
You are currently browsing the category archive for the ‘Health’ category.
‘Why do you even care what’s happening in America? It doesn’t affect you, does it?’
I’ve been astounded to hear a few people ask me this question after finding out that the kidlet and I participated in the Women’s March a few weeks ago, or after hearing me speak about the current situation in the US with the Trump Administration threatening to repeal the Affordable Care Act, and allowing insurers to discriminate against those with pre-existing health conditions.
I care a lot about what is happening in America at the moment. Without a doubt, my main focus is what is going on with healthcare and insurance, (however today, I am stunned, dismayed at Betsy DeVos’ confirmation as Education Secretary, but that is mostly because I cannot believe that someone who thinks guns have a place in schools ‘because of, you know, grizzlies’ is in charge of education).
Does it affect me directly? Well, probably not. But it is incredibly naïve of us to think that what happens in the US is completely irrelevant here in Australia. We know our politicians look to the US for policy direction. Our new Health Minister, in his maiden speech to Parliament, put forward the case for the adoption of a healthcare system more in-line with the US-system.
Of course what is going on in America affects us, but, actually, that’s not the point.
The real point is that I care because it’s about people. Not only that, it’s about the most vulnerable people. And like it or not, people with chronic health conditions are vulnerable. We are high-level users of healthcare, we face more discrimination and we cost more to the system. We can be hit where it hurts: easily and unfairly.
Of course, within this group there are some more vulnerable than others.
In the same way, I’ve had people ask me why I care so much about insulin access around the world, which seems like such a callous thing to even think, much less say out loud, when you remember that the life expectancy for a child diagnosed with type 1 diabetes in sub-Sahara Africa is 12 months. I actually still struggle to get my head around that really.
I care because I am a global citizen and I care because my social responsibility is to those less fortunate. I care because when my brothers and sisters around the world are struggling because they can’t access diabetes care, it hurts us all. I care because when I hear that instead of protecting the most vulnerable – as they should – governments are building walls (no pun intended) to make it more difficult, more frustrating and more tiring, the response should never be ‘oh well’, it should be ‘What.Can.I.Do?’ I care because diabetes is hard enough without having to fear being turned away from A&E or from other treatment. I care because no one should die because they can’t easily and affordably access a drug that has been around for 95 fucking years.
Of course I marched last month and you can bet that I will be doing it again. And you bet that I will be standing alongside my friends in the US as they fight one of the hardest battles they’ve ever faced just to be able to access healthcare, and my friends from around the world too as they fight access issues. And I will continue to make donations to charities helping those who cannot access insulin and be an Ambassador for Insulin For Life Global as they continue their excellent and necessary work.
But if you really think that it’s all too far away, so it won’t touch us, then perhaps you might like to do something to help people closer to home. As someone delicately reminded me last week, it is not only people in developing countries who struggle to access diabetes healthcare and drugs, and whose outcomes are far, far poorer than those of us living firmly inside a privilege bubble.
Get involved with or make a donation to an Australian-based charity if you would prefer to do something to help those closer to home.
We should all care because when others are disempowered, it means they are not able to get the best care or expect the best outcomes. And we do something because we can; and if we can, we should. That is what being socially responsible is all about.

Flowers die; children shouldn’t. Make a donation to Spare a Rose, Save a Child, and Life for a Child today. Click on the rose to take you straight to the donation page. Simples!
Just over three years ago, we sold our house and prepared to move into our new one. The real estate agent we had charged with getting us the best possible price for our much-loved first home walked through each room, nodding his head and taking notes. Once he’d finished the tour, we sat around the kitchen table and he started:
‘Your house is beautiful. You have it decorated very tastefully and it’s incredibly warm. The artwork is just lovely. The rooms are well proportioned and there is a sense of space. It’s really easy to fall in love with this home.’
We smiled at him. Clearly we had nailed the single-fronted Victorian style, not overdoing the period features, instead adding modern touches throughout while still giving a nod to the heritage of the area. Obviously, I should have been a stylist and was wondering how we could get on The Block.
Evidently, we’d be getting a call from the editor of Belle magazine for a feature. I imagined the photo spread: there was I standing in the kitchen whipping up a batch of cookies; Aaron sitting on the front veranda playing the guitar; close ups of the rosebushes in full bloom across the front of the house; the kidlet sprawled on the floor of her room, drawing; me lazily lounging on the couch reading with one of the dogs curled up at my feet….
And then the real estate agent brought me out of my reverie and back to reality.
‘Now, get rid of half of your stuff! There’s a storage place around the corner. Use it! Also, why is there Nutella everywhere?’
We stripped the house right back, brutally removing any details that made the house ours.
The music room was turned back into a bedroom, so by the time we had finished there was not a single musical instrument in the house, except for an oud we’d picked up in Morocco a couple of months earlier. The floor to ceiling CD shelves were dismantled and we held onto a handful of CDs, the rest going into boxes.
Books and bookshelves also were packed away leaving fewer than half our collection on show. Photos were packed away, reminders of our travels stored safely. Nutella jars were hidden away. By the time we finished no one would know that a musical and bookish family who had spent a lot of time traveling the globe and eating Nutella had been living there for 15 years.
The house felt a little like an empty shell, however it did provide potential buyers a sense of the space and feel of the house. In essence, we had taken the house back to basics allowing anyone walking through to imagine themselves making cookies in the kitchen or playing guitar on the veranda…
My diabetes management feels like it needs someone to walk through it and get rid of the excess. It seems there is so much going on – diabetes technology everywhere; bells, whistles and alarms; apps to record, remind and recommend; comparisons between different devices. I’ve been thinking about building some sort of automated system after being inspired following some meetings in New York. I look at numbers, turn them on their head as I analyse them and use the data to make minuscule changes, but don’t feel any clearer about what I am doing. There is a lot happening and it feels a little cluttered.
The thing is, I don’t really know what back to basics is when it comes to diabetes. Is it a complete and utter disconnection from technology? Returning to a basic and planned diet that is similar each and every day? Is it keeping records of everything in a simple notebook, looking for patterns?
Reminding myself of my word for the year – and overarching direction – perhaps I just need to pause and consider why it is that my diabetes management has found itself where it is – slightly chaotic with a lot going on!
It’s time to pause. It’s time to remember why 16 years ago I wanted to start using a pump and why 8 years ago I started using CGM. What were the motives behind those decisions and are they being achieved? Are they still relevant?
Lots of questions. Lots of thinking to do. With an overall aim of simplifying things, and that can’t be bad.

The front room of our old house ready for sale: from walls lined with books and comfortable places to read and work to bare basics.
When I spend time with friends in the US, they often take great delight in the words I use or the way I pronounce things. Apparently, there is much to amuse in the Australian-English language. In New York back in January, when speaking with friends about our voting practices, I explained the concept of the ‘sausage sizzle’. Our friends were looking at each other clearly wondering if we were serious, or completely making things up (i.e. fair dinkum or having a lend of them). It is my aim to have as many of my DOC friends as possible using ‘frocked up’ whenever they speak about dressing a little fancily!
And, somewhat oddly, it is in America that I am (apparently) most difficult to understand. I know I speak very, very fast and the frequent waving of hands can be distracting. I’ve learnt to adapt with some things (spelling my name when ordering coffee, I say ‘zee’ instead of ‘zed’) and try to adapt to the local lexicon (trash instead of rubbish / gas instead of petrol / Waldo instead of Wally* etc.) and try to slow down the speed with which I speak.
It’s February which means one thing and one thing only. It’s a month of red roses. That’s right, it’s time again for Spare a Rose, Save a Child.
I could tell you all about it again, but let me leave it to Manny and Graham who, once they get over the language barrier, do a great job of explaining the whole idea behind Spare a Rose…
I make a monthly donation to Life for a Child via this campaign. Each month AUD$6 comes out of my account and directly deposited into theirs. Six bucks. Basically, that’s a coffee and a half. So, the equation is this:

That’s right: for what it costs me to purchase 1.5 coffees, a child in a developing country survives for another month.
Every February, I urge people to consider donating to Spare a Rose Save a Child – either as a one off on Valentine’s day, or to set up making a monthly donation. And this year, with all that is going on in a very messed-up world, here is one small way to feel that you are helping out someone who really, truly needs it.
‘Inshulin’ or ‘inssulin’. It doesn’t matter how you say it. Just help a kid in need get some!
![]()
*IT’S FREAKING WALLY, NOT WALDO!
Sometimes, I’m a lousy person with diabetes (PWD). I am thoughtless and unclear about what I need, have ridiculous expectations of others – and myself, and am lazy. But I’m not always like that. And I think I know what I need to do to be better.
Being a better PWD is about being true to myself. It is also about reflecting on exactly what I need and I hope to get it.
- I need to remember that diabetes is not going away
- I need to remember that the here and now is just as important as the future
- I need to remember that I don’t have to like diabetes, but I have to do diabetes
- I need to remember that the diabetes support teams around me really only have my best interest at heart, and to go easy on them when I am feeling crap
- I need to empty my bag of used glucose strips more frequently to stop the strip glitter effect that follows me wherever I go
- I need to remember that it is not anyone else’s job to understand what living with my brand of diabetes is all about
- I need to remember that the frustrating and tiresome nature of diabetes is part of the deal
- I need to be better at changing my pump line regularly
- I need my diabetes tasks to be more meaningful – quit the diabetes ennui and make smarter decisions
- And I need to own those decisions
- I need to see my endocrinologist
- I need to decide what I want to do with my current diabetes technology. There is nothing new coming onto the market that I want, but what about a DIY project to try something new? #OpenAPS anyone…?
- Or, I need to work out how to convince the people at TSlim to launch their pump here in Australia
- I need to check and adjust my basal rates
- I need to do more reading about LCHF and decide if I want to take a more committed approach or continue with the somewhat half-arsed, but manageable and satisfactory way I’m doing it now
- I need to remind myself that my tribe is always there and ask for help when I need it.
- I need to make these!
And being a better PWD is knowing what I need from my HCPs and working out how to be clear about it, rather than expecting them to just know. (I forget that Legilimency is not actually something taught at medical school. #HarryPotterDigression)
So, if I was to sit down with my HCPs (or if they were to read my blog), this is what I would say:
- I need you to listen
- I need you to tell me what you need from me as well. Even though this is my diabetes and I am setting the agenda, I do understand that you have some outcomes that you would like to see as well. Talk to me about how they may be relevant to what I am needing and how we can work together to achieve what we both need.
- I need you to be open to new ideas and suggestions. My care is driven by me because, quite simply, I know my diabetes best. I was the one who instigated pump therapy, CGM, changes to my diet and all the other things I do to help live with diabetes
- I need you to understand that you are but one piece of the puzzle that makes up my diabetes. It is certainly an important piece and the puzzle cannot be completed without you, but there are other pieces that are also important
- I need you to remember that diabetes is not who I am, even though it is the reason you and I have been brought together
- And to that – I need you to understand that I really wish we hadn’t been brought together because I hate living with diabetes
- I need you to remember that I set the rules to this diabetes game. And also, that there are no rules to this diabetes game
- I need you to understand that I feel very fortunate to have you involved in my care. I chose you because you are outstanding at what you, sparked an interest and are able to provide me what I need
- I need you to know that I really want to please you. I know that is not my job – and I know that you don’t expect it – but I genuinely don’t want to disappoint you and I am sorry when I do
- I want you to know that I respect and value your expertise and professionalism
- I need you to know that I hope you respect and value mine too.
And being a better PWD is being clear to my loved ones (who have the unfortunate and unpleasant experience of seeing me all the time – at my diabetes best and my diabetes worst) and helping them understand that:
- I need you to love me
- I need you to nod your heads when I say that diabetes sucks
- I need you to know I don’t need solutions when things are crap. But a back rub, an episode of Gilmore Girls or a trip to Brunetti will definitely make me feel better, even if they don’t actually fix the crapness
- Kid – I need you to stop borrowing my striped clothes. And make me a cup of tea every morning and keep an endless supply of your awesome chocolate brownies available in the kitchen
- Aaron – I like sparkly things and books. And somewhere, there is evidence proving that both these things have a positive impact on my diabetes. In lieu of such evidence, trust and indulge me!
- I need you to know I am sorry I have brought diabetes into our lives
- I need you to know how grateful I am to have you, even when I am grumpy and pissed because I am low, or grumpy and pissed because I am high, or grumpy and pissed because I am me.
Today is my first day back at work. I spent the weekend preparing for the day by sitting in the sunshine, drinking coffee, deadheading rose bushes and switching back on the part of my brain that thinks about work. And remembering how to walk in high heels.
The new year looms ahead. It’s huge. There are things to finish from last year and lots of new projects waiting to begin. And starting fresh with a clean slate and thinking strategically about how to get things done is important.
I don’t really do New Year’s resolutions. I’m lousy at committing to anything remotely healthy, so there is no point in trying to promise to do something that I’ll do for two days, then stop doing and then feel bad at myself for not doing it anymore.
I don’t really want to use the New Year to focus on diabetes by concentrating on particular tasks or specific measures. Outcomes seem to be organic and setting goals, while a noble gesture, often lead to disappointment. Feeling like a failure is not how I want to begin the year!
But I do like the idea of embracing the New Year and cracking open its spine, revealing clean pages and new beginnings.
Australian writer and publisher, Mia Freeman, shared that last year, she came up with a word that would help draw her attention to her plans for the year ahead, and has done the same for this year.
I like this idea – the thought of having some sort of directive that would be an overarching theme for decision making and planning, and would, hopefully, mean that I ended the year feeling a success rather than just a shattered and weary mess.
Because I have found myself pretty exhausted at the end of the last few years. I know everyone is – we get to a point where we are just done and need a break. I felt as though I was burnt out with life when I went on leave, and the much needed holiday was about getting back to a place where I felt I could tackle what lay ahead.
With this in mind, I wanted my word to help me avoid that burn out, so that come the end of the year, the exhaustion I felt was not so overwhelming.
So, I spent some of the time we were in New York auditioning words, trying them out, rolling them around on my tongue and hearing them in my mind, thinking what they could mean for me throughout 2017. As I walked around the snowy streets, I projected how I wanted to feel at the end of this year and what I would need to get there.
The word I have settled on is pause.
As soon as I said it, I knew it was the right word. I wrote it down, over and over, thinking about how it could shape and help plan my year. I wrote it on scraps of paper and shoved them into my purse and handbag to remind me. And the minute I walked into my office this morning, I wrote it on a post-it and stuck it to my wall.
Pause doesn’t mean that I will be stopping anything I’m doing. It doesn’t even necessarily mean I’ll be cutting back. But it does mean that before committing to anything new, continuing with something old or exploring different ways of doing things, I will pause and think about why and how I am doing it.
The tendency to simply say yes to everything serves no one – the results are me not doing things as well as I might like or feeling disappointed with the end result.
I also am seeing how I can adapt the word to suit my diabetes management. I think that too often, I am on autopilot, not really thinking about what it is that I am doing. To pause means giving meaning to actions, attention to decision making and focus to the way I choose to manage my diabetes. Jumping on a bandwagon because it has been written up in a few different diabetes magazines – without pausing to consider if it is right for me – really makes no sense. I am very guilty of wanting, needing the latest toy without necessarily stopping to think if it will serve any purpose.
There is already a lot in the calendar for 2017 – all the way through to its end with the IDF’s World Diabetes Congress rounding out the busy year in December. I’m the Deputy Stream Lead for the Living with Diabetes Stream, so there is no chance of slowing down as the year winds down.
So, with all this in mind, my word for the year is going to help shape how I approach things. I’ll have to see how it goes and I expect I’ll need to pull myself back at times, reminding myself to stop, think and, perhaps, wait. And then, as I pause, take the time to let things sink in, catch up and take shape.

Last week, my Timehop app reminded me of this snapshot in time.

This photo was taken at the 2013 International Diabetes Federation’s World Diabetes Congress in Melbourne, and that look on my face is of pure anger. I was listening to a speaker – a doctor – referring to ‘non-compliant diabetics’ as he was telling of the ‘poor outcomes’ of ‘patients’ in his practise.
The old language chestnut came up again on the second day of the #MayoInOZ conference during the innovation showcase was held. In this session, nine speakers were each given five minutes to present how they are using social and digital tools to improve healthcare. (This is where Kim spoke about #OzDOC and how healthcare professionals use the hourly tweetchat as an opportunity to engage and learn from people with diabetes.)
The final speaker in the innovation sessions was a late addition and it was great to see diabetes again being represented. I know I am biased, but I do always get excited when I see diabetes on the program!
Andy Benson from Coffs Endocrine and Diabetes Centre presented on the project she has been working on: telling the story of diabetes in a series of documentaries to be screened on the BBC.
So, first things first. I love this idea. I am a huge fan of having diabetes out in the ‘public’ space, pulling it out from diabetes groups and diabetes-specific forums, because in most of these cases, we’re preaching to the converted. It’s one of the reasons I love writing for Mamamia Women’s Network where I know that most of the readers probably don’t already have a connection to diabetes.
If these documentaries are screened on the BBC, imagine the audience! It is so refreshing to see people thinking outside the box and looking for ways to present to a new audience – and to tell stories, real stories of real people who actually live each day with diabetes.
Andy showed two short video clips from the still-in-development documentaries. As healthcare professionals on screen spoke about diabetes, I automatically prickled, my language and stigma sensors being alerted straight away.
I wasn’t the only one. In a room with two other diabetes advocates – Kim, Melinda Seed (Once Diabetes), as well as several very vocal health advocates and activists, there was a sense of discomfort at what we were seeing.
I inhaled – maybe ‘gasped’ is a better word – when one of the HCPs used the words ‘diabetes plague’ in his introductory words. There was an undeniable sense of blaming the person with diabetes in the words being used and the sentiments being expressed.
The Twitter conversation from both people in the room and those following along was honest and candid. And, quite frankly, it was uncomfortable too. Andy had disclosed that she has type 1 diabetes, and I didn’t want to be actively criticising the work of a fellow PWD.
However, I could not keep quiet either. When Andy came over to chat after her talk, we had a very open discussion. I was probably quite blunt in my comments.
It is not okay to use language that is stigmatising. The format of the information being presented (i.e. unscripted interviews) doesn’t preclude anyone from being courteous and respectful, and I don’t believe that PWD were being treated either courteously or respectfully in the way about which we were being spoken.
I understand that there is a desire for authenticity and genuineness when interviewing documentary ‘talent’, however it is possible to be clear from the outset that language needs to be respectful at all times. Not sure where to begin with this? How about the Diabetes Australia Language Position Statement which actually provides suggestions for inclusive, non-stigmatising language?
I think it is really important to acknowledge that the road to satisfaction in the way we use language that is inclusive and non-stigmatising is a very, very long one. Also, I genuinely don’t believe that there was any malice intended on the part of the film makers or the interviewees.
We also need to acknowledge that the language used in what has been (and many would argue continues to be) a patriarchal health system is entrenched in the thinking of many – it was part of their training and is a habit that will take time to break. But by acknowledging it, we are not saying it is okay.
As I said, I love the idea that diabetes is a topic for a documentary that is being made for a non-diabetes-specific audience. However, if those people walk away thinking that my healthcare condition is a burden to society (and therefore I am too!) or that they believe it is okay to continue to use words that stigmatise, then there is the potential for this work to do more harm than good.
And finally, a call to not only the coordinators and owners of this work, but to all who are developing any sort of health information using any sort of platform: talk to people with the condition. Lots of them. It is not okay to have one token consumer representative; there should be many – as many as (if not more than) any other expert being consulted.
Today, I gave a talk to healthcare professionals at a hospital in outer Melbourne. I was invited months ago after the organisers heard me speak at another event, and they wanted me to speak about living with diabetes.
As I said in the introduction to my talk, I am dead boring. Plus, I am only one voice. So, to create some balance and some interest, I reached out through Facebook and asked this:

As usual, the online community didn’t disappoint. I had over forty responses and weaved them into my presentation, adding real impact to what I was saying, reinforcing my comments with the comments of others walking a similar path of life with diabetes.
I started by asking the audience a question…
And then I said that I would be talking about life with diabetes. Except, I reminded the audience that life with diabetes was very different depending on where in the world you were diagnosed and that my story is about my ‘first world diabetes’ and I checked my privilege almost as a disclaimer.
I used that point in my talk as an opportunity to speak about those who cannot access or afford insulin and how this is simply, not okay. I could sense the surprise in the room as I said that people are dying because of lack of access.
Then I spoke about what diabetes is to me and here is what I said:
It’s boring and tedious and frustrating.

It’s made me an expert. And that we need our HCPs to acknowledge the hours and hours and effort we put into managing our own brand of diabetes and the expertise we develop from living so closely with this condition.

It’s about humour – because laughing is a tool I use to get through this and that’s okay.
 It’s about words, because language matters and sticks with us forever.
It’s about words, because language matters and sticks with us forever.
It’s about stigma. I asked if they could think of another condition that was so stigmatised and surrounded by blame – and that while we experience it with type 1 diabetes, I said that I believed my brothers and sisters with type 2 diabetes have it so much worse.

It’s invisible – despite the bright blue patch surrounding my Dexcom, most of the time it is hidden away and not on show for all to see.

It’s about people and community and the DOC and the people that are like the air I breathe – without whom I would not be managing at all.

It’s about my family. And then I explained, fighting back tears, that this is the hardest part of life with diabetes for me. I’ve written about it a lot, spoken about it often. But thinking about how diabetes impacts on Aaron and the kidlet breaks – absolutely shatters – my heart into pieces. The worry I cause my parents makes me feel guilty and resentful. And every day I regret the time I told my sister that my life expectancy had been cut thanks to my type 1 diagnosis because I will never forget the look in her eyes indicating the pain I had just caused her.
I answered a couple of questions and then my talk was done. I thanked the audience for listening, stepped down from the stage, took a deep breath. Someone came up to me as I was gathering my bags and said that she learnt more about real life with diabetes in that talk than in all her years nursing.
This is the power of story telling. The comments I read out and shared have so much power in them. We need to keep telling our stories, turning the way we talk about diabetes on its head. It’s not about the numbers, the tools or anything else. It is about people.
Thank you so much to everyone who shared their comments with me on my Facebook post yesterday and today.
November is a big month in diabetes. For those of us living in Australia, the main event is World Diabetes Day on 14 November, but I’m certainly happy to be swept up in the USA’s Diabetes Awareness Month.
For the next four weeks, there will be a lot of diabetes awareness about and it’s a great opportunity to speak about real life with diabetes, dispel some myths and set the record straight when someone tells you to increase your cinnamon consumption to cure your diabetes.
Get your blue on…
Blue is the colour of diabetes and, this month, it’s my colour of choice! (Including this potentially misguided nail colour. My manicurist actually said ‘Are you sure?’ when I picked it our yesterday.)

I’m stuck with these nails for a couple of weeks now, but plan to accessorise with a lot more blue (including the blue mascara and eye liner I bring out just for November!)
And a throwback to 2011 (seriously!) when Cherise got a few DOC folk together to make this video. Wear blue!
Diabetes is not about numbers. Until it is.
JDRF has this nifty calculator on their website that (somewhat scarily) adds up the numbers to show just how many diabetes tasks we’ve undertaken in our diabetes lives. Here’s mine (as of yesterday).
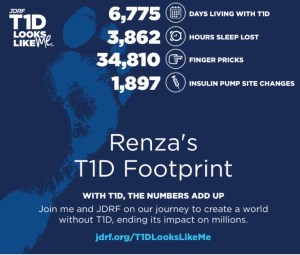
I am the first to say that diabetes is not all about numbers, but I do love this because it shows the magnitude of this condition and its relentlessness. You can get yours here.
(And JDRF UK has their own here.)
What is diabetes awareness month all about anyway?
In fact, what are ALL awareness months about? This beautiful and throughtful post from Jessica Apple from A Sweet Life (online magazine) is definitely worth a read.
And this take from a Diabetes Dad…
And Tom Karla (AKA Diabetes Dad) has this to say about just who this whole month is for. (Spoiler: it’s not for those of us already living with diabetes!) As I said on Twitter yesterday – I spend a week every July (during National Diabetes Week in Australia) trying to explain this. Will be forwarding Tom’s post far and wide from now on!
7 day online peer support…
Did you know that there is a free online Peer Diabetes Mentoring Summit running right now (until 7 November). Diabetes Dominator, Daniele Hargenrader, has coordinated this fab event and you can claim your free ticket here. So many terrific sessions with great speakers to follow!
Photo challenge
There’s a fun photo challenge for the month from Project Blue November. Using the prompts they’ve provided, post a photo each day to your SoMe feeds to share your life with diabetes, tagging the pic with #ProjectBlueNovember. Here are the prompts:

What I’d tell myself at diagnosis..
Lovely piece from the team at Diabetes Forecast where some PWD share the wisdom they would give their newly diagnosed self. Read it here.
And here’s the letter I wrote to my newly diagnosed self a few years ago. It still holds pretty true!
Circled
The International Diabetes Federation’s WDD selfie app (download for free at the app store) allows you to add a blue circle – the international symbol for diabetes – to any photo you’d like.

Big Blue Test
And of course, November means that it is time once again for the Big Blue Test, brought to us by Diabetes Hands Foundation. Over 125,000 BBTs have been logged since the program started in 2010. Easy peasy lemon squeezy instructions are:
 Get logging for good karma. There’s even an app you can use to make it super easy. (And yes – I’ll be logging before and after I take the pups for a walk!)
Get logging for good karma. There’s even an app you can use to make it super easy. (And yes – I’ll be logging before and after I take the pups for a walk!)
Keep in perspective.
It’s really easy to get overwhelmed by everything diabetes that’s going on this month. If your SoMe feeds are anything like mine, they will be overtaken by diabetes and there really does seem to be no escape.
Which is why it’s important to remember that we are about so much more than diabetes and find time in the month to do things that remind us of that. We have a couple of birthdays to plan and an upcoming trip to New York to think about – all things that will hopefully keep the whole month in perspective. Plus there is always baking…maybe some cookies…

There are few topics guaranteed to polarise and cause debate like food and what we are eating. Our choice of what we put in our mouths will always generate comments, whether invited (and welcome) or not. And add diabetes to the mix and it gets even worse. From ‘Should you be eating that’ to ‘Here, this is low fat, low sugar, high cardboard content’, we get it all!
I wrote a couple of months ago about how I had unintentionally started eating low(er) carb, and shared my thoughts on how that was going. I’ve also made a few comments on my social media feeds about some things I’d been trying. Interestingly, and as a result, I’ve been contacted by complete and utter strangers wanting to give me their thoughts. This in itself is not that odd; I frequently have messages from people I don’t know about my blog.
What is different here though, is the tone that is often used. And it is not always particularly positive. I’ve been accused from jumping on a bandwagon, loving Pete Evans (that one made me laugh for about four days straight!), letting down the team and being untrue to my Italian heritage. I ignored them all.
I’m a few months in now and couldn’t really care less what people think. I am trying something to try to improve my own diabetes management, not anyone else’s and I’m certainly not even considering suggesting that this is something others might like to try. The My Diabetes My Rules thing possibly applies here more than anywhere else.
The experiment has been continuing, and what I have been most interested in is not only the results regarding my diabetes, but I also really wanted to know if this change in my hearting habits is truly sustainable.
So, a couple of things I want to say to begin with. I have not adopted low carb high fat as a way of life for me. I am ad hoc at best. There are some things that I refuse to change and I have no problem with that at all. This lack of real commitment has drawn criticism from a few people who also thought they would message me to say that if I wasn’t doing low carb high fat properly that I was a fraud and should just shut up. I ignored them too. (That’s the beauty of writing your own blog – you don’t have to listen to people!)
The sustainability issue seems to have worked for me by muddling through the best way I can, making sure that I never say no to something I really want to eat. And perhaps, that was the ‘Aha’ moment for me. There is no right way to do this – except the way that works for me.
For example: I love bread. Love it. Adore it. Love. Love. Love. But there is bread and there is bread. When I eat bread, I only eat bloody good bread. Like a beautiful, chewy seeded sourdough from Baker D Chirico, bought fresh from the bakery and slathered with lashings of real butter – preferably French; always salted.
I’ve decided that there is no point eating a piece of highly processed square bread out of a packet that is not freshly baked and is full of preservatives. So I don’t eat it.
My breakfast most mornings continues to be a milky coffee. I’m nor cutting out the milk or the sugar, even though I know both do raise my BGLs. But I manage that as well as I can, hoping for no spike within half an hour of consumption. I am not good in the mornings without that first (and often second) coffee. And for the love of all that is good and those around me, it’s best that I just have my latte and get on with it.
Overcoming the mindset of needing to eat carbs has been a huge challenge for me. HUGE. It is possibly a combination of 18 years of conditioning about the need to include carbs in my meals and also generally loving carb-based foods.
But there are options. And as I work out what they are, meals are becoming easier.
Where I think I have been getting the biggest bang for my buck is adapting evening meals to be lower carb. This has resulted in far nicer glucose levels in the evenings, overnight and, subsequently, in the mornings. For me, it’s complete
ly and utterly undeniable that not loading with carbs equals diabetes that is far easier and nicer to try and manage.
 So, here are just a few things that I’ve prepared recently to give you an idea of what I have been doing to lower my carb intake. Often, my evening meal is zero carbs which is generally what I have been aiming for as this offers the best post-prandial results.
So, here are just a few things that I’ve prepared recently to give you an idea of what I have been doing to lower my carb intake. Often, my evening meal is zero carbs which is generally what I have been aiming for as this offers the best post-prandial results.
For the colder months, the oven has been working overtime, cooking braises and stews for hours at a time. Or one pan wonders like this that combine chicken, chorizo, lemon, garlic and spinach.
 I always love to serve them with mashed potatoes, but have tried mashed cauliflower instead. I refused to even entertain the thought of mashed cauli until recently, when I decided to try it and have found it it delicious. (I either steam or bake it first
I always love to serve them with mashed potatoes, but have tried mashed cauliflower instead. I refused to even entertain the thought of mashed cauli until recently, when I decided to try it and have found it it delicious. (I either steam or bake it first
and then pulverise it with a stick blender with salted butter (lots) and milk. Or cream if I have some in the fridge.) I can eat a huge bowl of it and my glucose levels do not shift a smidge. (I know this to be true because I have, on several occasions, eaten nothing but a huge bowl of it for dinner and then watched the flat line of my CGM.)
 Actually, cauliflower has become a favourite food. And it’s insanely cheap at the moment. Roasted cauli has become another staple. My favourite way is to cut out the core and bake it whole, drizzled with olive oil, oregano and fresh garlic. But cauliflower is one of those veggies that simply soaks up flavours, so anything goes. I’ve also tried lemon, garlic and rosemary which works a treat. (I’ve worked out that steaming the cauli in the microwave for about 5 minutes first cuts the cooking time down, so usually I do that before shoving it in the oven.)
Actually, cauliflower has become a favourite food. And it’s insanely cheap at the moment. Roasted cauli has become another staple. My favourite way is to cut out the core and bake it whole, drizzled with olive oil, oregano and fresh garlic. But cauliflower is one of those veggies that simply soaks up flavours, so anything goes. I’ve also tried lemon, garlic and rosemary which works a treat. (I’ve worked out that steaming the cauli in the microwave for about 5 minutes first cuts the cooking time down, so usually I do that before shoving it in the oven.)
I made low carb gnocchi one night with hazelnut meal instead of flour and tossed them through a burnt butter and sage sauce, with tiny pieces of crispy fried pancetta sprinkled on top.

Do I feel as though I missing out on anything? Not really. Because if I want something, I still eat it. No foods are considered taboo, there are still no ‘good’ or bad’ foods. I still bake heaps and sample everything I make. (Case in point – these amazing squidgy choc-chip cookies I made the other day that are delicious!)

But what I do know is that minimising riding the blood glucose rollercoaster makes me feel better and this is by far the easiest way I have ever known to do that. It’s not perfect and there are still un-explained highs and lows. There is no name for this way of eating. But it is working for me, so for now, I’ll stick to it.
There is a dance I do with diabetes each and every day. I praise, celebrate and highlight the good; I avoid, shut out and ignore the bad. The things that scare me are pushed away – as deep as they can go. When they threaten to rise to the surface, I do the equivalent of sticking my fingers in my ears and start chanting ‘la, la, la’ so they recede to where they belong. Out of sight. Out of mind.
I’ve done this for as long as I’ve had diabetes. From day one, I pushed away the ugly and scary images of diabetes complications. I conveniently ignored the warnings and threats. Obviously. Because no one wants to be scared or warned or threatened the day they find out they have a life-long chronic health condition. Or ever.
I am scared. Diabetes scares me a lot. It always has, but for some reason, it is more at the moment. I don’t know why. Nothing has changed. There has not been a frightening experience or a noticeable change in anything. But as days and weeks and months and years as a person with diabetes gets crossed off some imaginary calendar, I am suddenly feeling that it is a countdown to where the really difficult things start.
I worry about what each passing hour is doing to my body and to my mind. If I’m being particularly forgetful, I wonder if it is because my head is so full of diabetes considerations that there is no room for a synonym for fear (dread, anxiety, terror, dismay alarm….) or recalling what day my kid has library each week.
But thinking about it more, I think the fear comes from the lies we are sold about our diabetes. I was promised the day I was diagnosed by a lovely, but most likely completely out of touch doctor, that diabetes is a matter of maths and that if you do the equations properly, it can be easily controlled.
Diabetes can’t be controlled, and with each moment of failure – and there are many and they are constant – I have feared the consequences. And I fear diabetes. With each missed calculation or out-of-range number or confusion about how the hell this thing really works, I see failure. And fear.
Diabetes is not a matter of maths, and the idea that I can control it results in a constant state of high alert as I pretend to be a body part that, when working, is pretty damn perfect. I am not perfect. In any way. And neither is the way I manage my diabetes. It’s messed up. And I’m messed up about it.
And now, as always, there are the fears. And they seem bigger and bolder all the time. I fear diabetes-related complications – long- and short-term. I fear losing the ability to take care of myself and care for others. I fear diabetes becoming so intrusive that I am unable to do anything else. And I fear diabetes becoming the first, last and only thing others think about when they see me. Perhaps most of all, I fear diabetes becoming the first, last and only thing I think about when I see me…
I wonder just how differently I would feel about diabetes – the known and unknown – if I was told at diagnosis that I would get this wrong more times than I got it right. And that was perfectly okay, understandable and acceptable. I wonder how much less significant the feelings of failure would be. And how much more in check my fears would be.

9 March, 1998. 37 days before diagnosis.






