
You are currently browsing the category archive for the ‘Stigma’ category.
It’s been a hot minute, hasn’t it. And by ‘hot’ I mean sweltering here in Melbourne. While my friends in the northern hemisphere are sharing snow photos, we’ve been dealing with days in the high 30s and 40s. (For my US friends – we hit almost 120°F this month. It was not nice.)
Anyway, now that the weather discussions are over, let me wish you all a belated happy new year. I’d like to say that I hope that your start to 2026 has been gentle and kind, but instead, picture me gesturing wildly at the world and shaking my head in despair.
I finished up 2025 feeling pretty damn exhausted and burnt out. But, really, who wasn’t feeling that way? There was a lot of good stuff that I could look back on, but the never-ending travel wore me out. I feel compelled to say that I know I am fortunate to do the work I do, and I love my job. Being able to work with people in the diabetes community who are making real change is a gift every single day. I would just be so happy if someone could find out a way for Australia to not be a 30-hour trip away from most of the places I need to visit.
I was lucky to have a three-week break over the Christmas/New Year period where I travelled no further than 5kms from my house, and I’ll have had a 10-week hiatus before I next find myself in an airport. Both of these breaks feel like a luxury!
But as we gear up for 2026, it’s undeniable that the global health world is in a mess and diabetes is not immune to that. I’m really pleased that some of my work will involve addressing issues that are important to people with diabetes. I’m beyond honoured to have been invited to give the Anita Carlson lecture at this month’s Psychosocial Aspects of Diabetes (PSAD) Conference (even happier that it’s being held in a regional city in my state and I only have to drive for an hour to get there!). I’ve called my lecture ‘Building Diabetes Healthcare from the Ground Up’ and it’s given me an opportunity to imagine just what diabetes healthcare could be if people with diabetes were actually centred and involved in its creation.
Next month the first Global Summit to End Diabetes Stigma is being held in Jaipur, India. Can you imagine hundreds of people with or working in diabetes coming together in one place to come up with meaningful and real strategies to end stigma? For disclosure purposes, this event is being funded via a grant from Breakthrough T1D (I work there), and I am involved in the planning of the event. It feels like a culmination of a lot of efforts highlighting the impact of stigma to get to a place where the diabetes world is ready to collaborate to end it. I’m so thrilled to be working for the organisation that has recognised that.
For me right now though, there is an overarching feeling that the world really is burning. While the US gets a lot of our attention, diabetes healthcare and access to insulin and care remains incredibly lacking in other parts of the world. As always, the most vulnerable in our world are impacted the most negatively. I don’t know about you, but a lot of the time I feel helpless.
Now it’s February, you may have once again seen that the annual Spare a Rose campaign has started. I think this is the fourteenth year of the campaign. I think back to what the diabetes community was like when Spare a Rose first started, and honestly, it feels very different to what we have today. I don’t know if a campaign like this would be started in today’s community. In fact, sometimes I find it harder and harder to find community and advocacy these days, as “influencer culture” takes hold.
And so, it’s worth remembering where Spare a Rose came from and the intentions behind it. It was a group of advocates in the US who wanted to give back somehow. I should point out that the advocates who started Spare a Rose had already given so much to the community. Many of them have taken a back seat to front-facing advocacy efforts but their legacies live on, even if fewer and fewer people see how they shaped the DOC. It’s diabetes advocates who have driven this campaign over the years and made sure that it has remained in the view of people with diabetes.
I have always loved the simplicity of Spare a Rose. The donation being asked for is small – US$5. For those needing a refresher, the idea is to give your loved one eleven rather than twelve roses and donate the saving to the campaign. In our house, we forgo flowers completely and recognise that empty vases are a small price to pay for making a donation to the value of a year’s worth of insulin.
I know that many are doing it tough these days. I also know that a lot of people who would have donated without a second thought in the past are unable to do so now due to changes of circumstances in so-called high-income countries.
But if you can support Spare a Rose by making a donation, please do. All funds go directly to the brilliant charity Insulin for Life, and each contribution makes a difference to a person with diabetes in a low-income country. If you can’t make a financial contribution, please share the website across your networks. Someone else in there might be able to donate. Every single dollar counts.
Click to donate!

Last week I was in Geneva for the 78th World Health Assembly (WHA78). It’s always interesting being at a health event that is not diabetes specific. It means that I get to learn from others working in the broader health space and see how common themes play out in different health conditions.
It’s also useful to see where there are synergies and opportunities to learn from the experiences of other health communities, and my particular focus is always on issues such as language and communications, lived experience and community-led advocacy.
What I was reminded of last week is that is that stigma is not siloed. It permeates across health conditions and is often fuelled by the same problematic assumptions and biases that I am very familiar with in the diabetes landscape.
I eagerly attended a breakfast session titled ‘Better adherence, better control, better health’ presented by the World Heart Federation and sponsored by Servier. I say eagerly, because I was keen to understand just how and why the term ‘adherence’ continues to be the dominant framing when talking about treatment uptake (and medication taking). And I wanted to understand just how this language was acceptable that this was being used so determinately in one health space when it is so unaccepted in others. This was a follow on from the event at the IDF Congress last month and built on the World Heart Foundation’s World Adherence Day.

While the diabetes #LanguageMatters movement is well established, it is by no means the only one pushing back on unhelpful terminology. There has been research into communication and language for a number of health conditions and published guidance statements for other conditions such as HIV, obesity, mental health, and reproductive health, all challenging language that places blame on individuals instead of acknowledging broader systemic barriers.
I want to say from the outset that I believe that the speakers on the panel genuinely care about improving outcomes for people. But words matter as does the meaning behind those words. And when those words are delivered through paternalistic language it sends very contradictory messages. The focus of the event was very much heart conditions, although there was a representative from the IDF on the panel (more about that later). But regardless the health condition, the messaging was stigmatising.
The barriers to people following treatment plans and taking medications as prescribed were clearly outlined by the speakers – and they are not insignificant. In fact, each speaker took time to highlight these barriers and emphasise how substantial they are. I’m wary to share any of the slides because honestly, the language is so problematic, but I am going to share this one because it shows that the speakers were very aware and transparent about the myriad reasons that someone may not be able to start, continue with or consistently follow a treatment plan.
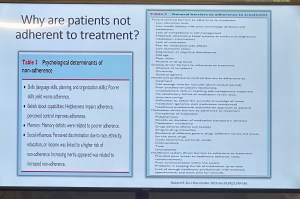
You’ll see that all the usual suspects are there: unaffordable pricing, patchy supply chains, unpleasant side effects, lack of culturally relevant options, varying levels of health literacy and limited engagement from healthcare professionals because working under conditions don’t allow the time they need.
And yet, despite the acknowledgement there is still an air of finger pointing and blaming that accompanies the messaging. This makes absolutely no sense to me. How is it possible to consider personal responsibility as a key reason for lack of engagement with treatment when the reasons are often way beyond the control of the individual?
The question should not be: Why are people not taking their medications? Especially as in so many situations medications are too expensive, not available, too complicated to manage, require unreasonable or inflexible time to take the meds, or come with side effects that significant impact quality of life. Being told to ‘push through’ those side effects without support or alternatives isn’t a solution. It is dismissive and is not in any way person-centred care.
The questions that should be asked are: How do we make meds more affordable, easier to take, and accessible? What are the opportunities to co-design treatment and medication plans with the people who are going to be following them? How do we remove the systemic barriers that make following these plans out of reach?
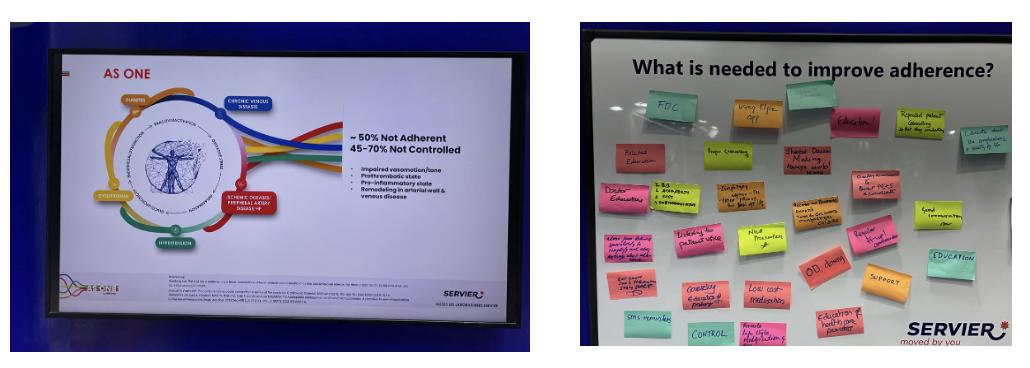
One of the slides presented showed the percentage people with different chronic conditions not following treatment. Have a look:

My initial thought was not ‘Look at those naughty people not doing what they’re told’. It was this: if 90% of people with a specific condition are not following the prescribed treatment plan, I would suggest – in fact, I did suggest when I took the microphone – the problem is not with the people.
It is with the treatment. Of course it is with the treatment.
The problem with the language of adherence is that it frames outcomes through the lens of personal responsibility. It absolves policy makers of any duty to act and address the structural, economic and systemic barriers that prevent people from accessing and maintaining treatment. Why would they intervene and develop policy if the issue is seen as people being lazy or not committing to their health?
And it means the healthcare professionals are let off the hook. It assumes they are the holders of all knowledge, the giver of treatment and medications, and the person in front of them is there do what they are told.
There is no room in that model for questions, preferences, or complexity. There is no room for lived experience. There are no opportunities for co-design, meaningful engagement or developing plans that are likely to result in better outcomes.
When the room was opened up to questions, I raised these concerns, and the response from the emcee was somewhat dismissive. In fact, she tried to shut me down before I had a chance to make my (short) comment and ask a question. I’ve been in this game long enough to know when to push through, so I did. I also don’t take kindly to anyone shutting down someone with lived experience, especially in a session where our perspective was seriously lacking. Her response was to suggest that diabetes is different. I suggest (actually, I know) she is wrong.
And I will also add: while there was a person with lived experience on the panel, they were given two questions and had minimal space to contribute beyond that. I understand that there were delays that meant they arrived just in time for their session, but they were not included in the list of speakers on the flyer for the event while all the health professionals and those with organisation affiliation were. There comments were at the very end of the session, and I was reminded of this piece I wrote back in 2016 where health blogger and activist Britt Johnson was expected to feel grateful that the emcee, who had ignored her throughout a panel discussion, gave her the last five minutes to contribute.
Collectively this all points to a bigger issue, and we should name that for what it is: tokenism.
I didn’t point this out at the time, but here is a free tip for all health event organisers: getting someone to emcee who is a journalist or on-air reporter does not necessarily a good emcee make. Because when you have someone with a superficial understanding of the nuance and complexity involved in living with a chronic health condition, or understand the power dynamics and sensitivities required when facilitating a conversation about long-term health conditions, you wind up with a presenter who may be able to introduce speakers, but you miss out on meaningful and empathetic framing of the situation. There are people with lived experience who are excellent emcees and moderators, and bring that authenticity to the role. Use them. (Or get someone like Femi Oke who moderated the Helmsley + Access to Medicine Foundation session later in the day. She had obviously done her homework and was absolutely brilliant.)
I know that there has been a lot of attention to language in the diabetes space. But we are not alone. In fact, so much of my understanding has come from the work done by those in the HIV/AIDS community who led the way for language reform. There are also language movements in cancer care, obesity, mental health and more. And even if there are not official guidelines, it takes nothing to listen to community voices to understand how words and communication impact us.
So where to from here? In my comment to the panel, I urged the World Heart Foundation to reconsider the name of their campaign. Rather than framing their activities around adherence, I encouraged them to look for ways to support engagement and work with communities to find a balance in their communications. I asked that they continue to focus on naming the barriers that were outlined in the presentations, and shift from ‘How to we get people to follow?’ to ‘How do we work with people to understand what it is that they can and want to follow?’.
Finally, it was great to see International Diabetes Federation VP Jackie Malouf on the program on the panel. She was there to represent the IDF, but also brought loved experience as the mother of a child with diabetes. The IDF had endorsed World Adherence Day and perhaps had seen some of the public backlash about the campaign and the IDF’s support. Jackie eloquently made the point about how the use of the word was problematic and reinforced stigma and exclusion, and that there needs to be better engagement with the community before continuing with the initiative.
One of the things of which I am most proud is seeing how the language matters movement has really made people stop and think about how we communicate about diabetes. Of course, there’s still a long way to go, but it is very clear that there have been great strides made to improve the framing of diabetes.
One area where there has been a noticeable difference is at diabetes conferences. I’m not for a moment suggesting that there is never negative language used at conferences and meetings, but the clangers stand out now and are likely to be highlighted by someone (i.e. #dedoc° voices) in the audience.
Earlier this month, the 75th IDF World Congress was held in Bangkok. Sadly, there was no livestream of the Congress, but it’s a funny thing when you have a lot of friends and colleagues (i.e. #dedoc° voices) in attendance. It meant that I had my own livestream. Sadly, the majority of what I was being sent were the language clangers.
But let’s step back a week or so to before the Congress even started. I was feeling horrendous and my brain was in a foggy, virus haze, yet I still managed to be indignant and vent at the horrendously titled ‘World Adherence Day’ which was being ‘celebrated’ on 27 March. Here is my post from LinkedIn, which has been viewed close to 12,000 times:

What I didn’t say in my post was that the IDF had eagerly endorsed the day with a media release and social media posts. My LinkedIn post took all my energy for that day, and I didn’t get a chance to follow up with the IDF. Plus, I assumed their attention would have been focused very much on the upcoming Congress.
Also, I hoped that it was a one-off misstep. I mean, surely the organisation had learnt its lesson after the Congress in South Korea when I boldly challenged incoming-president Andrew Boulton for his suggestion that people with diabetes need some ‘fear arousal’ to understand how serious diabetes is. You can see the video of my response to that at the end of this post and read the article I co-authored (Boulton was another co-author) about language here.
Alas, I was wrong. Just days before the Congress started, I saw flyers for this session shared online:

I was horrified and commented on a couple of the posts I saw. I was surprised to see some responses from advocates which amounted to ‘We can deal with it when we get there.’ Here are reasons that isn’t good enough. Firstly – not everyone is there, so all they see is the promotional of an event, comfortably using stigmatising language. It suggests that this language and the meaning behind it is okay. The discussion shouldn’t be happening after the fact. In fact, the question we should be asking is: HOW did this even happen? Where were the people with lived experience on the organising committee of the Congress speaking up about this? Did they get to see it before it was publicised? And how did the IDF miss it? This is, after all, the organisation that launched a ‘Language Philosophy’ document in 2014 (which sadly seems to be unavailable online today). It’s also the organisation that has invited me to give a number of talks about the importance of using appropriate and effective communication to IDF staff, attendees of the Young Leaders Program and as an invited speaker at a number of Congresses.
A major sponsor at the IDF Congress seemed to be very excited about the word adherence. In fact, it appeared over and over in their materials at the Congress. Here is just a couple of their questionable messaging sent to me by people (i.e. #dedoc° voices) attending the Congress:
I will point out that the IDF obviously understands the impact of stigma on people with diabetes and the harm it causes. There were sessions at the Congress dedicated to diabetes-related stigma and how to address it. In fact, I had been invited to give one of those talks. But what is disappointing is that despite this, terminology that contributes to stigma is being used without question.
I wasn’t at the Congress but from what I saw there was indeed a vibrant lived experience cohort there. #dedoc° had a scholarship program, and, as usual, there was a Living with Diabetes stream. However, I will point out that the LWD stream was not chaired by a grassroots advocate as has been the case for all previous LWD streams. It was chaired by a doctor with diabetes and while I am in no way trying to delegitimise his lived experience, I am unapologetically saying that this is a backwards step by the IDF. When there is an opportunity for a person with diabetes who is not also a health professional is given to a health professional or a researcher, that’s a missed opportunity for a person with diabetes. There were seven streams at the IDF Congress. All except for one are 100% chaired by clinicians and researchers. Only the LWD stream is open to PWD. I know that when I chaired the stream, the four members of the committee were diligent about looking through the entire and identifying any sessions that could be considered problematic for people with diabetes. It appears that didn’t happen this time.
All of this points to a persistent disconnect. It is undeniable that the language matters movement is growing, but it is still not embedded across the board—even within organisations that should know better. If we are serious about addressing stigma and centring lived experience in diabetes care, then language can’t be an afterthought or a debate to have after the posters are printed and the sessions are underway. It must be part of the planning and the review process. The easiest way to connect the dots is to ensure the lived experience community is not only present, but also listened to, respected, and in positions to influence and lead. We are long past the point where being in the room or offered a solitary seat is enough – the room is ours; we are the table.
Postscript:
I have written extensively on why language – and in particular the word ‘adherence’ – is problematic. It’s old news to me and to many others as well. This piece isn’t about that. But if you want to know why it’s problematic, here’s an old post you can read.
Disclosures:
I was an invited to give a talk about diabetes-related stigma at the IDF Congress in Bangkok, but disappointingly, had to cancel my attendance due to illness. The invitation included flights and accommodation as well as Congress registration. I was also on the program for two other sessions and was due to present to the YLD Program.
Other IDF disclosures: I have been faculty for the YLD Program for the last 10 years; I chaired the LWD Stream at the 2019 Congress and was deputy chair of the 2017 Congress.
Last week, at the ISPAD Meeting in Lisbon, I was lucky enough to catch up with remarkable diabetes advocate Jazz Sethi and together, we launched a new resource about #LanguageMatters and women with diabetes. Jazz and her team from Diabesties conceived this idea and worked with a number of women in the diabetes community to bring this resource to life and add it to the ever-growing stable of #LangaugeMatters resources. I was one of those women.
So, why do we need a specific document highlighting the challenges faced by women with diabetes, and how language can be used to help overcome these challenges?
Let’s talk about gender bias in healthcare.
Anyone who has even a mild interest in healthcare knows that gender bias is very real, and women do indeed face specific challenges. The situation is worse for women from different backgrounds, sexual orientations and gender identities.
This was the reason behind the International Diabetes Federation focusing World Diabetes Day activities on women and children back in 2017.
Here is just some of the information from that campaign, explaining issues faced by women:
- As a result of socioeconomic conditions, girls & women with diabetes experience barriers in accessing cost-effective diabetes prevention, early detection, diagnosis, treatment & care, particularly in developing countries.
- Socioeconomic inequalities expose women to the main risk factors of diabetes, including poor diet & nutrition, physical inactivity, tobacco consumption and harmful use of alcohol.
- Stigmatisation & discrimination faced by PWD are particularly pronounced for girls & women, who carry a double burden of discrimination because of their health status & the inequalities perpetrated in male dominated societies.
- These inequalities can discourage girls & women from seeking diagnosis and treatment, preventing them from achieving positive health outcomes.
Beyond diabetes, and more generally in the healthcare world, women’s health concerns are frequently denied, minimised, ignored or not believed. Women are gaslit into believing that symptoms are not real, pain is imagined and that we are overreacting. These attitudes can have serious consequences. Here’s just a sprinkling:
- This year, findings of the Australian-first #EndGenderBias survey found 2 out of 3 women experience discrimination in healthcare.
- A Danish study of 6.9 million people showed that diagnoses for diabetes came four-and-a-half years later for women than men; cancer is diagnosed in women 2.5 years after it is diagnosed in men.
- This World Economic Forum article about the women’s health gap highlights how far more women than men are not diagnosed for common health conditions.
- This McKinsey Report showed that when it comes to gender-specific health conditions, diagnosis rates differ. Eight out of ten women are undiagnosed with menopause, and six out of ten are undiagnosed with PCOS. Meanwhile, only three out of ten men with erectile dysfunction remain undiagnosed.
- Want more? Okay, here’s something from the UK showing that women are underdiagnosed, undertreated and under-represented in clinical trials directed at management strategies for cardiovascular disease, making their results less applicable to this subset.
Pivoting back to diabetes, this from a Lancet editorial:
- Compared with men, women with diabetes are disproportionately affected by depression and anxiety & have a lower quality of life, which can negatively affect attitudes towards self-management &, in turn, disease outcomes
- Women with type 1 diabetes have a 40% higher excess risk of premature death than men with the disease, and those individuals with type 2 diabetes have up to 27% higher excess risk of stroke and 44% higher excess risk of coronary heart disease.
- Women from high income countries are less likely than men to receive the care recommended by guidelines
And a recent study published out of Canada reported:
- Women with diabetes may face additional challenges related to gender-based discrimination and its impact on depression symptoms
- Stigma was more significantly perceived by women compared to men
None of this will be a surprise to anyone who is familiar with gender bias in medicine. Actually, none of this will be remotely surprising to anyone who has listened women share their experiences in healthcare.
And so, anything that can be done to address this is surely a good idea, right?
Well, IDF Europe thinks so! In this article, one of their recommendations for addressing gender equality in diabetes is: The development of specific approaches to diabetes prevention, education and care for women and girls. In other words, targeted, specific, tailored information is frequently needed to ensure that messages get through and issues are addressed.
Which brings us full circle to the #LanguageMatters and women with diabetes resource launched last week. A resource specifically for women with diabetes, by women diabetes. It identifies the issues and provides practical solutions to address them and shines a light on gender bias in diabetes care, asking that women are treated with respect and all our concerns are believed.
You’ll see that nowhere in this article have I denied that men with diabetes face challenges, or that men with diabetes could benefit from focused information and resources. And the new language resource for women doesn’t say that either. And yet, that was an accusation on the cesspit that is Twitter after a video was tweeted, where Jazz and I excitedly launched this new resource. Because ‘whataboutism’ is never far away.
Diabetes MattHERs has been widely shared on social media, with overwhelmingly positive responses. But here’s the kicker: the only backlash? Aimed at a woman. Men who shared it? Nothing but praise. Funny how that works. It’s almost as though there’s a different standard for women. Perhaps… I don’t know… could it be bias?

It’s never hard to find a source of diabetes stigma. Because sadly, it’s all around us. And right now, the source seems to be much of the discussion about the report from the Australian Parliamentary Inquiry into Diabetes.
Yes, I was very excited about the report last week when I was writing about the recommendations and accompanying content about increasing access to pumps and AID systems. That was incredible news, and it was terrific to see that the community-led efforts were met with such a positive outcome.
But the messaging more broadly hasn’t been so great and it’s very disappointing.
Disappointing, but not surprising really. After all, the inquiry was for diabetes and obesity. Last week, I said that people with T2D deserve the same attention as people with T1D when it comes to advocacy efforts and campaigns. Well, so do people living with obesity. When the inquiry was first announced, I remember reading through its terms of reference and feeling my heart sink. These are two separate and equally important health issues that need focused attention. And within that, diabetes itself comprises different types; again, all equally important and requiring specific attention.
But instead of giving diabetes the attention it deserved with an inquiry purely focused on highlighting what is needed to improve outcomes for those of us living with the condition and enhancing the health system to better serve us, we were given an inquiry that conflated two separate and significant health conditions. Something was going to get lost in this. And it seems that is diabetes.
Since the report was launched on Wednesday, a lot of media coverage has focused on one specific recommendation: the sugar tax. That was what was on the front page of The Australian, a segment on the Project and in a number of radio interviews. Also mentioned in this coverage was the recommendation about junk food advertising to children. As you can imagine, the commentary from the community has been pretty horrid and completely misinformed. If ever there was a time for not reading the comments, this is it.
I completely agree that a sugar tax is a good idea and have been saying so for years. I also believe that junk good advertising should be banned completely, especially for children, starting with TV and online advertising and extending to sponsorship of children’s sporting activities. Again, I have been involved in initiatives involving this for years. One of the reasons these measures are important is that they make healthier choices more accessible, which can reduce the risk of people developing obesity. And yes, obesity is a risk factor for T2D. However not everyone who is obese will develop T2D and not everyone who has T2D is obese. Yet this nuance is missed completely with simplistic messaging and grouping the two together.
And this nuance is important. As is pointing out that obesity is also a risk factor for many other conditions as well such as several types of cancer, liver disease, heart attack and stroke, high blood pressure, high cholesterol, osteoarthritis, sleep apnoea, mental health conditions, fertility problems and pregnancy problems. Not only T2D, so why is it included in an Inquiry about diabetes?
I shouldn’t be surprised by the media missing the mark completely, but that doesn’t mean that it doesn’t anger and upset me. Because efforts can be made to try to minimise harm and stigma from misreporting. I was asked to contribute to a media release this week about the AID work and I made it very clear that I would not be involved in anything where messaging could be seen as stigmatising. I provided a copy of language position statements and asked to see the release before it went out to make sure that it all aligned. I pointed out to the PR agency that I would publicly call out any media that came from this release if it was in any way stigmatising about any type of diabetes. Sadly, I don’t think there has been that level of care across PR and media groups. Without that care and attention the stigmatising tropes about diabetes, in particular T2D, are in overdrive.
But it’s not just the media. In the report itself, there is this statement: ‘There is a huge burden being placed on health resources by people with Type 2 diabetes’, a statement that clearly blames people with T2D for needing to use our underfunded, under-resourced, understaffed healthcare system. Absolutely no recognition of non-modifiable risk facts or social determinants of health. More stigma. More misinformation. More throwing people with T2D under the bus. And this impacts on all types of diabetes, whether we like it or not.
I really wish that as we are all tripping over ourselves to highlight this Inquiry report, we also stop to think about the messages about diabetes we are setting free into the world. So far, very little of what I have seen hasn’t made me cringe. Far too much has been stigmatising and harmful. We all have a role to play in ensuring that we do not contribute to diabetes stigma, especially when participating in commentary about and the media circus of a new shiny report being launched.

On November 14, the world will literally light up in blue to celebrate World Diabetes Day. And here in Melbourne, an event highlighting one of the most important issues in diabetes today will be held. The entire event will be dedicated to how the global diabetes community is coming together to work to #EndDiabetesStigma. And you can be there!

I’m delighted to be sharing the hosting seat with Dr Norman Swan, physician, journalist and host of Radio National’s Health Report. A veritable A-Team of people from the international diabetes community will be part of the event, sharing their experiences of diabetes stigma and why efforts to end it are so necessary and timely. There will be representatives from the global lived experience community, diabetes organisations and health professionals and researchers. You really don’t want to miss it!
For those able to attend in person, you’ll have a chance to catch up with diabetes mates. Any chance for opportunistic peer support is a great thing and I’m so pleased that I’ll be seeing diabetes friends that I’ve not seen for a very long time.
This isn’t only for Melbourne locals. There will be a livestream for people around the world to watch, share and be part of on social media. It’s free to attend and will be a great opportunity to see the diabetes world come together on a day dedicated to us!
Diabetes stigma is a hot button topic in the diabetes world. It has been for some time. I wrote just last month how stigma was one of the most talked about issues at ADA. That week, we also launched an Open Letter from the Diabetes Community, asking health professionals to join us in our call to stop diabetes stigma.
And behind the scenes, for all of this year, another exciting, BIG, project has been hatching and I’m so excited to share it today.
Earlier this year, in an unprecedented show of unity and determination, a group of 51 experts from 18 countries joined forces to pool our lived, research and clinical experience to address diabetes stigma and discrimination. Together, we’ve reviewed the scientific evidence and established an international consensus on 49 Statements of Evidence and Recommendations. The full report on this review has been submitted and is currently under review.
Excitingly, the group also reached a consensus on a Pledge dedicated to bringing an end to diabetes stigma and discrimination. And that’s where you come in! Everyone can sign to show your commitment stop the ingrained negative judgments, stereotypes, and prejudices that influence attitudes about diabetes, and contribute to the stigma so many of us face. This isn’t just for the community. We know there is sometimes an echo chamber as we say the same things to each other, over and over. We also know that while diabetes stigma is indeed prevalent within our community, we also need to tell the story of its harm outside the diabetes world.
Well, here’s an easy way to do both. Please sign the pledge and share details across your social platforms. You can sign as an individual, and we’d also love for you to see if your place of work, school, community group, hospital, church, sporting team, favourite cafe…basically anywhere that is likely to come into contact with people with diabetes (i.e. literally everyone!) would be interested in signing too.
This is a true community effort, with involvement from stakeholders from across the diabetes landscape, across the world. You won’t see logos anywhere, because this for and about all people with diabetes. The names of the people involved in the work so far is on the website.
Are you with us?

All too frequently, when talking about meaningful lived experience engagement, I hear about ‘Hard to Reach Communities’. A number of years ago, I called rubbish on that, putting a stop to any discussion that used the term as a get out of jail free card to excuse lack of diversity in lived experience perspectives.
‘People with type 2 diabetes don’t want to be case studies’ or ‘Young people with diabetes don’t respond to our call outs for surveys’ or ‘People from culturally and linguistically diverse communities won’t share their stories’ or ‘Folks in rural areas don’t come to our events’. These are just some real life examples I heard when asking why there was no diversity in the stories I was seeing.
See how the blame there is all on the people with diabetes? They don’t want, don’t respond, won’t share, won’t attends. It’s them. They’re the problem. It’s them.
I stood on stage at EASD in Stockholm last year and challenged the audience to stop using the term ‘hard to reach’. Because that’s not the case at all. The truth is that in most cases, the same old, uninventive methods are always employed. And those methods only work for a very narrow segment of the community.
I recently heard someone begrudge that all applicants who responded to a recent call out for a new committee were the same: white, had type 1 diabetes, city-dwelling. ‘Of course they are,’ I said. ‘That’s the group that loves a community advisory council and responds to an expression of interest call out on socials. They are able to attend meetings when they are scheduled, are confident to speak up and are willing to share their story, because they probably have before and received positive feedback for doing so Plus, they’re expecting everyone else at the table will look and sound just like them.’
But the lack of diversity isn’t the problem of the people who didn’t respond. It’s the problem of whoever is putting out a call and expecting people to reply because that’s how it’s Always Been Done.
This was a discussion at a meeting during last week’s American Diabetes Association Scientific Sessions. The #dedoc° voices were meeting with the ADA’s Chief Scientific Officer, Dr Bob Gabbay, and Vice President in Science & Health Care, Dr Nicole Johnson. The question about how to reach a broad audience was asked. At #dedoc°, efforts have been made to attract a diverse group of people to our scholarship program, and have, to a degree there as been some success. A glance at any one of the #docday° events, or scholarship alumni will see people who had not previously been given a platform within the diabetes community. But there is always more than can be done.
The discussion in that meeting at ADA mirrored many that happened throughout the week. And it’s not surprising that US diabetes advocate Chelcie Rice came up with the perfect way to explain how to do better at engaging with the who have previously been dismissed as ‘hard to reach’. He said: ‘You can’t just put pie in the middle of the table. Deliver the pie to where they are.’ And he’s right. Those tried and true methods that work for only one narrow segment of the community have been all about putting pie in the middle of the table, knowing that there will be some people ready with a plate and a fork. But a lot of people are not already at the table, or comfortable holding out their plate. Or maybe they don’t even like that pie. But we never find out because no effort is really made.
Chelcie once said ‘If you’re not given a seat at the table, bring your own chair‘ and I’ve repeated that quote dozens, if not hundreds of times. And his words ring very true for people like me who have felt very comfortable dragging my own chair, and one for someone else and insisting that others scramble to make room for us. But that metaphorical table isn’t enough anymore. Not everyone wants to sit at a table and we need to stop expecting that. Instead, it’s time to find people where they are – the places, the settings, the environments they feel comfortable and at home. That’s how you do engagement.

On day 2 of the American Diabetes Association Scientific Sessions, rushing between meetings, I overhead another attendee say this: ‘I’ve never heard so many people talking about diabetes stigma’. I turned to them, a bright smile on my face and said, ‘I know, right?’, (a phrase I only ever utter when I’m in the US).
Just a few hours earlier, Jazz Sethi and I had tweeted simultaneously, setting free an open letter from the diabetes community about diabetes-related stigma. You may have seen it; thousands of people have. And others have shared, commented and even translated it into different languages (I think we’re at 6 translations and counting). Here it is!



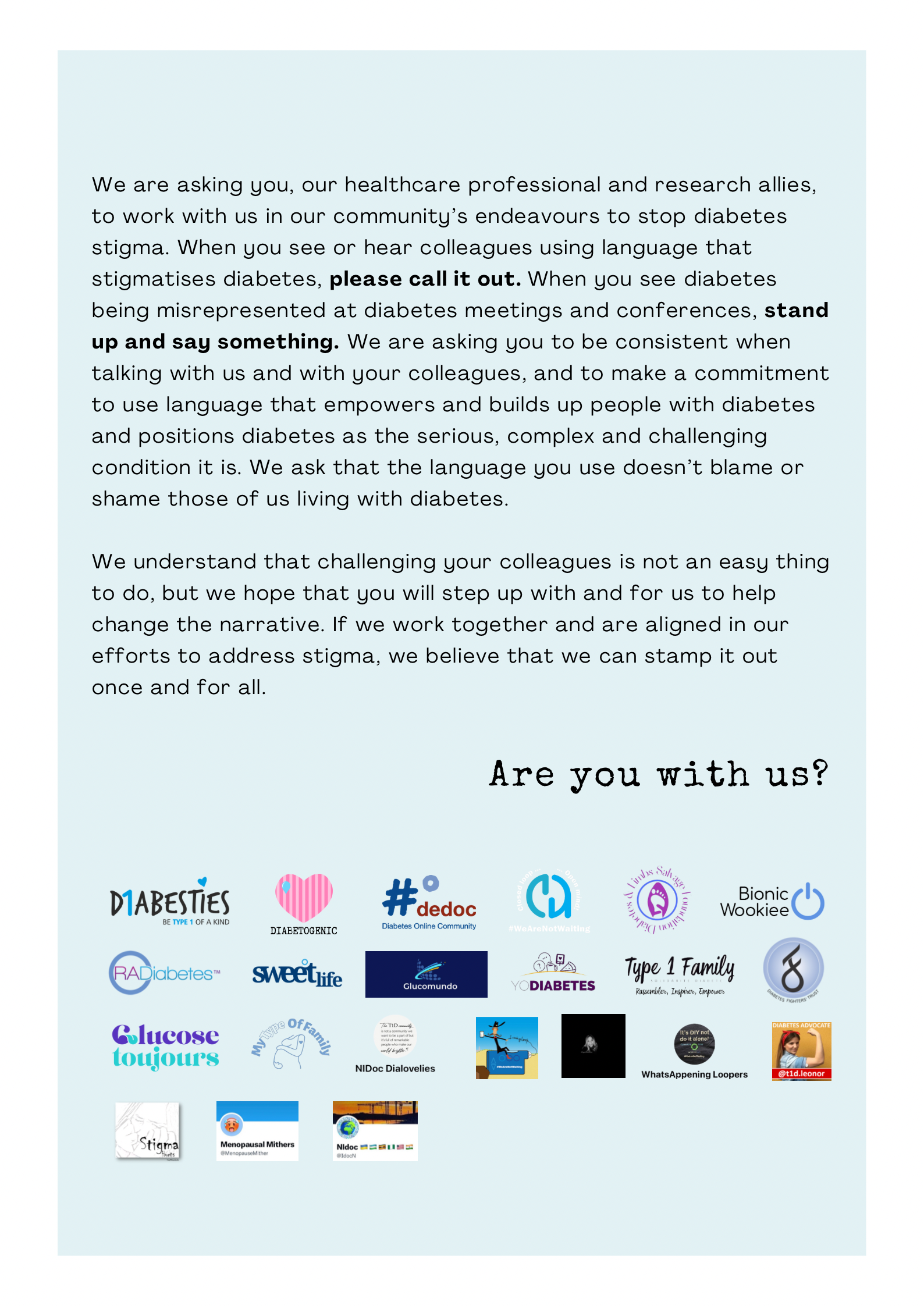
When we first asked advocates from the community if they would like to add their logo to the letter we were surprised by the quick response. Almost everyone we went to said yes. We hadn’t gone out too widely – we wanted to test the waters first. The first version of the open letter includes advocates and peer support groups from across the world. Amazing!
And after our very low-key, (i.e. a couple of tweets from unverified Twitter accounts, so who knows what the algorithm did with them!), we were once again inundated by people asking for us to add their logos. (We haven’t managed to add them yet, but absolutely will in coming weeks. Please give us time if you’ve shared your logo. We’ll get there. And I’ll update this post with the new final page when that happens.)
There is something magic about these sorts of very grassroots, very community, very inclusive initiatives. Not only are they great because they collaboratively offer a narrative from people with diabetes, highlighting an issue that is of great importance to many. They also show you just how powerful and united our community is while also pointing to individuals and groups who are keen to work together, support each other and power the importance of lived experience. And that’s pretty special!
Imagine a community where people come together to make things happen. You don’t have to look far, really. Just look at the diabetes community!
Here’s something new from some folks (Jazz Sethi, me and Partha Kar) who are desperately trying to reshape the way diabetes is spoken about, and how fortunate I feel to have been involved in this project!

The thinking behind these particular language resources is to truly centre the person with diabetes when thinking about communication about the condition. In this series, we’ve highlighted three groups where we know (because these are the discussions we see in the diabetes community) language can sometimes be stigmatising and judgemental. This isn’t a finger-pointing exercise. Rather it’s an opportunity to highlight how to make sure that the words, images, body language – all communication – doesn’t impact negatively on people with diabetes.
A massive thanks to Jazz and Partha. Working together, and with the community, to create and get these out there has been a joy. (As was sneaking into the ATTD Exhibition Hall before opening time so we could get a coffee and find a comfortable seat to work before the crowds made their way in!) And a super extra special nod to Jazz who pulled together the design and made our words look so bright pretty! And a super, super, super special thanks to Jazz for designing my new logo which is getting its first run on the back of these guides.
You can access these and share directly from the Language Matters Diabetes website. These don’t belong to anyone other than the diabetes community, so please reach out if you would like to provide any commentary or be involved in future efforts. There’s always more to do!







