You are currently browsing the category archive for the ‘Advocacy’ category.
Imagine a community where people come together to make things happen. You don’t have to look far, really. Just look at the diabetes community!
Here’s something new from some folks (Jazz Sethi, me and Partha Kar) who are desperately trying to reshape the way diabetes is spoken about, and how fortunate I feel to have been involved in this project!

The thinking behind these particular language resources is to truly centre the person with diabetes when thinking about communication about the condition. In this series, we’ve highlighted three groups where we know (because these are the discussions we see in the diabetes community) language can sometimes be stigmatising and judgemental. This isn’t a finger-pointing exercise. Rather it’s an opportunity to highlight how to make sure that the words, images, body language – all communication – doesn’t impact negatively on people with diabetes.
A massive thanks to Jazz and Partha. Working together, and with the community, to create and get these out there has been a joy. (As was sneaking into the ATTD Exhibition Hall before opening time so we could get a coffee and find a comfortable seat to work before the crowds made their way in!) And a super extra special nod to Jazz who pulled together the design and made our words look so bright pretty! And a super, super, super special thanks to Jazz for designing my new logo which is getting its first run on the back of these guides.
You can access these and share directly from the Language Matters Diabetes website. These don’t belong to anyone other than the diabetes community, so please reach out if you would like to provide any commentary or be involved in future efforts. There’s always more to do!

On Sunday, one of those annoying diabetes things happened – a kinked insulin pump cannula, subsequent high glucose levels followed by a little glucose wrangling tango where, instead of rage blousing, I tried to gently guide my numbers back in-range. I thought about how frustrating diabetes can be – unfairly throwing curve balls at us even when we are doing ‘all the right things’. And so, I used this little story for a post on LinkedIn to illustrate why I am so dedicated to making sure that stories like this are heard and lived experience is centred in all diabetes conversations.
Meanwhile, anyone who has even the barest of little toes dipped in the water of the diabetes community would have heard about Alexander Zverev being told by French Open officials that he was not permitted to take his insulin on court. He was expected to inject off court and, according to Zverev, was told ‘looks weird when I [inject] on court’. Insulin breaks would be considered as toilet breaks.
What’s the connection between this story and my LinkedIn story? Absolutely none. Except there kind of is.
I’m not about to write about sports or try to connect my story with that of a top-ranking tennis player. That would be totally out of my lane. (The couple of years of tennis I took when I was in grades five and six give me no insight into life of a tennis player.)
However, when it comes to discussing diabetes and the stigma surrounding it, I’m definitely in my lane. I understand and am very well-versed when it comes to talking about the image problem diabetes faces and how that fuels the stigma fire.
The response from the diabetes community when the Zverev story broke. Most people were incredibly supportive of the tennis player and rightfully indignant of the incident. JDRF UK responded swiftly with an open letter to the French Open organisers, eloquently highlighting why their ruling needed to be changed. And changed it was.
My LinkedIn post was shared a few times and there were comments from people saying that these stories help others better understand our daily challenges and work to cut through a lot of the misconceptions about diabetes.
And then there was this direct message:
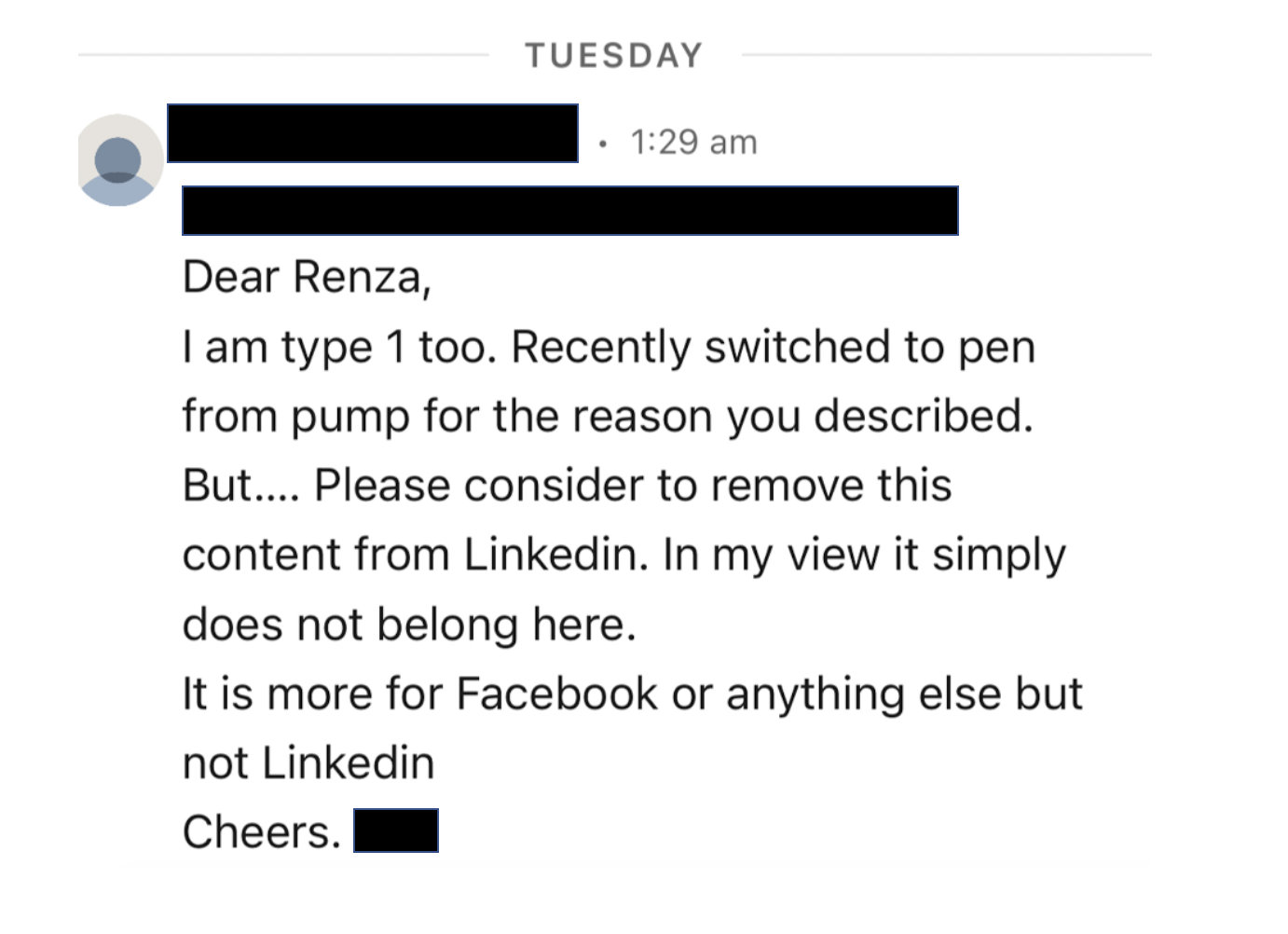
I bristled as I read it. My initial response was ‘How dare this man try to tell me what I can and can’t post on LinkedIn. Who is he to tell me what I can and can’t share?’ I snapped a reply back to him where I pointed out: ‘…I am a diabetes advocate, working to change attitudes and raise awareness about living with diabetes. My post belongs here on LinkedIn as it very much aligns with the work I do.’
But I haven’t been able to stop thinking about it because as problematic as it is for someone trying to silence what people with diabetes share online, there was more that was troubling me.
The idea that diabetes is a topic only appropriate in certain contexts and should be hidden away from others reinforces shame. Suggesting work settings are not the place to talk diabetes plants that seed that diabetes, and people with diabetes, could be liabilities in the workplace. Talking about diabetes on LinkedIn – a platform for business and workplace networking – is relevant because people with diabetes exist in business and workplaces, and the reality is that diabetes sometimes interferes with our work. Which is perfectly okay. Last week, I needed to refill my pump during a meeting. So, I let others on the call know what I was doing and carried on. On another day, I was recording a short video about a research program and after take 224 realised I needed to treat a hypo and did so. I shouldn’t need to feel that these aspects of daily life with diabetes are only allowed to happen out of view.
Essentially, this is what Alexander Zverev was being asked to do at his workplace: hide away when he needed to perform a task that keeps him alive, as if there is something shameful and disgusting about it. In my mind, this top ranked tennis player playing in a Grand Slam competition should be commended. I mean, any tennis player who does that is remarkable. Zverev does it and then goes about performing the duties of a pancreas. His opponents don’t have to do that! Their pancreas doses out the perfect amount of insulin without any help. Talk about an unfair advantage!
Not everyone wants to talk diabetes with others and that’s fine. But those of us who are happy to speak about and ‘do diabetes’ wherever we are shouldn’t feel that we are doing anything wrong. Diabetes stigma exists because there are so many wrong attitudes about diabetes. It’s insidious and it’s damaging. It erects barriers creating a climate of shame and perpetuates misconceptions that lead to ignorance. And it pressures us to hide away the realities of diabetes, as if there is something to be ashamed of. But there is nothing shameful about living with diabetes. There is nothing shameful about injecting insulin on Centre Court at Roland-Garros, or sharing frustrations on LinkedIn. Or anywhere else. Diabetes has a place wherever your workplace might be. Stigma, however, does not.

I woke up (at 4am thanks to a hypo, but that’s another story all together) and scrolled through a variety of social media feeds and, because I seem to follow a lot of diabetes-related pages and people, was bombarded with the below. And so, these are my very early morning musings, a stream of consciousness mess, the logic and rationality of which is most likely influenced by low blood sugar. (The typos, however, are all mine.)
So, let me begin by saying that this is important work – of course it is. The DiRECT trial has really put the idea of diabetes remission on the research agenda, encouraging further research into the issue, provided another potential diabetes treatment option for people with type 2 diabetes, and supporting people with type 2 diabetes looking at this way of managing their diabetes. Choice. It’s a good thing!
Today we have some follow up data (after the initial two years of the trial), providing updates on how research participants are going. Again. It’s important research, and it is helping increase knowledge and understanding of type 2 diabetes. Good stuff!
But one of the things I am all about is accuracy in reporting and this, my friends, isn’t it.
I wasn’t going to even touch the heading of the article, because surely the inaccuracy of it doesn’t need highlighting at all, but let’s go there anyone. The DiRECT trial is researching people with type 2 diabetes, and it probably would be good to mention that. I guess that nugget is in the sub-heading, but it might be good to not relegate it there.
But let’s look at that sub-heading. ‘Stay free of symptoms’ is an interesting thing to highlight when we know that in many cases, people with undiagnosed T2D don’t have any symptoms anyway. Surely focusing on what it means in terms of day-to-day life with diabetes (i.e. medication, monitoring requirements, daily burden of ‘doing diabetes’, frequency of HCP visits) would be more meaningful.
Back to the heading and we have the word reverse which is pretty much incorrect in all ways possible. The word they’re looking for is remission. Why? Because even if the result from those in the study is that they don’t require diabetes meds, and their glucose levels are back in range, they still do have diabetes.
I’m not a statistics person. Data hurts my head and numbers make me cry, and I get the complete and utter irony of saying that considering that I live with a condition that depends on me understanding data and numbers, but now is not the time to come at me and my 2.9mmol/l self. Please and thank you.
But there is a number in this research that seems to be jumping out at me and it’s this number: 23%. Let me clarify (this is from the Diabetes UK press release): 23% of participants who were in remission from type 2 diabetes at two years in the original trial remained in remission at five years.
It’s important to also point out that this isn’t 23% of the total people who started in the DiRECT trial five years ago – not all participants were in remission after two years. At two years, 36% remained in remission. Or 53 out of the original 149 research participants in the intervention group (plus a additional 5 people in the control group).
So that 23% is of 58 people who remain in remission now at five years. That’s 13 people. Or about 8% of the starting number. That’s a very different story to what is being presented in news stories, media releases and cross socials today, isn’t it?
And that matters. Big time. Because there is real danger that many people will read the media reports today and in their minds that will mean that remission from type 2 diabetes is a far more likely outcome than reality and is the likely outcome for everyone.
I’m not here to argue whether remission is a thing or not – it is. FOR SOME PEOPLE with type 2 diabetes. Adding pieces to help understanding of the giant puzzle that is diabetes is brilliant for everyone. Research helps us do that. Sharing that research so that people living with diabetes better understand the options available and learn more about how our particular brand of diabetes works is gold!
But I am here to argue that publishing grand sweeping statements about how to ‘reverse’ type 2 diabetes, or telling only part of the story about the research, without the necessary nuance, is inaccurate and will further stigmatise type 2 diabetes and those living with it, especially those who are not able to achieve remission of their condition. The very idea that they could be made to feel that they are not trying hard enough or that they have failed is not being sensationalist.
The stigma associated with type 2 diabetes is considerable and everyone has a responsibility to making it better and not add to it. And surely an even heavier burden of that should fall to those who are working in diabetes. If my 4am, glucose-starved brain is able to grasp how stigmatising something like this could be to people with type 2 diabetes, then it should be glaringly obvious to anyone who has even a passing interest in the condition.
Hey, do you remember a couple of weeks ago when it was International Women’s Day and women got a cupcake (probably baked by a woman) and a breakfast (probably organised by a woman) and then we all agreed that gender equality didn’t need to be spoken about for another year?
Look, I know I sound cynical. But that’s only because I am. Every year at Diabetogenic, I write a post celebrating the incredible women working in diabetes. Mostly I centre diabetes advocates who are generally donating their time – and emotional labour – to power advocacy efforts and make change. And if you look back at the history of the DOC, you will see that the majority of the work has been by women in the community. (Don’t @ me with your ‘But I’m a bloke and I’ve done this’ commentary. It’s not the time for #NotAllMen.)
This year, I started to write something, and then stopped, and started again. And then stopped. Anyone who is a frequent visitor to this site or follows any aspects of my personal advocacy knows that I celebrate the incredible work done by grassroots and community advocates (many/most of whom are women) throughout the year and I didn’t want to buy into the ‘It’s-IWD-here-are-the-womens-now-it’s-back-to-the-misogyny-we-usually-deal-with’ crap that seems to be the aftermath of each and every IWD.
So, I’m using today – this random day – to give a shout out to some of the great things going on that you may have seen, or you may have missed. These things are powered by women who, in most cases, are doing this as extra work on the side of their day jobs, and everything going on in their personal lives. But it’s undeniable that it’s this sort of stuff that is going on all the time, usually flying under the radar, but it’s making a difference to so many folks in the diabetes world.
And so…
There is some remarkable work out of India where the Blue Circle Foundation continues to make a mark in diabetes advocacy. On IWD, a team of women from the Foundation conducted an awareness program for 200 women inmates in Yerwada Jail in Pune, India. This is part of their ongoing Project Gaia which creates safe spaces for women with diabetes. Snehal Nandagawli is just one of the women involved in this work. You can hear more from her at this week’s #dedoc° #docday°.

From the UK, Mel Stephenson-Gray has been a brilliant force in the diabetes community for a number of years. She recently launched a fabulous new Insta page celebrating and empowering women with diabetes. It’s called Diabetes Women’s Health Club and the information she’s been sharing (accompanied by gorgeous graphics) is brilliant. I loved the profiles of some of women who were groundbreaking pioneers in diabetes research. Go give the page a follow now!
Dawn Adams hasn’t managed to convince me that she is only one person because the sheer volume of the work she is doing is immense and she’s bloody everywhere. Dawn continues to blaze trails in her research and writings about diabetes and menopause (follow @MenopauseMither on Twitter for great information and support), has been featured in a number of Diabetes UK publications, spoke at the recent #dedoc° symposium at ATTD, and continues to be a daily support and mentor to people across the global diabetes community. I’ve barely scratched the surface with this list. Someone please send Dawn a coffee and cinnamon bun so she can sit down for 30 seconds and recharge her batteries!
Another woman who is a human powerhouse and obviously works 23 hours a day (lazily, she sleeps for an hour) is Jazz Sethi whose work with the Diabesties Foundation continues to multiply exponentially. She’s also a brilliant speaker and gave an emotional talk at ATTD last month. Check out just some of what she is doing here (and stay tuned for something super exciting that we’ve been working on together!)
Also at the recent ATTD #dedoc° symposium, Hamidah Nabakka from the Sonia Nabeta Foundation captivated the packed-to-capacity room, sharing stories of children and young people living with diabetes in Africa. This was held on the first day of ATTD and for the rest of the week, I had people coming up to me and saying that it was their highlight of the whole conference.
I’m getting to this a little late because it was started last year, but Niki Breslin started a brilliant Insta page to build community called ‘My Type of Family’ for anyone with diabetes who is planning and trying to conceive, pregnant, recently had a baby and parenting. There’s lots of great information and encouragement for the community with this page and definitely worth a follow!

I was so excited to see some artwork by Miss Diabetes from New Zealand make it across the ditch Melbourne in an IWD street art exhibition. Her comic ‘Women and Diabetes’ was on show in our city’s iconic Hosier Lane! Miss Diabetes’ diabetes advocacy is super well-known in the community thanks to her tireless efforts supporting Insulin4All efforts and with work she’s done with the WHO diabetes team. You can see the artwork here.
Anita Sabidi in Indonesia continues to drive and build community with her advocacy work that shine very bright lights on issues such as emotional wellbeing and mental health, and women’s health. Anita is a regular speaker about these important topics, and also leads a number of community initiatives supporting women with diabetes in Indonesia. She’s also speaking at #docday° this week.
Dana Lewis never ceases to amaze. Last week she ran 100kms in a day, but unbelievably, it’s not her physical feats that make her name so well known in the diabetes world. It is, of course, her work in open source AID. Last month she gave two presentations at the Open Diabetes Closing Conference, and she has an upcoming session at the ADA Scientific Sessions in San Diego. On top of that, she continues to publish regularly and is a force for nothing but good!
Ashley Ng from Australia has been documenting life with two gorgeous little girls on her blog, opening up about some of the more difficult aspects of parenting while living with diabetes. I love Ash’s candidness and honesty and am always grateful for her ability to be so raw, but also hopeful. Read and subscribe to her blog here.
These women are just a few of the many who continue to make our community tick and flourish. There work is not only meaningful on 8 March: it’s making a difference every, single day. The very idea that women and their achievements get just one day of real celebration (albeit while battling the calls of ‘where’s International Men’s Day?’) is in equal parts frustrating and insulting. I celebrate the incredible work that women spearhead all the time because I know that alongside that work, they are dealing with patriarchal attitudes that make their successes all the more remarkable. That deserves far more than a cupcake!
Postscript
The UN theme for the day was DigitALL: Innovation and technology for gender equality, not the saccharine sweet ‘EmbraceEquity which means absolutely nothing and was created by some corporate machine that does nothing to advance equality in any way. So, if you spent IWD posting selfies of you hugging yourself, that’s great, but what did that really mean when it comes to advancing gender equality?
If you haven’t had a look at the website from the UN, it’s definitely worth it, even if it’s just to see the high-level details, one of which explains that online gender-based violence silences women and discourages their public participation. It may be odd to think this is a thing in the diabetes community when so much of what you see comes from women, but actually, it’s real. Harassment is a concern for many women, and I know of many women who have stopped sharing or locked down their accounts (permanently or temporarily), or deleted them completely, due to this harassment. I’m one of those women. This is something to be mindful of every day – not just a single day in March.
Four weeks. That’s about how long ago it was that the first murmurings of Fiasp being withdrawn from the PBS were heard in the Australian diabetes community.
It’s been a pretty wild ride in those four weeks, hasn’t it? I never should be surprised at the dedication and never-say-die attitude of diabetes communities, but what we saw from the Australian community was next level! And it went beyond that, with Aussie advocates rallying our friends from overseas (hello #dedoc° Voices!) to amplify our efforts here.
And today, news of a reprieve. Fiasp would be available on the PBS for another 6 months for anyone with a script dated prior to 1 April 2023. (That’s the catch – you need a script before that date, or you will have to pay the private prescription cost.)
This is a great result. It gives everyone with diabetes using Fiasp some breathing space to make plans for what happens if we need to change insulins.
There are a lot of beautiful things about grassroots advocacy. Firstly, it can be incredibly responsive. It takes just one person to share, and the community response is often instantaneous.
We saw that here, didn’t we. As soon as it was just a hint about what was going on with Fiasp, people with diabetes in Australia took to it. This was even before the Minister’s office was aware of what was happening! From a petition (amazing, Belinda!), blog posts and discussions in social media groups, to standing around conference exhibition halls (this is exactly what was going on at ATTD with Aussie advocates!) the momentum started and picked up speed.
It is undeniable that the best results happen when everyone works together, and as I said in my post about this issue a couple of weeks ago, …Community advocacy is often the starting point of rumblings that, combined with strong advocacy from diabetes organisations, leads to policy change.
This is a dazzling example of exactly that! A community of all stakeholders coming together, led by community. Doesn’t THAT make you feel all warm and fuzzy? And today, people with diabetes have celebrated in great ways – the people who should be centred in this win for their efforts. This was my tweet about that earlier today:

Some final thoughts
Celebrate the win and cheer with other community advocates. I’ve loved seeing the commentary in online community groups today! Our celebrations are so meaningful because it is our fridges that were going to be bare of Fiasp if this didn’t come through!!
I know it’s tempting to stockpile, but please don’t! There are 14,000 Australians using Fiasp and hopefully everyone who needs to get a script filled over the next six months will be able to do so effortlessly. Of course there is the human urge to make sure we don’t run out but remember that if you have a year’s supply in the fridge, that might mean someone can’t get their next week’s supply.
This isn’t done yet! Six months is AWESOME but keep the pressure up with the grassroots efforts that worked this time.
I’ve just returned from Berlin, where I attended the ATTD Conference for a week of super busy meetings, information gathering, collaborations and advocacy. At every turn, people with diabetes (many attending after being awarded a #dedoc° voices scholarship) were discussing how community advocacy is key to driving change. I heard about remarkable efforts from people across the globe who are genuinely improving the lives of people with diabetes in their part of the world. And when anyone had a question, or asked for advice, people were only too happy to offer and share.
Right now, if you’re in Australia and live with diabetes, especially type 1 diabetes, you may have heard the kerfuffle about Novo Nordisk’s Fiasp being withdrawn from the PBS after Novo Nordisk made the decision to withdraw Fiasp. The Government can’t compel them to keep it listed.
So what now? Well, now is the time to rally the troops. Already, grassroots advocacy efforts by people in the Australian diabetes community (and friends across the globe thanks to the #dedoc° network) are making a lot of noise. There’s a petition (with over 6,000 signatures) and there have been blog posts. Social media groups are lighting up with comments and questions. This is how a groundswell starts.
You can also get political by reaching out to your local MP. I know that many people think that this is a daunting task, or believe that nothing will come of it. I counter that suggestion by pointing to any significant change in diabetes access in Australia. I’ve been in these trenches for decades now and know the effectiveness of people power. Community advocacy is often the starting point of rumblings that, combined with strong advocacy from diabetes organisations, leads to policy change. I can’t tell you how many letters I wrote back in the early 2000s before insulin pump consumables were on the NDSS. (I thought that the PM and health minister were going to take out restraining orders after I wrote to them both a couple of times each week for three years!) At one point, back in around 2002, I was invited to a meeting with Julia Gillard (in opposition at the time) who asked to speak with a group of diabetes advocates (did we even use that word then?) who had been regularly writing about the cost of pump therapy.
I also think of the incredible community efforts that lead to the Carers’ Allowance being changed back in 2010 so that the parents and carers of children continued to receive payments until their child was 16 years old, rather than being cut off when their child turned ten. Or the numerous letters I wrote, along with thousands of other people, to have CGM added to the Scheme. There have been other issues too – diabetes seems to mean one after another that needs attention.
Right now, the issue is Fiasp and you may be thinking about sending an email, but wondering where to start. Start with your story. Because only you can do that.
You can tell your story and write whatever you feel comfortable – your diabetes may vary and the way you advocate will too. I have some ideas I’m going to share below and I think they are worth considering when you are writing to your local MP. My philosophy is always to keep things short and sweet. I bring the heart with my story and add limited data to win over minds. Hearts and minds remains a central basis to my advocacy ideas. So, if you’re wondering where to start, here are some ideas that may help:
- They don’t know diabetes and don’t know details, so start with the basics and keep it to the point: I am writing about an issue affecting me as a person with diabetes and that issue is the withdrawal of Fiasp from the PBS. Fiasp is the only ultra-rapid insulin available in Australia and there is no comparable and easy swap to be made.
- Be clear about the issue: Fiasp is being withdrawn from the PBS. While it may be available on a private prescription this will make it too expensive for many people with diabetes, meaning a management option is being removed.
- Explain how that impacts you: As a person living with type 1 diabetes, I am required to take insulin every day. Fiasp is the insulin that works best for me and if I am no longer able to afford to use it due to it being removed from the PBS, my diabetes management will be negatively impacted.
- Be clear about your ask: I am asking for you to advise what the Government is doing to address this matter, and how it is working with Novo Nordisk to resolve the concerns of many people with diabetes who are worried we will no longer be able to afford the best treatment option for our diabetes.
Don’t ever believe that you are not going to be part of the movement that makes change. Just a minute in the Australian diabetes community right now is enough to see how a movement has already started. It’s organised and collaborative and the noise is already beyond a rumble. And you can add your voice.
Disclosure
I have worked in diabetes organisation for the last twenty-one years. Recently I joined the Global Advocacy Team at JDRF International as Director of Community Engagement and Communications and until earlier this year I was Head of Community and International Affairs at Diabetes Australia. My words on this blog are always my own and independent of my work and the organisations where I am working. My individual local and global advocacy efforts are in addition to my ‘day job’. I am also Global Head of Advocacy for ##dedoc°°.
Like clockwork, the beginning of February heralded a sea of red in every retail store, with cutesy cupid motives and love hearts adorning shop windows. Valentine’s Day was the next big merchandising opportunity and, friends, it’s time to buy up.
At the same time, the diabetes community also starts to be sprinkled with red – this time red roses. Because once again, it’s time for Spare a Rose, Save a Life. It’s the complete opposite of consumer culture. And it’s something that is very close to my heart.
This year marks ten years since Spare a Rose was first launched by a group of diabetes advocates from the US. The story has been told many times but it’s worth repeating, because it says a lot about this community. These advocates wanted to do something that supported others living with diabetes, specifically those in under-resourced counties. And so, Spare a Rose, Save a Child (now Spare a Rose, Save a Life) was created, with a vision to bring together the diabetes community, uniting in the collaborative goal of supporting those who need it.
The simple equation of ‘sparing’ one rose and donating the $5 saving to a diabetes charity was tangible. That face dollars provides insulin for a month. That’s how it has worked for ten years now. Close to one million dollars has been raised in that time, which is truly remarkable when you think about it. It’s people in the community reaching into our pockets to help make a change.
This year, donations are once again going directly to Insulin for Life, a charity that continues to support people with diabetes in countries where there is most need. Insulin for Life has been running for many years and their work is significant. Last year, as war broke out in Ukraine, the charity was able to rally their networks within days, getting critical diabetes supplies where they were most needed. That support continues, and a big part of that is due to the generosity of the diabetes community getting behind Spare a Rose for Ukraine.
As soon as the war started, the diabetes community were desperately looking at how to help and almost immediately, people dug deep. With $400,000 raised in months, so many in the community showed just how committed we are to focusing on others. That’s the diabetes community I know and love!
And so, this year – the tenth anniversary of Spare a Rose – we’re asking again for people to dig deep and help if they can. Leave egos at the door and do the simple thing of supporting community efforts by sharing links, encouraging others to learn about Spare a Rose and, where possible, donate. The only people who benefit from this campaign are people with diabetes who need it. By the community, for the community. Truly the best way to celebrate Valentine’s Day.
Here’s your Spare a Rose, Save a Life refresher for how it works. It’s super easy, and if you click on the image, it will take you directly to the donation page. (Donations are made directly to Insulin for Life.)

Postscript and disclaimer
I have been a community volunteer for the Spare a Rose campaign for a number of years, involved in promotion and communications. I’ve taken a step back this year (for a bucketload of reasons, including this), but am no less involved behind the scenes. I have just started a new job and much of the focus is supporting people with diabetes in low to middle income countries which means I’ll be supporting efforts of many different diabetes charities, including Insulin for Life and Life for a Child (previous charity partner of Spare a Rose), A4D, CDIC and others, as well as the brilliant community groups lead by advocates on the ground.
Manhattan’s East 41st Street is Library Way. Patience and Fortitude, the grand lions that stand guard outside the New York Public Library gaze down the street, keeping an eye on people hurrying by, and those who stop to admire the beautiful and imposing building.
Library Way is paved with bronze plaques engraved with literary quotes. I’ve walked the street between 5th and Park avenues a number of times, just to read the inscriptions.
The other day, as I hurried home to our apartment, this plaque caught my eye:
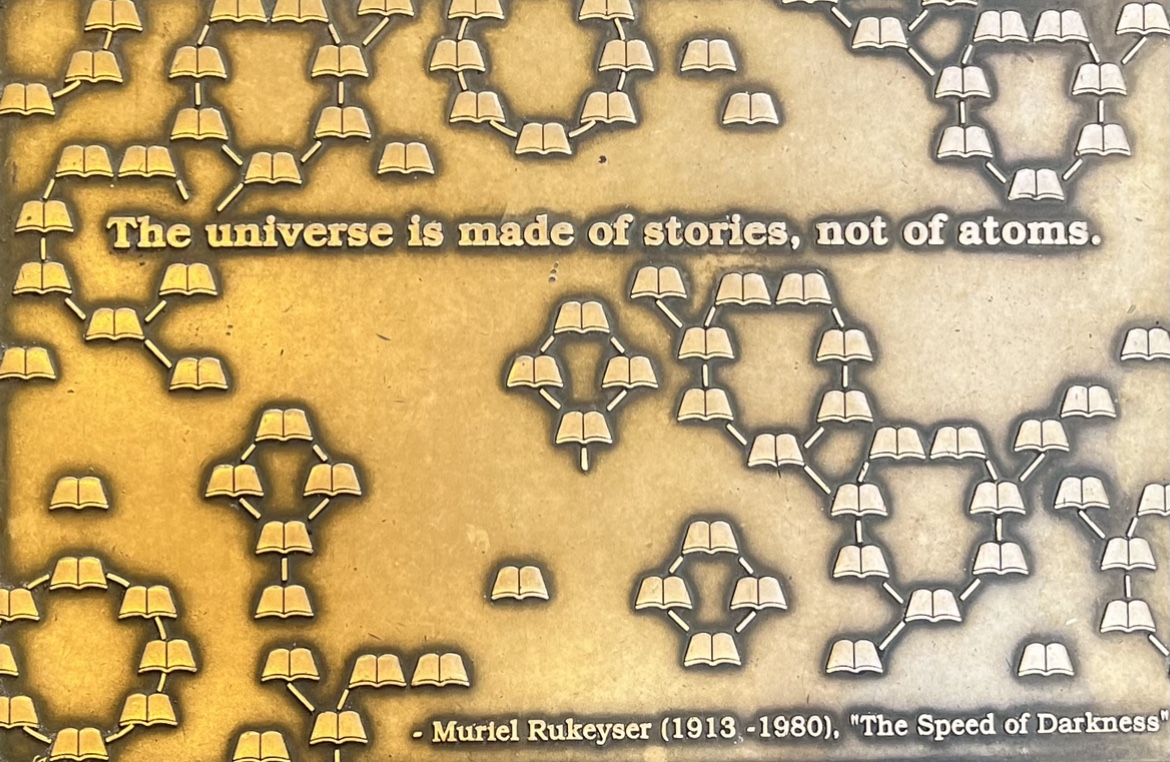
I stopped, made sure I wasn’t blocking any one’s way (lest I attract the wrath of Fran Lebowitz who is living rent free in my mind after I watched ‘Pretend it’s a City’), and I snapped a quick photo with my phone.
‘Isn’t that true,’ I muttered under my breath as I picked up speed and walked at the only pace I’ve come to accept in this gorgeous city – ultra fast.
This blog has always been about stories. Mostly mine, sometimes mine intersected with others. My advocacy life is about sharing stories and encouraging others to understand the power and value of those stories. It’s stories we connect with because we connect with the people behind them.
My time in New York is wrapping up and I’ll be back in Melbourne soon. I’ll be home, starting a new job and I’m so excited. And part of the reason for that excitement is that I will still be working with people with diabetes and their stories.
In the world of advocacy – in my advocacy life – lived experience is everything. I can’t wait to hear more stories, meet more people and learn more. And keep centring lived experience stories. Because, after all, that’s what the universe – and the diabetes world – is truly made of. Just like the plaque says.
It’s World Mental Health Day and that seems as a good as any a day to speak about diabetes and mental health. Actually, every day is a good day for that, but with every health organisation’s social media manager’s attention turned to today’s health promotion day, I’m jumping on that bandwagon and adding this post to the myriad on Diabetogenic that address the very significant issue of diabetes and mental health.
I don’t think it’s fair to say that we don’t speak about diabetes and mental health these days. We do. As is so often the case, the conversations started in the community, led by people with diabetes and then were slowly, but surely picked up by other stakeholders. Many health professionals are tuned into mental healthcare being part of diabetes care. And in recent years, diabetes organisations have followed the lead of the community by running public health campaigns aimed at raising awareness of diabetes and mental health. Thanks to peer-reviewed research, we have evidence to show that diabetes impacts mental health and that mental health impacts diabetes.
But even if we say confidently say that diabetes mental health is on the agenda, there is still good reason to believe that more light be shed on the topic, and more attention be given to it. And to really advocate for mental health care to be seen as part and parcel of diabetes care. I really do believe that would make a huge difference.
When we talk mental health in diabetes, there’s a lot to consider. Of course, there are the diabetes-specific things like diabetes burnout and diabetes distress. Plus, eating disorders can take on a particularly diabetes-focus with conditions such as diabulimia (which really, really needs to be listed in the Diagnostic and Statistical Manual of Mental Disorders – it’s such a difficult, under-researched, misunderstood, yet very present reality for so many people living with diabetes).
But there are also ‘every day’ mental health conditions that are increased when someone lives with diabetes, such as depression and anxiety. Just how much of that is linked to diabetes?
And for those of us who dabble in the advocacy world, there is advocacy-related burnout to contend with too and that can and does start to impact our own diabetes management and mental health.
I couldn’t even try to estimate the number of times I’ve given talks about diabetes and mental health from a lived experience perspective. But I am always happy to be asked, and always willing to talk about it, even if it means being quite vulnerable and exposed when I do so.
I remember when my work in diabetes organisations started to focus more on mental health, and I also remember when those discussions were accompanied by a change in narrative. Suddenly, a lot of what we spoke about – from diabetes-related complications to risk reduction – came with a side serve of mental health commentary. It helped to show the undeniable link between the two. And the community responded to that favourably.
Diabetes has never just been about glucose levels, or carbohydrates. And there are healthcare professionals and researchers and organisation leaders that understand that – probably because they have spent time really listening to people with diabetes, rather than just churning out the old tropes about the ticking time bomb of diabetes. Actually, those tropes have probably contributed to a lot of diabetes-related distress.
Starting conversations about diabetes and mental health can be difficult. I like to think that all HCPs these days are aware of the intersection between diabetes care and mental health care, but sadly, I don’t think that is necessarily the case. If the stories I frequently see on social media are anything to go by, there is still a way to go when it comes to having frank, open, honest discussions that recognise that the mental health of people with diabetes needs attention.
These days, I know that my mental health is really not that great. While I know that may seem alarming, I actually see it as progress. Being able to identify that I am feeling this way means I can do something about it. In years gone by, I had no awareness about my mental state. I didn’t know what to do about it.
When I talk about how my mental health is faring – especially when feeling as I do now – there is often surprise. I am not backwards in coming forwards and I know that many people see me as confident, assertive, and self-assured. And I am that way. I’m also pretty bubbly and positive about life in general. But with it comes some dark times and dark thoughts and dark days that are really not especially easy to manage.
I don’t know about others, but when things are dark, everything seems bigger and scarier. I had a low the other night that hit below 2.0mmol/l, and ordinarily I’d deal with it and move on. But during the hypo and since then I’ve not been able to stop thinking about it and worrying about it. It never pays to play ‘what if’ in diabetes, and yet most of my thoughts when remembering the other night have started that way. The constant crap that I’ve been dealing with in the advocacy space for far too long now feels unbearable, and seems so, so nasty that I feel a wave of anxiety just being online. The burden of simply doing diabetes feels massive. The other day, I cried when my insulin pump demanded a battery change. And I can’t shake this overwhelming feeling that I have no idea what I am doing with my own diabetes management and am so anxious about complications, even though there is no good reason for it. These are the dark feelings. The reason sleep gets disturbed. The reason that my heart beats faster.
If I could wave a wand and make one thing come true this World Mental Health Day, it would be that everyone with diabetes has access to mental health care as part of routine diabetes care. And if I could wave that wand for a second time, I’d want my own mental health to build back up and become a little more robust than it is right now. That would be really, really great.