idea.
I expected it to be all touchy-feely. I expected lots of hugs. I expected a quiet understanding – of all and from all who were there. I expected to feel included and part of something and welcomed.
And those expectations were all met. Ten fold.
But what I didn’t expect was the sheer, overwhelming emotion of the conference.
And I didn’t expect the science.
Make no mistake. Friends for Life is a diabetes conference in the truest sense of the word. It is not a support group meeting – of course there is support, but it is much more than that – it is a scientific meeting with the focus very clearly on providing up-to-date, evidence-based, important information to people living with diabetes. It’s not dumbed-down – absolutely not! The information presented at FFL would not be out of place at the ADA scientific meeting I’d attended the month prior, or ADS-ADEA conference I am attending next month.
I didn’t expect an exhibition hall that was bigger than what I know I’ll see at the annual ADS-ADEA conference.
I didn’t expect that there would be announcements like the one Ed Damiano made about his work on the (brilliantly named, iLET) bionic pancreas. And when it was made, I didn’t expect the outpouring of emotion, of gratitude, of understanding, of hope.
And running alongside it – as part of it – are the sessions where you sit, and breathe and cry and nod and share your story. Or say nothing and just fill up.
This is not a cult-like gathering of the pancreatically-challenged and our support people. There is no sitting around feeling sorry for ourselves. Equally, it’s not a pep rally where we marched to the beat of the same drum, patting ourselves in the back. Every person at that conference has their own story and while there certainly are similarities, there are also differences.
Friends for Life challenged me. It made me feel uncomfortable at times. The discussions were not all easy and self-affirming. There were topics that I don’t regularly talk about, instead hiding them away in a chamber of my mind that I manage to keep locked away most of the time. I sat quietly in talks about how diabetes affects those around me. I struggled to share my story at times. But I did, often with hesitation, because talking about how diabetes impacts on Aaron and our beautiful girl hurts me in ways that make me feel like I am falling to pieces inside.
I didn’t walk out of all of those challenging sessions feeling great. But I felt validated and I felt less alone. And I understood better that it was okay to speak about those confronting issues, even if what I am feeling isn’t wonderful. I took away from those sessions the ideas and strategies other use and I feel better equipped to manage some of the more difficult aspects of living with diabetes in the family.
I attended FFL as a guest of Children with Diabetes (CWD). For years, I have been begging CWD President, Jeff Hitchcock to bring this event to Australia and while I did that with the idea that it would be great for people affected by diabetes to have the experience, I had no idea just what that experience would mean. I still am not fully cognisant of what the experience has given me.
My expectations weren’t met at Friends for Life. They were exceeded. And I hope that we can find a way to bring it to Australia so that as many people as possible can become part of the FFL family.
A huge thank you to Jeff Hitchcock and the CWD Board for covering my costs to attend Friends for Life 2015.
 Some dot point facts:
Some dot point facts:
- It’s National Diabetes Week here in the wonderful land of Oz.
- It’s about all types of diabetes. Every. Single. Last. Type.
- 280 people are diagnosed with diabetes each and every single day in Australia.
- All types of diabetes sucks.
- No one asks to get diabetes.
And now some dot point observations:
- There is no merit in changing the name of the different types of diabetes. None at all.
- I am yet to hear a decent argument about why we should change the name of type 1 diabetes to something else.
- Having said that, if you can incorporate the word ‘unicorn’ into a new name for type 1 diabetes, I might get on board. Although probably not. I just want a unicorn.
- Many health conditions have ‘types’ and ‘sub-types’. There are five different types of lupus. Can you name them? Can you tell me how they are different? If someone said they have lupus, would you be able to engage in a meaningful discussion about their ‘type’ of lupus? I know I certainly couldn’t – and my mum has lupus.
- Quite frankly, I don’t care what type of diabetes the 280 people diagnosed each day have. It is all diabetes and it is all a condition that is significantly underfunded, a condition which carries horrendous stigma and a condition which is crap to live with.
- What I do care about is that there is increased awareness about all types of diabetes. I care that more research dollars are thrown at diabetes. I care that more healthcare professionals know about diabetes and about diagnosing ALL types, quickly. I care that people living with all types of diabetes have access to healthcare and devices and medications and support.
- The whinging and whining and bitching and moaning that is coming from some circles is tedious. Especially considering the whinging and whining and bitching and moaning is being done mostly amongst like-minded people so nothing is actually being achieved.
And finally, a comment:
Last week, I sat in on MasterLab, a two day advocacy workshop run by the wonderful Diabetes Hands Foundation. In the room were some of the most successful, vocal, passionate, smart diabetes advocates in the world. These are people who take their cause to government and make changes for people living with diabetes, who raise awareness about living with diabetes and raise funds to help support people living with diabetes. They do it without fanfare and without accolades. They just do it.
How many times do you think there was a discussion about the different types of diabetes? How many times do you think parents of kids with diabetes in the room tried to say how much tougher they have it than others with diabetes? Or people with type 1 diabetes complaining that no one understands why it is more difficult than type 2? How many times do you think that type 2 diabetes was demonised?
Not once.
Because those smart people in the room – the people who are respected and listened to in the wider diabetes space – know that there is no point in working against each other.
But you know what? I’ve been saying this for some time and there are people far more eloquent than I on the same page.
This is from (US-based) Diabetes Patient Advocacy Coalition (DPAC):
How will you share a unified patient voice for a disease as diverse as diabetes? (Type 1 vs. type 2, parent vs. child, etc.?)
DPAC has committed to the idea that diabetes doesn’t discriminate. We have no interest in promoting cross-type discord. There are benefits of numbers, passion, and reach in various parts of the diabetes community. We all benefit from all those skills. If an individual has an interest in raising their voice to help people with diabetes get access to safe and quality products and services in the United States, then we welcome them with open arms.
Divided we can be ignored. Together we make a difference.
And in her wrap-up of last week’s MasterLab, my friend Alanna wrote this brilliant blog post. And this closing paragraph:
We as a community need to stop putting our walls up. Nobody, not you, not me, not the president of the USA can advocate for change in diabetes care and treatment until we educate effectively. Defending your “type” and throwing the other under the bus is unacceptable behaviour, and is counter productive to creating positive change and a world without the financial, physical and emotional burden of diabetes.
I am calling on all of my readers, old and new to commit to never trying to defend your type, and only defending the human beings who are living with mal-functioning pancreases so we can really get to work.
Another friend, Kerri Sparling wrote this last year, speaking about the wonderful Walk with D initiative.
The diseases are different in their origin but so similar in how they map out physically, and more importantly, emotionally, and I wish I had known that earlier. I wish I had been more supportive of my type 2 peers. I wish I had known how they felt.
I have lost friends because of my stand on this issue. I have had arguments with people who think that I should be using this blog and my voice to advocate for changing the name of type 1 diabetes or rallying against people not understanding the differences between the types of diabetes. I have had people challenge me and ask me what I stand for – what my diabetes advocacy is all about.
The answer is simple. I am against diabetes stigma. I am against building up one type of diabetes at the expense of another. I am for access to healthcare and devices and medications for all people with diabetes. I am for a unified community. I am for the wonderful #OzDOC community which is a beacon in Australia of unity within the diabetes world, and congratulate Kim Henshaw in promoting an inclusive, supportive and downright fun platform for all people with diabetes to connect.
It doesn’t mean we have to agree on everything or all be focusing on the same issues. It just means that we work together and are kind to each other. #TypeAll
Gorgeous new James Taylor CD made its way into our home yesterday. Angels of Fenway is a favourite given that I was there just a few weeks ago.

National Diabetes Week is an important week for people living with diabetes in Australia. It is an opportunity to have all types of diabetes given attention and focus in the media and to talk about the significant health issue it is – for people living with diabetes, their families, and health systems.
And sometimes, messed up in the campaigns and the social media onslaught, we get sidelined by arguments and heated discussions, and we start to forget one of the real reasons this week is important: how diabetes affects those of us actually living with the condition.
Today, I helped launch a new report. The Diabetes MILES Youth survey was conducted last year and the results have now been published. The survey aimed to examine the impact of diabetes on young people living with diabetes and their families.
The report (which can be found here) shows that a quarter of young people living with type 1 diabetes experience moderate to severe depressive or anxiety symptoms. This image shows the top problem areas for girls and boys.
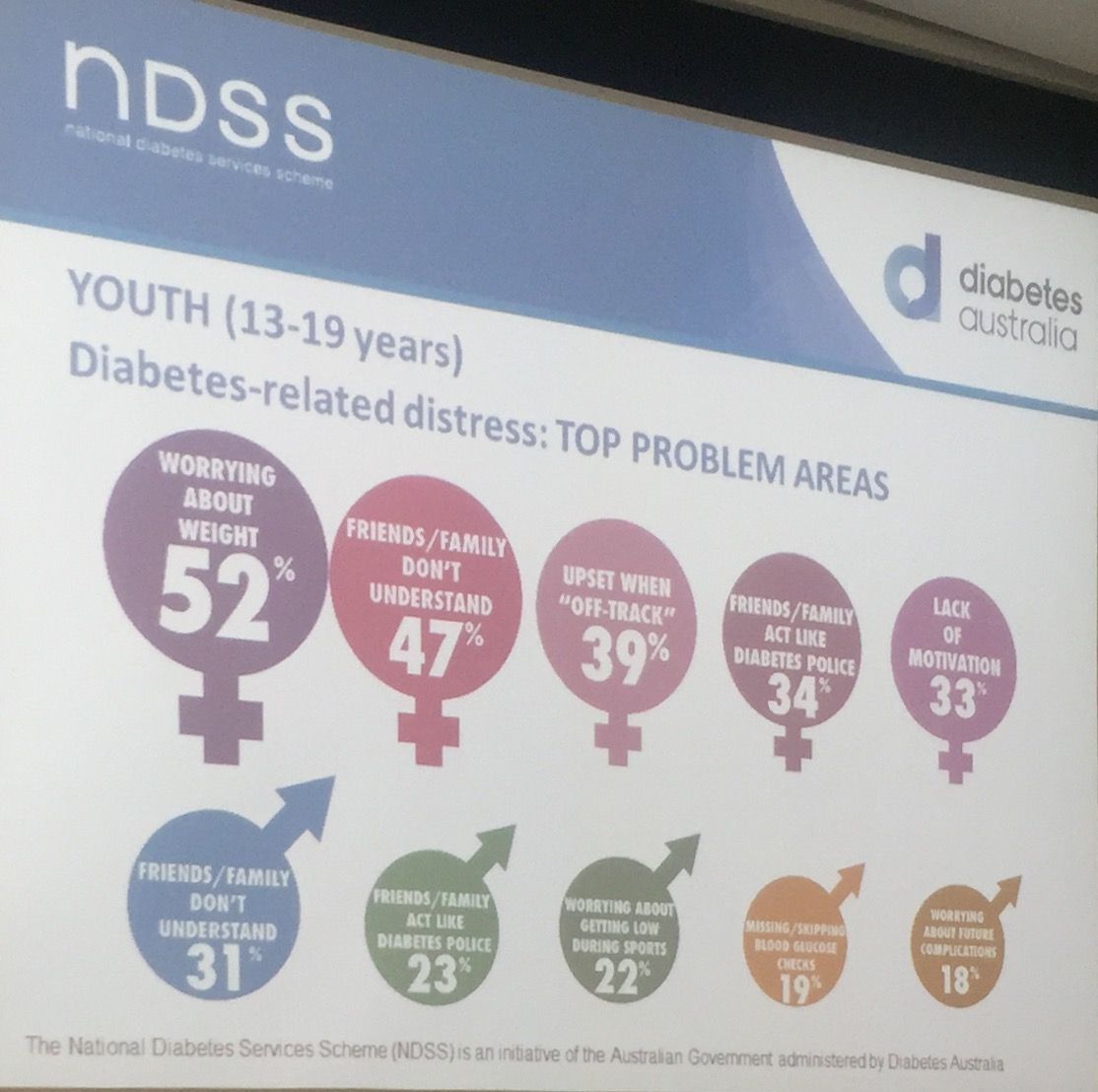
Today’s launch was incredibly powerful. Of course, we heard the statistics and heard how significant the problem is (a third of parents of children with diabetes reported impaired emotional well-being). And we heard about why this sort of work is important. But for me, and I suspect most people in attendance this morning, the most powerful moments were when we heard from Ryan Lange and Freya Wickenden, two young people living with diabetes. Both spoke beautifully about the role diabetes plays in their lives. Freya’s mum, Dallas, also spoke and shared some insights into parenting a child with diabetes.

As I said in my presentation at the launch – I can speak about this for hours and hours. I am a passionate advocate for all people with diabetes, but the vulnerability we see so often in young people with diabetes has meant that this has become a focus area of my work. But my words are insignificant and unimportant. It’s the words from young people living with diabetes that are central to understand what they are facing. Here is just some of what they told us.
The Diabetes MILES Youth report – was funded by the National Diabetes Services Scheme, and initiative of the Australian Government administered by Diabetes Australia. The study was conducted in collaboration with Australia Centre for Behavioural Research in Diabetes. The Diabetes MILES Youth project is part of the Young People with Diabetes National Diabetes Program for which I am Program Manager.






