
You are currently browsing the category archive for the ‘Diabetes’ category.
Today I hate diabetes.
I am completely and utterly sick of the World Diabetes Day messages that are scrolling through my screen. I am over looking at posters and diabetes empowerment messages and I cannot be bothered being involved in the activities that are all around me. I don’t want to talk about it – which is actually really unfortunate as I am giving a Grand Rounds talk at the Austin Hospital today about life with type 1 diabetes.
This morning I am hypo-fucked after dealing with a low that would not quit. This is the sort of low that mocks and teases and is just plain cruel. And when it finally passes, glimpses and flashbacks plague my mind for the coming days, reminding me how vulnerable and scared I feel.
I needed help to manage it – and I absolutely hate making my lows someone else’s problem. Eventually, after a jar of jelly snakes, raisin toast and two glasses of milk, my BGL started to resemble something respectful and I was able to change out of my sweat-soaked PJs. Despite being in something dry and under a warm doona, I was chilled to the bone and shivered for an hour before finally falling asleep.
Today, diabetes made me break a promise I’d made to my daughter – a walk to school with the puppy. But what made me feel even worse was the way she nodded her head in acceptance – and understanding – of why I was breaking the promise. I hate that diabetes is part of my daughter’s life because of me. I hate that she understands diabetes. I hate that she ‘gets it’ when I tell her that I can’t do something because of my stupid blood sugar.
Today I hate diabetes.
Today, I feel defeated. Today, I desperately want to not be living with this condition.
Yesterday, I took part in Diabetes Queensland’s WDD social media campaign that asks people to share what ‘type 1 diabetes for me is….’ (#T1D4MeIs). Here is what I came up with:
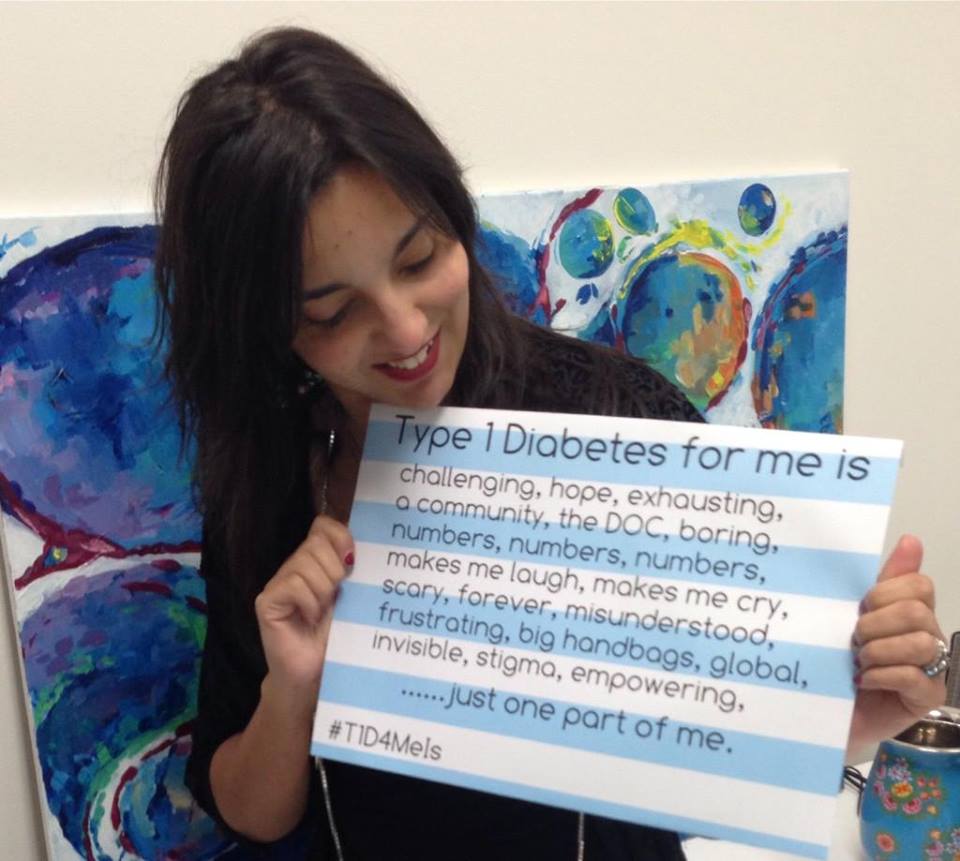
Today, my poster would look a lot different. It would have just one word.

Today I hate diabetes. I don’t feel empowered. I don’t feel ‘in control’. I just feel sad. And scared.
‘Excuse me,’ I turned to my left to the man sitting next to me on the 7am flight to Sydney and smiled. ‘Yes?’ People were still boarding around us and I was killing time checking Twitter before being told to switch my iPad to flight mode.
‘Oh. I couldn’t help notice…’ He was looking at my hand which held my pump. I finished pressing a button to silence an alarm and hastily shoved the device back down my top, all the time looking at him. He paused and I waited for the question about what it was I had in my hand, or, perhaps, recognition. He looked flustered.
‘Um. I couldn’t help notice what you were looking up on Twitter. Did you go last night?’
He motioned to the stream I was scrolling through – all images and tweets of the previous night’s Rolling Stones concert at Rod Laver Arena. My smile got wider.
‘Yes!’ I said. ‘Were you there?’
He shook his head. ‘I have tickets for Saturday night at Hanging Rock, but I’m selling them to someone. It’s my best mate’s 40th birthday, so…’ He let his voice trail off. ‘So, how was it?’
I started with ‘AMAZING!’ and went through every superlative I could think of, telling him how incredible the gig was; how amazingly the band played; how energetically Mick Jagger danced.
‘Damn,’ he said. ‘I was hoping you’d tell me that they were past it and it was terrible.’
‘I can lie if you want me to. But really – it was one of the best gigs I’ve ever seen!’ I then thought of something. ‘Did you say you have someone to buy your tickets for Saturday?’
‘I think so. I’ll find out later this morning.’
I reached into my bag and handed him my card. ‘Sorry for being so forward, but if, for some reason, your friend doesn’t want them, please call me. I’ll buy them from you.’
‘Sure,’ he said, tucking my card into his shirt pocket.
I went back to scrolling through the tweets and glanced back. He was still looking at me.
‘Um…’ he started. ‘Well…have a good flight.’
‘Thanks! I’m about to fall asleep. Clearly I don’t have the energy of the Stones – I’m exhausted after the late night.’ I smiled at him again, turned off my iPad and promptly fell asleep before the plane took off, waking just in time to hear the seatbelt sign being turned off. We were in Sydney.
It was the usual craziness as passengers jumped up, grabbed their bags and jostled to get off the plane. As my seat-mate reached up to the overhead locker to pull down his briefcase, I saw it. There, sticking out of his trouser pocket, was a pump line.
He turned in time to see me noticing it. He stopped for a moment before saying, ‘Well…See you later. I’ll be in touch if the tickets don’t sell.’
‘Cool. Good luck. Enjoy your friend’s 40th – it better be worth it!’ And then, before he walked down the passageway, I said, ‘You’ve got my card.’

The highlight at the Stones’ gig was their first encore – You Can’t Always Get What You Want – because the Consort of Melbourne, conducted by one of my mates, provided the choral introduction. And here it is!
For the last three weeks, ever since returning from overseas, there has been a constantly replenished bunch of roses on the kitchen table. They range from a blush colour through to a beautiful light orange and have a fragrance that hits you as you walk into the room. After a few days in the house, they have opened, blooming magnificently, and then, over the next few days, drop their petals prettily and gently at the base of the vase.
Along the fence at the front of the house is a row of stunning rose bushes. To give you an idea of my gardening prowess, I can kill a cactus. (Correction – I have killed a cactus.) But roses seem to be indestructible. In our old house, we had three beautiful Margaret Merril roses along the front fence with a gorgeous perfume that would stop passers-by. One – the middle one – was a wedding gift from one of my bridesmaids (showing extreme optimism on her part that I wouldn’t kill it within a week) and the other two were bought to plant alongside.
I love roses – especially old fashioned ones. I love the fact they are enduring – that once they have flowered, I can butcher them back to nothing and within a short time, they will be rewarding me again with their beautiful blooms. I love that it doesn’t matter how much I neglect them, they still grow and thrive. I love that while roses may not be the trendy flower of the moment, they are always so elegant and beautiful.
Recently, on walks with the new puppy, I’ve been paying much attention to the beautiful bushes on our street. There is every colour imaginable, some with a gorgeous scent, others purely decorative. There are arbours welcoming people into gardens and climbers decorating the period homes in the area we live. One house has the most stunning, overrun bush – almost a tree, actually – that I stop at each time we walk by. It looks like it has been there for decades and when it’s time, I intend to knock on the door and ask the owners if I can take a cutting.
Roses have an inextricable – and ridiculous – link to diabetes for me. Whenever I am pruning them, I inevitably stab a finger on one of their angry thorns and, whilst cursing the pain, use this as a perfect excuse to check my BGL. There’s never any point wasting blood.
When our old Margaret Merrils – which were standards rather than bushes – were being trained to grow and stand tall, they were always tied to their stakes with spent pump lines.
And of course, the Spare a Rose, Save a Child campaign beautifully juxtaposes diabetes and roses.
I’m not sure if it is the fairy-tale-like quality of the pricked finger and drops of blood, or the fact that it doesn’t matter what I seem to do – whether a tend to them diligently or ignore them completely – but the roses are still there. I’m not sure if it is the beauty that thrives despite the nasty thorns that lie underneath. But there is something about a rose that makes me think forever. Just how I feel about diabetes….

In full bloom on the kitchen window sill.
I am all for going with the flow. I’m happy to try out something new, and one of my least favourite things is when I hear people say ‘…but we’ve always done it this way‘. I like visiting new places and being challenged by new adventures.
But equally, I love a bit of routine in my day – especially on weekday mornings and at bedtime.
We have a morning routine that ensures everyone is out of the house dressed, organised, fed and watered and where they need to be. Our daughter heads to school with her lunch packed, notes signed, homework done and packed away, and her hat ready for playtime.
We do this every single Monday to Friday during the school term. Weekends and holidays are all over the place because we rarely need to be somewhere in a clean uniform by 9am.
Bedtime is the same. This is also all about routine. PJs on, teeth cleaned, hair brushed and plaited, and lots and lots of cuddles with last chats about the day. Then into bed for a spot of reading. This is followed by the added-extras. The kidlet tries to bargain another five minutes of reading time, sneaks her light back on when she’s told to sleep, and gets up for a drink of water. She says good night to her puppy about fifteen times and tries to find the cat, coaxing Cherry to sleep on her bed.
It’s the bedtime routine that we do pretty much every night. It works – even with the bargaining and distracting.
Last night’s cuddles were given over the phone because I am away for work overnight in Sydney. It’s the first time in two years that I’ve not done the bedtime routine (apart from the overseas travel and her occasional sleepover with friends) and when I hung up from her, I realised I’d forgotten to ask if there was any last thing she wanted to say to me. I told her I loved her, but I didn’t say ‘I love you mostest.‘ At which point we would both say ‘Not a word!‘ I’m out of practice with the one-night-away-from-each-other routine.
Actually, as it turns out, I’m out of practice with the one whole night away from home thing! I arrived in Sydney without any toothpaste and three strips for my BGL meter. This was remedied with a quick visit to an NDSS pharmacy (for both strips and toothpaste). There were three jelly beans languishing around the bottom of my bag which weren’t going to be particularly helpful if I went low, so I popped into the convenience store across from the hotel to replenish hypo supplies.
I also forgot to pack spare diabetes consumables. Of course, I have my contingency bag that has one spare line and reservoir. But none of these spares helped when I ripped (and I mean ripped – blood everywhere!) my two day old sensor from my skin as I got changed.
Now, this wouldn’t have been a problem if I was not travelling alone. But being on my own without my CGM makes me nervous. A phone call to a friend living in Sydney who made a mercy dash into the city with a spare sensor has made me feel so much more relaxed.
I don’t wear a sensor all the time, but I do make a point to if I am travelling – especially if travelling on my own which I’ve really not done for some time. Ordinarily (at home), if I ripped a sensor out, I wouldn’t bother putting one straight back in. But I knew that I’d have a really restless night (of no sleep) without the security blanket that is an alarming-if-low CGM.
I used to do a lot of overnight travel and I had it just right. I had the packing perfect, I timed line changes just right and I had a mental checklist that I would work through with great skill and precision. I rarely – if ever – forgot anything.
Routine gets a bad wrap because it’s considered boring and unadventurous. And that may be the case. But the stress that comes from being without the necessary diabetes stuff – or having a really lousy hypo that could have been prevented with a CGM – is far more boring. And quite frankly, these are adventures I can do without!
Today, I am so pleased to have Jane Reid guest blog for me. I’ve never met Jane in real life (I hope to one day!), but we are friends on Facebook and seem to have very similar interests. We share a lot of posts about books, libraries, grammar and punctuation. Jane often posts really thoughtful and honest comments to my blog posts and I am always so interested to hear her opinion and experiences. Thanks for sharing today, Jane.
I have lived with T1 for 50 years – well, almost, but who’s counting?
It seems like a long time, but it has whizzed by. From diagnosis, (diabetic ketoacidosis and coma), to now, (pump, some hypo unawareness and some complications), I have lived it all with the help of my parents, my friends, my HCPs, and most of all, my husband who has put up with nearly 43 years of type 1. He told me yesterday that any sort of illness or set back that affects one of us is OUR problem. That is true love.
For the first few years I lived through what I call the ‘dark ages’. Glass syringes, horrible, large needles that went blunt quickly and testing (if you can call it that) with tablets dropped into a mixture of urine and water. If the result was blue, you were probably hypo; if the result was orange-brown you were high. My first specialist-physician (did they even have endos in 1965?) did me the greatest favour he could have. He told me that I would be the person who knew most about my diabetes, and he was correct. Thank you, Tom Robertson!

Jane
When I look back, I now realise that I had gastroparesis from quite early on, although it was only diagnosed ten years ago. Maybe I just didn’t want to know at that time, and I certainly never told any HCPs. I could probably have saved myself a lot of grief if I had.
The complication I really feared was retinopathy. I am a voracious reader, and I had heard gruesome tales of people going blind. Well, it wasn’t as bad as that, and it took over twenty years to develop. The treatment was worse than the fear, and the waiting around to see the ophthalmologist was worse than the treatment. I was treated by an ophthalmologist whom I can only describe as arrogant, and patronising. He did, however, save the majority of my sight, although I have almost no peripheral vision and can no longer drive.
I have had no treatment for over twenty years, so I guess he knew what he was doing. Losing my driving licence was the worst thing for me, although it was not until ten years ago. It has, to a certain extent, taken away my autonomy and independence, although every time I get into the car I know why I no longer drive. Believe me; everyone else on the road is safer because I’m not behind the wheel!
My latest complication is diabetic nephropathy (CKD). I was, to put it mildly, surprised and depressed when I found out. Luckily, the specialist I was sent to in the ACT, put me at ease, told me all about it, and arranged for a kidney biopsy. That showed that the disease was not nearly as bad as first thought, and was only at the very first stage. His comment to me was ‘I’m the same age as you, and I’ll look after you for the next seven years, and then I’ll hand you onto someone else when I retire’. That was reassuring!
I’d prefer not to have type 1 diabetes, but I can live with it. I’ve found out that I can live with complications; sure, I’d prefer not to, but they just become part of life. The worry and the fear are worse than the reality. I just do the best I can. None of us can do more than that.
Jane Reid is a proud member of the Newcastle Knights Rugby League Club and early next year will be eligible to receive a Kellion Medal for living with type 1 diabetes for 50 years – congratulations Jane!
Diabetes research funding – simply not enough
Last Friday, the successful National Health and Medical Research Council (NHMRC) grant recipients were announced.
Let’s start with the good news.
Funding for 848 grants was announced, totalling over $580 million across a wide range of health conditions. This includes project grants, partnership projects, Centres of Research Excellence and other Fellowships and grants.
This is great stuff. Medical research is essential and we should be encouraging more dollars being delivered to the very clever clinicians, researchers and scientists carrying out this important work. ‘Cures not Cuts’ is a motto we should be thinking about all the time – not only when there is a real or perceived threat to funding dollars.
Diabetes received $54 million in grants for 60 research projects.
Here is the not so good news.
Diabetes received $54 million in grants for 60 research projects.
That’s right. The good news is also the bad news. Whilst it is terrific that 60 research projects received funding and $54 million is not to be sneezed at, I do not believe that it is enough.
Cancer received funding of $89.9 million for 156 projects, and cardiovascular disease $82.4 million across 106 grants. All of these are worthy and should be funded. Make no mistake – I am not saying that money should not be given to cancer or CVD research. Of course I am not.
I am told that when funding announcements are made, there is also dissatisfaction amongst the cancer community, with many ‘lower profile’ cancers often being overlooked. Ovarian, pancreatic and lung cancer are frequently considered the poor cousins of the cancer world, despite significant numbers of people being affected by – and dying from – these cancers.
Of course, we can argue that the money is never enough. We can argue that we are all self-interested and only care about our own condition or the condition affecting our family and friends and to a degree, that is absolutely true.
Please understand, I am not saying that diabetes is worse than any other disease or health condition. Any regular readers of this blog will know that I absolutely do not subscribe to the ‘my condition is worse than yours’ arguments.
But if we are to believe that the magnitude of the ‘diabetes problem’ – and there is some pretty compelling evidence to support that it will indeed be the largest health burden in Australia by 2017 – then surely we need to see a bigger investment into diabetes research. We need diabetes to be’ top of mind’ as the number one health concern.
The results of last Friday’s funding announcements reinforce what I wrote here about diabetes having an image problem when it comes to funding – and fundraising. With more and more people affected, surely this should be reflected in increased funding for research, programs and services.
We’re not seeing that.
DISCLAIMER
At the risk of this outing me as someone with a case of sour grapes, I should acknowledge that I am listed as an Associate Investigator on a grant application that was not successful. Yes, I am disappointed. But this certainly was not the only diabetes grant that was unsuccessful. Many other very worthwhile applications faced a similar fate.
Congratulations to all the successful applicants.
I am as guilty as the next person of being judgemental at times. I like to think that I am not, but I’d be lying to myself if I honestly believed that I never uttered a pejorative comment about other people’s choices.
I really, really try to not be judgemental when it comes to how people choose to manage their diabetes. But I know that I am a zealot when it comes to technology and have been very, very guilty in the past of having conversations that sound like this
‘Are you on a pump? Why are you not on a pump? You should be on a pump? Pumps rock! Your life would be so much better if you were on a pump? That’s not a valid reason for not being on a pump. Do you want the details of my pump educator? Here, let me list the million reasons why I love being on a pump. Let me list them in a LOUDER VOICE to convince you. If you’re not on a pump you don’t really care about yourself.’
I know; I’m an absolute joy to be around sometimes.
But I’m trying to not be like this anymore. And to help remind me, I have made a poster of one of the things that has become a bit of a mantra and have it hanging in my office.

Feel free to substitute ‘diabetes’ for any other health condition. Or simply for the word ‘life’.
Because here’s the thing: when you make a decision about how you manage your diabetes, it is about your health. And that is an incredibly personal decision based on your own perspective, circumstances and experience. It’s got nothing to do with anyone else.
There is one caveat to this that I think is really important.
This works and is all fine as long as the decisions that you make as part of your ‘whatever’, (your diabetes, your life etc.) don’t negatively impact on others.
As a result, anti-vaxxers don’t get to claim this as their own. Because their irresponsible actions do affect others.
Same goes for doing anything that emotionally or physically hurts another person, or has the potential to.
Actually, also goes for people who wear leggings as pants. Because, LEGGINGS ARE NOT PANTS and your decision to treat them that way hurts my eyes.
BUT! If you are making decisions that impact on you and you alone, knock yourself out. You don’t owe anyone an explanation or need to justify your choices. Own it.
About two months ago, I realised something. It came as a bit of a shock because I have had some pretty difficult and dark times over the last couple of years.
I realised that I am okay with who I am.
I know that it sounds kinda clichéd and like I’ve been reading a book of inspirational quotes (which I’ve not!) but it was a little of a revelation. Because for some time now, I’d felt like I really didn’t like who I was.
This all happened one afternoon as I listened to my daughter and a couple of her friends playing outside. They were sprawled out on the front veranda, lying on their stomachs, drawing, looking up occasionally to see what our new puppy was up to. In between such busy-ness, they were speaking about what they liked about each other and what they liked about themselves.
I love this about kids. Before they develop the ‘I must hate and criticise myself lest people think I am up myself’ gene, they feel free to say that they are pretty damn great. Because they are.
My daughter is really lovely when people compliment her. She smiles and says ‘thank you’. And sometimes, she says ‘I know’. It’s beautiful and honest.
‘You’re a great reader,’ I told her the other day when she told me she wanted to read Anna Karenina (seriously – no idea, but she’s six chapters in and loving it). ‘I know. I love to read,’ she answered. She didn’t sound boastful or conceited. She was acknowledging what I said as the truth. Because, it is!
When someone compliments me, I make up every reason to discredit their comment which, when you think about it, is actually very rude.
Having a chronic health condition makes it really easy to think that we are not enough or that we are broken. Add to that any other health concerns and suddenly, we can start to think of ourselves as hopeless. And when we start to add feelings of distress and a significant reduction in our emotional wellbeing, things get worse and worse.
Supplement that with other things that are getting us down and it is only a little hop, step and jump away from feeling hopeless, desperate and desolate. It’s hard to see anything good in ourselves.
The bottom line is that I stopped liking myself. I stopped being able to see the good or the positives and I simply could not be proud of anything that I was doing – even though during that time I knew I was doing some pretty amazing things.
I’m not sure what it was that jolted me out of this. I’d like to think it was ‘bolt-of-lightening’ like, but I don’t think it was. Perhaps it is the robustness that comes with age that reminds us that actually, through the shit, there is good. And a rather Pollyanna-ish attitude that ‘this too will pass’.
I listened to the kidlets and smiled. And then I remember thinking ‘Actually, I’m okay too. I really do like myself. I deserve to have good things happen to me, because I am worthy and good.’
I stopped thinking about my health problems as things that made me fragile and shattered, instead conceding that they are part of the sometimes fragile fabric that when put together makes up me.
I stopped thinking that the things that had been upsetting me where a reflection of the person I was and accepted that many of those particular things were out of my control and had nothing to do with me.
And just like a patchwork quilt, when you look at the pieces alone they don’t make sense and they are not really useful or beautiful or amazing or wonderful.
But when you put them together, they work.
I like myself. And it’s a really, really, really amazing place to be.
We need hope. I know that every day I live in great hope.
- Hope that I will find the perfect pair of jeans in the perfect blue colour that make my legs look long and slender, my backside look perfect and that fit comfortably around the waist.
- Hope that I will walk into my office one day to find a Nutella vending machine.
- Hope that I will never again be served bad coffee.
- Hope that my daughter will grow up in a world of equality for all.
- Hope that when I get home today all the washing from our recent overseas trip will have been done, folded and put away.
- Hope that I will walk into a vintage store and find an original (non-replica) Eames arm chair and ottoman for $150.
- Hope that the whole cast of West Wing will come together for a movie. Please. Please, please, please, please.
- And hope that diabetes will be cured.
You may have read over the weekend that type 1 diabetes has been cured. This article irresponsibly said the cure is ‘imminent’
I am possibly the world’s greatest cynic when it comes to reading about cures for diabetes. There is much eye rolling, exasperated sighing and sarcastic comments about being unemployed and shutting down this blog because no one will care about type 1 diabetes anymore because it won’t exist.
I simply don’t believe that the cure is ‘just around the corner’ or ‘five years away’.
But let me be really clear about this. I want a cure. I want diabetes to not be a part of my – or anyone’s – life anymore. And I am really, really pleased and eternally grateful that there are people far, far smarter than I working to find the way to a cure.
Having said that, I get concerned about the false hope that eventuates every time there are reports of research breakthroughs. 
Feeling hope gives us a reason to believe and sometimes that is all we have to get us through the day.
But equally, I find I can’t put all my faith into believing that there will be a cure for diabetes because if there is not, what happens then?
I understand the need for the hype – it helps with funding and interest and gets people talking. And we need people talking about and funding research into diabetes. More and more and more.
And I do like to hear about the research and breakthroughs that are getting us a step closer to finding a cure.
But I believe that even if we are a step closer, there is still a very long way to go.
So, I take it all with a grain of salt. I read it and file it away. And then I move on. Hopeful. But realistic as well.






