
You are currently browsing the category archive for the ‘Awareness’ category.
On November 14, the world will literally light up in blue to celebrate World Diabetes Day. And here in Melbourne, an event highlighting one of the most important issues in diabetes today will be held. The entire event will be dedicated to how the global diabetes community is coming together to work to #EndDiabetesStigma. And you can be there!

I’m delighted to be sharing the hosting seat with Dr Norman Swan, physician, journalist and host of Radio National’s Health Report. A veritable A-Team of people from the international diabetes community will be part of the event, sharing their experiences of diabetes stigma and why efforts to end it are so necessary and timely. There will be representatives from the global lived experience community, diabetes organisations and health professionals and researchers. You really don’t want to miss it!
For those able to attend in person, you’ll have a chance to catch up with diabetes mates. Any chance for opportunistic peer support is a great thing and I’m so pleased that I’ll be seeing diabetes friends that I’ve not seen for a very long time.
This isn’t only for Melbourne locals. There will be a livestream for people around the world to watch, share and be part of on social media. It’s free to attend and will be a great opportunity to see the diabetes world come together on a day dedicated to us!
Australian airports seem to have become a battleground recently for travellers with diabetes. My own experiences since Australia opened back up to travel have been appalling and each week there are reports in online diabetes pages about some pretty horrendous experiences. Specifically, the problems are to do with full body scanners which have been rolled out across international security checkpoints nationally, and some domestic checkpoints.
This year alone in half a dozen international flights out of Melbourne Airports and a dozen or so domestic flights, all been much more difficult than any travel experience pre-COVID. I documented one particularly brutal encounter at Brisbane Airport last year in this Twitter thread. Sadly, since then, other instances have been just as awful.
It seems that the training modules for security staff have incorrect information about which scanning devices are safe for diabetes devices. In my experience, the messaging is consistent: staff have been told that the metal detectors (the older walk-through screeners) are unsafe while the newer full body scanners (the stand still and be scanned) are safe. This is at odds with information from device companies and health professionals and has resulted in a number of people reporting clashes at security checkpoints.
There’s so much discussion about this, as well as lots of confusion and some pretty dire misinformation across OzDOC socials, some of it coming from diabetes groups. Let me try to break this down with information that is based on advice from device companies and the Department of Home Affairs. This is what I have used to try to help me streamline my own travel experiences – with varying levels of success.
Firstly, let’s start with the Department of Home Affairs. This page has the information you need, but specifically, under the section Travellers who have a mobility aid, prosthetic, medical device or medical equipment is this: ‘If you have a medical device or medical equipment, it may streamline the screening process if you have a letter or medical identification card from your doctor or healthcare professional that describes the device or equipment. It is also recommended that you talk with your doctor, healthcare professional or check the manufacturer instructions for guidance on whether the medical device or equipment is suitable for screening by body scanner technology or X-ray technology, and if not, make the screening officer aware of any restrictions before beginning the screening process.’
Device companies all have their own advice, so familiarise yourself with what their recommendations. I wear a Dexcom, and carry a printed copy of security screening advice. At the end of this post you’ll find links and relevant information about the different devices available in Australia.
Knowing how tricky things are likely to be, I am super prepared for security checks now. I carry a letter from my endocrinologist that states I’m wearing diabetes devices that must not go through the full body scanner, and that my pump cannot be removed (not so relevant these days as I wear Omnipod). In a sign of just how much the times have changed, I now need to show that letter about 80% of the time at Australian airports. Pre-COVID I maybe needed to produce it twice in hundreds of journeys.
I always remain calm and clear about what I need: ‘I am wearing medical devices and cannot go through the fully body scanner. I can go through the metal detector, or I need a pat down. I’m happy to wait out of your way.’ I stand firm with this request, remaining polite and calm even when there is increasingly aggressive pushback. In most cases, security staff will tell me that the training says body scanners are safe and metal detectors are not. At this point, I offer the letter from my doctor and the printed out advice from Dexcom and mention the relevant information from the Department of Home Affairs. If there continues to be pushback, I’ll ask to speak with a supervisor. I truly hate doing this.
While this isn’t applicable to me now, at no point ever would I remove my insulin pump and hand it to security staff for inspection. Disappointingly, some of the device companies’ travel advice (and today I saw advice from a diabetes centre) suggests this. Don’t do it. I am happy for them to swab it while I hold it, but I won’t disconnect and hand it over. Items go missing and handed to the wrong person or could be damaged at busy security checkpoints.
I know others with diabetes are happy to go through whatever scanner they are directed to and have had no adverse issues and that’s great. But this isn’t about individual experiences so much as about how to manage situations according to manufacturers’ advice and knowing what official information from the relevant Government department is. It’s also about being treated respectfully and having our own lived experience and knowledge respected by security staff; something that sadly seems to be repeatedly forgotten.
If you’ve had a lousy experience and have the emotional labour to write a complaint to the airport, please do so. There are online forms you can use.
It would be really great if this additional work didn’t fall to people with diabetes. Device companies could step up here and provide cards to use at security checkpoints, similar to those that have been developed for people with pacemakers and knee and hip replacements. Simultaneously it would be great if there was a form that could be personalised and printed out or a card issued via the NDSS when people register for pump and/or CGM access (this wouldn’t serve people who are self-funding, but it would reach the majority of Australians affected). While I am sure that there are efforts underway to address it, there’s no time to wait and a temporary fix is needed immediately. And any other advocacy groups who are addressing this issue can make sure that the advice they are providing on behalf of their diabetes community is accurate and best serves the needs of people with diabetes.

Advice from device companies in Australia
AMSL has this advice for Dexcom users: ‘Use of AIT body scanners has not been studied and therefore Dexcom recommend hand-wanding or full- body pat down and visual inspection in those situations.’
Insulet Australia has this advice for Omnipod users: ‘The Omnipod DASH® PDM and Pods are safe to go through the x-ray machine and the Pods are safe to be worn through airport scanners.’
AMSL has this advice for Tandem T:Slim users: ‘your Tandem Diabetes Care insulin pump should NOT be put through machines that use X-rays, including airline luggage X-ray machines and full-body scanners.
Medtronic has this advice: ‘Your pump should not go through the x-ray machine that is used for carry on or checked luggage or the full body scanner.’
Abbott has this information for FreeStyle Libre wearers: ‘The FreeStyle Libre reader and the FreeStyle Libre sensor can be exposed to common electrostatic (ESD) and electromagnetic interference (EMI), including airport metal detectors. You can keep your FreeStyle Libre sensor on while going through these. However, the FreeStyle Libre reader and the FreeStyle Libre sensor should not be exposed to some airport full body scanners.’
A very quick post to invite you all to attend a fascinating session being held tonight as part of the Nossal Institute for Global Health’s Navigating Health Globally webinar series. With the beautifully alliterative title, Compassion, Care, Complexity & Culture, we will explore how diverse healthcare approaches can tackle limited access to health systems and fragmented care, focusing on shared care as a means to foster person-centred systems as part of person-centred care.
I’m so delighted that I get to open the event with a talk about compassion in healthcare: what it looks like, my own experience of working with remarkably compassionate healthcare professionals, and also, the impact on our experiences of healthcare when compassion is lacking.
The other presenters are remarkable and I am so honoured to offer the lived experience lens on stage with them. You’ll hear from Professor Victor Montori, endocrinologist, researcher and Professor of Medicine at the Mayo Clinic, Duleep Allirajah, CEO of the Richmond Group of Charities (a coalition of 12 national health and care charities), Dr Guy Fones, Head of Global Coordination Mechanism on NCDs, World Health Organization and James Sanderson, Director of Community Health Services and Personalised Care, NHS England. Expect me to be totally fan-girling when Professor Victor Montori is up, speaking about his Patient Revolution (if you don’t have a copy of his book Why We Revolt, add to cart now).
I know that the healthcare experiences I value the most – the ones that have helped me, left me feeling inspired and supported, valued and listened to – have all been founded in compassion. Sadly, it’s not necessarily guaranteed. I’m looking forward to highlighting the experiences, (and the healthcare professionals behind them), that have been powered by compassion. I hope to see you in the (virtual) audience.
Kick off time is 8.00pm AEST, (or 10.00pm NZST, 6.00am EST, 11.00am BST, 12.00pm CEST). It’s free to attend, but you will need to register (to watch live, or stream later at a reasonable hour). Details are here.
Diabetes stigma is a hot button topic in the diabetes world. It has been for some time. I wrote just last month how stigma was one of the most talked about issues at ADA. That week, we also launched an Open Letter from the Diabetes Community, asking health professionals to join us in our call to stop diabetes stigma.
And behind the scenes, for all of this year, another exciting, BIG, project has been hatching and I’m so excited to share it today.
Earlier this year, in an unprecedented show of unity and determination, a group of 51 experts from 18 countries joined forces to pool our lived, research and clinical experience to address diabetes stigma and discrimination. Together, we’ve reviewed the scientific evidence and established an international consensus on 49 Statements of Evidence and Recommendations. The full report on this review has been submitted and is currently under review.
Excitingly, the group also reached a consensus on a Pledge dedicated to bringing an end to diabetes stigma and discrimination. And that’s where you come in! Everyone can sign to show your commitment stop the ingrained negative judgments, stereotypes, and prejudices that influence attitudes about diabetes, and contribute to the stigma so many of us face. This isn’t just for the community. We know there is sometimes an echo chamber as we say the same things to each other, over and over. We also know that while diabetes stigma is indeed prevalent within our community, we also need to tell the story of its harm outside the diabetes world.
Well, here’s an easy way to do both. Please sign the pledge and share details across your social platforms. You can sign as an individual, and we’d also love for you to see if your place of work, school, community group, hospital, church, sporting team, favourite cafe…basically anywhere that is likely to come into contact with people with diabetes (i.e. literally everyone!) would be interested in signing too.
This is a true community effort, with involvement from stakeholders from across the diabetes landscape, across the world. You won’t see logos anywhere, because this for and about all people with diabetes. The names of the people involved in the work so far is on the website.
Are you with us?

All too frequently, when talking about meaningful lived experience engagement, I hear about ‘Hard to Reach Communities’. A number of years ago, I called rubbish on that, putting a stop to any discussion that used the term as a get out of jail free card to excuse lack of diversity in lived experience perspectives.
‘People with type 2 diabetes don’t want to be case studies’ or ‘Young people with diabetes don’t respond to our call outs for surveys’ or ‘People from culturally and linguistically diverse communities won’t share their stories’ or ‘Folks in rural areas don’t come to our events’. These are just some real life examples I heard when asking why there was no diversity in the stories I was seeing.
See how the blame there is all on the people with diabetes? They don’t want, don’t respond, won’t share, won’t attends. It’s them. They’re the problem. It’s them.
I stood on stage at EASD in Stockholm last year and challenged the audience to stop using the term ‘hard to reach’. Because that’s not the case at all. The truth is that in most cases, the same old, uninventive methods are always employed. And those methods only work for a very narrow segment of the community.
I recently heard someone begrudge that all applicants who responded to a recent call out for a new committee were the same: white, had type 1 diabetes, city-dwelling. ‘Of course they are,’ I said. ‘That’s the group that loves a community advisory council and responds to an expression of interest call out on socials. They are able to attend meetings when they are scheduled, are confident to speak up and are willing to share their story, because they probably have before and received positive feedback for doing so Plus, they’re expecting everyone else at the table will look and sound just like them.’
But the lack of diversity isn’t the problem of the people who didn’t respond. It’s the problem of whoever is putting out a call and expecting people to reply because that’s how it’s Always Been Done.
This was a discussion at a meeting during last week’s American Diabetes Association Scientific Sessions. The #dedoc° voices were meeting with the ADA’s Chief Scientific Officer, Dr Bob Gabbay, and Vice President in Science & Health Care, Dr Nicole Johnson. The question about how to reach a broad audience was asked. At #dedoc°, efforts have been made to attract a diverse group of people to our scholarship program, and have, to a degree there as been some success. A glance at any one of the #docday° events, or scholarship alumni will see people who had not previously been given a platform within the diabetes community. But there is always more than can be done.
The discussion in that meeting at ADA mirrored many that happened throughout the week. And it’s not surprising that US diabetes advocate Chelcie Rice came up with the perfect way to explain how to do better at engaging with the who have previously been dismissed as ‘hard to reach’. He said: ‘You can’t just put pie in the middle of the table. Deliver the pie to where they are.’ And he’s right. Those tried and true methods that work for only one narrow segment of the community have been all about putting pie in the middle of the table, knowing that there will be some people ready with a plate and a fork. But a lot of people are not already at the table, or comfortable holding out their plate. Or maybe they don’t even like that pie. But we never find out because no effort is really made.
Chelcie once said ‘If you’re not given a seat at the table, bring your own chair‘ and I’ve repeated that quote dozens, if not hundreds of times. And his words ring very true for people like me who have felt very comfortable dragging my own chair, and one for someone else and insisting that others scramble to make room for us. But that metaphorical table isn’t enough anymore. Not everyone wants to sit at a table and we need to stop expecting that. Instead, it’s time to find people where they are – the places, the settings, the environments they feel comfortable and at home. That’s how you do engagement.

On day 2 of the American Diabetes Association Scientific Sessions, rushing between meetings, I overhead another attendee say this: ‘I’ve never heard so many people talking about diabetes stigma’. I turned to them, a bright smile on my face and said, ‘I know, right?’, (a phrase I only ever utter when I’m in the US).
Just a few hours earlier, Jazz Sethi and I had tweeted simultaneously, setting free an open letter from the diabetes community about diabetes-related stigma. You may have seen it; thousands of people have. And others have shared, commented and even translated it into different languages (I think we’re at 6 translations and counting). Here it is!



When we first asked advocates from the community if they would like to add their logo to the letter we were surprised by the quick response. Almost everyone we went to said yes. We hadn’t gone out too widely – we wanted to test the waters first. The first version of the open letter includes advocates and peer support groups from across the world. Amazing!
And after our very low-key, (i.e. a couple of tweets from unverified Twitter accounts, so who knows what the algorithm did with them!), we were once again inundated by people asking for us to add their logos. (We haven’t managed to add them yet, but absolutely will in coming weeks. Please give us time if you’ve shared your logo. We’ll get there. And I’ll update this post with the new final page when that happens.)
There is something magic about these sorts of very grassroots, very community, very inclusive initiatives. Not only are they great because they collaboratively offer a narrative from people with diabetes, highlighting an issue that is of great importance to many. They also show you just how powerful and united our community is while also pointing to individuals and groups who are keen to work together, support each other and power the importance of lived experience. And that’s pretty special!
Imagine a community where people come together to make things happen. You don’t have to look far, really. Just look at the diabetes community!
Here’s something new from some folks (Jazz Sethi, me and Partha Kar) who are desperately trying to reshape the way diabetes is spoken about, and how fortunate I feel to have been involved in this project!

The thinking behind these particular language resources is to truly centre the person with diabetes when thinking about communication about the condition. In this series, we’ve highlighted three groups where we know (because these are the discussions we see in the diabetes community) language can sometimes be stigmatising and judgemental. This isn’t a finger-pointing exercise. Rather it’s an opportunity to highlight how to make sure that the words, images, body language – all communication – doesn’t impact negatively on people with diabetes.
A massive thanks to Jazz and Partha. Working together, and with the community, to create and get these out there has been a joy. (As was sneaking into the ATTD Exhibition Hall before opening time so we could get a coffee and find a comfortable seat to work before the crowds made their way in!) And a super extra special nod to Jazz who pulled together the design and made our words look so bright pretty! And a super, super, super special thanks to Jazz for designing my new logo which is getting its first run on the back of these guides.
You can access these and share directly from the Language Matters Diabetes website. These don’t belong to anyone other than the diabetes community, so please reach out if you would like to provide any commentary or be involved in future efforts. There’s always more to do!

On Sunday, one of those annoying diabetes things happened – a kinked insulin pump cannula, subsequent high glucose levels followed by a little glucose wrangling tango where, instead of rage blousing, I tried to gently guide my numbers back in-range. I thought about how frustrating diabetes can be – unfairly throwing curve balls at us even when we are doing ‘all the right things’. And so, I used this little story for a post on LinkedIn to illustrate why I am so dedicated to making sure that stories like this are heard and lived experience is centred in all diabetes conversations.
Meanwhile, anyone who has even the barest of little toes dipped in the water of the diabetes community would have heard about Alexander Zverev being told by French Open officials that he was not permitted to take his insulin on court. He was expected to inject off court and, according to Zverev, was told ‘looks weird when I [inject] on court’. Insulin breaks would be considered as toilet breaks.
What’s the connection between this story and my LinkedIn story? Absolutely none. Except there kind of is.
I’m not about to write about sports or try to connect my story with that of a top-ranking tennis player. That would be totally out of my lane. (The couple of years of tennis I took when I was in grades five and six give me no insight into life of a tennis player.)
However, when it comes to discussing diabetes and the stigma surrounding it, I’m definitely in my lane. I understand and am very well-versed when it comes to talking about the image problem diabetes faces and how that fuels the stigma fire.
The response from the diabetes community when the Zverev story broke. Most people were incredibly supportive of the tennis player and rightfully indignant of the incident. JDRF UK responded swiftly with an open letter to the French Open organisers, eloquently highlighting why their ruling needed to be changed. And changed it was.
My LinkedIn post was shared a few times and there were comments from people saying that these stories help others better understand our daily challenges and work to cut through a lot of the misconceptions about diabetes.
And then there was this direct message:
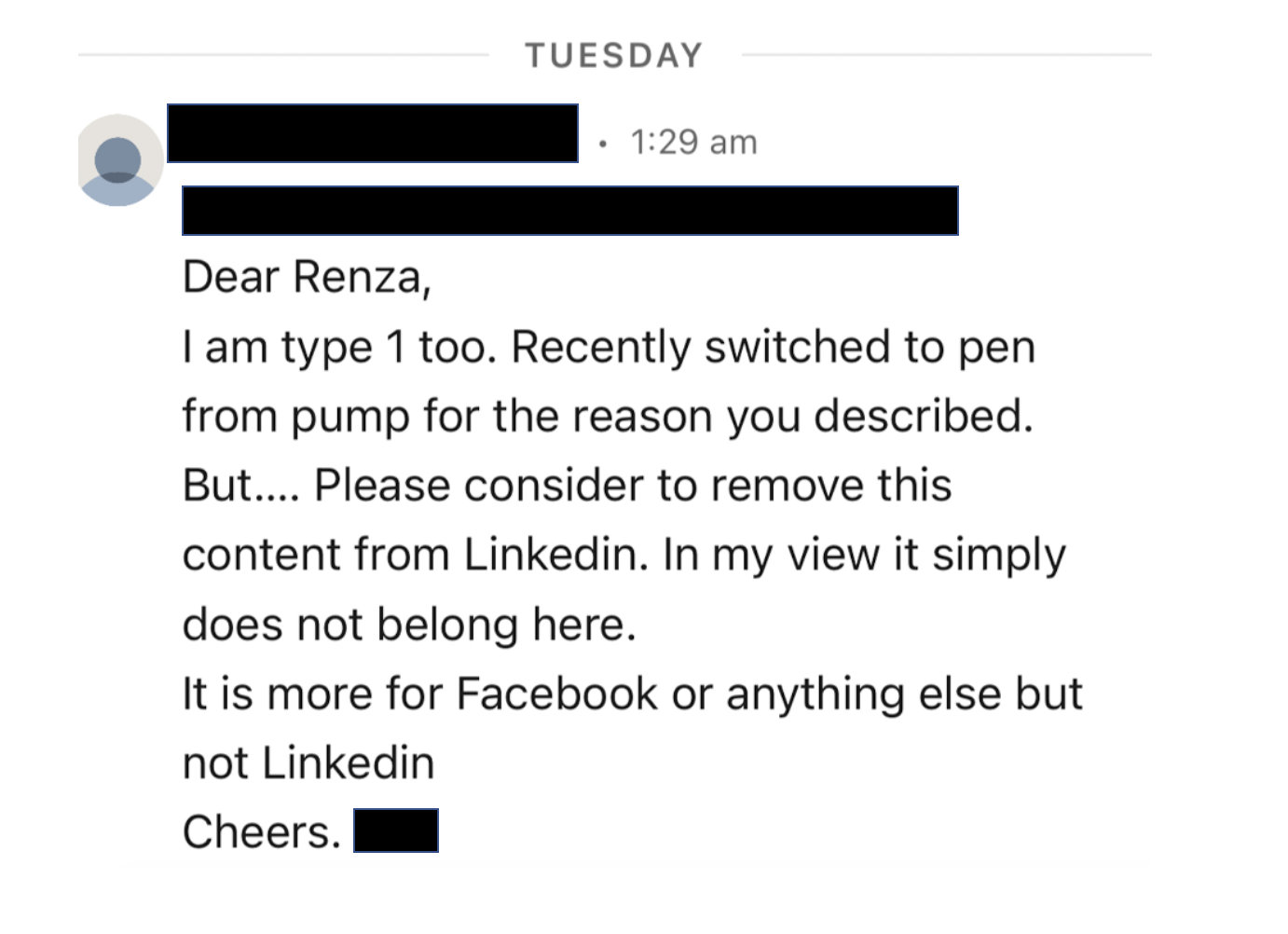
I bristled as I read it. My initial response was ‘How dare this man try to tell me what I can and can’t post on LinkedIn. Who is he to tell me what I can and can’t share?’ I snapped a reply back to him where I pointed out: ‘…I am a diabetes advocate, working to change attitudes and raise awareness about living with diabetes. My post belongs here on LinkedIn as it very much aligns with the work I do.’
But I haven’t been able to stop thinking about it because as problematic as it is for someone trying to silence what people with diabetes share online, there was more that was troubling me.
The idea that diabetes is a topic only appropriate in certain contexts and should be hidden away from others reinforces shame. Suggesting work settings are not the place to talk diabetes plants that seed that diabetes, and people with diabetes, could be liabilities in the workplace. Talking about diabetes on LinkedIn – a platform for business and workplace networking – is relevant because people with diabetes exist in business and workplaces, and the reality is that diabetes sometimes interferes with our work. Which is perfectly okay. Last week, I needed to refill my pump during a meeting. So, I let others on the call know what I was doing and carried on. On another day, I was recording a short video about a research program and after take 224 realised I needed to treat a hypo and did so. I shouldn’t need to feel that these aspects of daily life with diabetes are only allowed to happen out of view.
Essentially, this is what Alexander Zverev was being asked to do at his workplace: hide away when he needed to perform a task that keeps him alive, as if there is something shameful and disgusting about it. In my mind, this top ranked tennis player playing in a Grand Slam competition should be commended. I mean, any tennis player who does that is remarkable. Zverev does it and then goes about performing the duties of a pancreas. His opponents don’t have to do that! Their pancreas doses out the perfect amount of insulin without any help. Talk about an unfair advantage!
Not everyone wants to talk diabetes with others and that’s fine. But those of us who are happy to speak about and ‘do diabetes’ wherever we are shouldn’t feel that we are doing anything wrong. Diabetes stigma exists because there are so many wrong attitudes about diabetes. It’s insidious and it’s damaging. It erects barriers creating a climate of shame and perpetuates misconceptions that lead to ignorance. And it pressures us to hide away the realities of diabetes, as if there is something to be ashamed of. But there is nothing shameful about living with diabetes. There is nothing shameful about injecting insulin on Centre Court at Roland-Garros, or sharing frustrations on LinkedIn. Or anywhere else. Diabetes has a place wherever your workplace might be. Stigma, however, does not.

I woke up (at 4am thanks to a hypo, but that’s another story all together) and scrolled through a variety of social media feeds and, because I seem to follow a lot of diabetes-related pages and people, was bombarded with the below. And so, these are my very early morning musings, a stream of consciousness mess, the logic and rationality of which is most likely influenced by low blood sugar. (The typos, however, are all mine.)
So, let me begin by saying that this is important work – of course it is. The DiRECT trial has really put the idea of diabetes remission on the research agenda, encouraging further research into the issue, provided another potential diabetes treatment option for people with type 2 diabetes, and supporting people with type 2 diabetes looking at this way of managing their diabetes. Choice. It’s a good thing!
Today we have some follow up data (after the initial two years of the trial), providing updates on how research participants are going. Again. It’s important research, and it is helping increase knowledge and understanding of type 2 diabetes. Good stuff!
But one of the things I am all about is accuracy in reporting and this, my friends, isn’t it.
I wasn’t going to even touch the heading of the article, because surely the inaccuracy of it doesn’t need highlighting at all, but let’s go there anyone. The DiRECT trial is researching people with type 2 diabetes, and it probably would be good to mention that. I guess that nugget is in the sub-heading, but it might be good to not relegate it there.
But let’s look at that sub-heading. ‘Stay free of symptoms’ is an interesting thing to highlight when we know that in many cases, people with undiagnosed T2D don’t have any symptoms anyway. Surely focusing on what it means in terms of day-to-day life with diabetes (i.e. medication, monitoring requirements, daily burden of ‘doing diabetes’, frequency of HCP visits) would be more meaningful.
Back to the heading and we have the word reverse which is pretty much incorrect in all ways possible. The word they’re looking for is remission. Why? Because even if the result from those in the study is that they don’t require diabetes meds, and their glucose levels are back in range, they still do have diabetes.
I’m not a statistics person. Data hurts my head and numbers make me cry, and I get the complete and utter irony of saying that considering that I live with a condition that depends on me understanding data and numbers, but now is not the time to come at me and my 2.9mmol/l self. Please and thank you.
But there is a number in this research that seems to be jumping out at me and it’s this number: 23%. Let me clarify (this is from the Diabetes UK press release): 23% of participants who were in remission from type 2 diabetes at two years in the original trial remained in remission at five years.
It’s important to also point out that this isn’t 23% of the total people who started in the DiRECT trial five years ago – not all participants were in remission after two years. At two years, 36% remained in remission. Or 53 out of the original 149 research participants in the intervention group (plus a additional 5 people in the control group).
So that 23% is of 58 people who remain in remission now at five years. That’s 13 people. Or about 8% of the starting number. That’s a very different story to what is being presented in news stories, media releases and cross socials today, isn’t it?
And that matters. Big time. Because there is real danger that many people will read the media reports today and in their minds that will mean that remission from type 2 diabetes is a far more likely outcome than reality and is the likely outcome for everyone.
I’m not here to argue whether remission is a thing or not – it is. FOR SOME PEOPLE with type 2 diabetes. Adding pieces to help understanding of the giant puzzle that is diabetes is brilliant for everyone. Research helps us do that. Sharing that research so that people living with diabetes better understand the options available and learn more about how our particular brand of diabetes works is gold!
But I am here to argue that publishing grand sweeping statements about how to ‘reverse’ type 2 diabetes, or telling only part of the story about the research, without the necessary nuance, is inaccurate and will further stigmatise type 2 diabetes and those living with it, especially those who are not able to achieve remission of their condition. The very idea that they could be made to feel that they are not trying hard enough or that they have failed is not being sensationalist.
The stigma associated with type 2 diabetes is considerable and everyone has a responsibility to making it better and not add to it. And surely an even heavier burden of that should fall to those who are working in diabetes. If my 4am, glucose-starved brain is able to grasp how stigmatising something like this could be to people with type 2 diabetes, then it should be glaringly obvious to anyone who has even a passing interest in the condition.
There’s been quite a bit of discussion after yesterday’s post about a recent consultation I did with a creative agency looking to develop a campaign about diabetes-related complications. I try to be solutions oriented and offer ideas, rather than just swoop in and be critical, so with that in mind, I’ve put together a couple of checklists that may be of some assistance when thinking about ways to talk about complications.
Of course, as always, these are just my suggestions and others may completely disagree with them, or having more to add. But this is a start that can be considered, shared and built on. And it comes with the ever present reminder that people with diabetes deserve to see themselves represented in ways that don’t make us want to run for the hills or hide under the doona (duvet) and never come out. That’s always a really good place to start!







