
You are currently browsing the category archive for the ‘Diabetes’ category.
There are moments when someone says something so illuminating that it sticks with me and I turn their words over and over and each time, those words hit home deeper and deeper.
That’s how I’ve been since last week, when Victor Montori, during his talk at the Nossal Institute for Global Health’s Compassion, Care, Complexity & Culture webinar said: ‘The work of being a patient is invisible‘. He went on to talk about just some of what is required of people living with health conditions. Of course, Victor is spot on! There is nothing simple about needing to navigate complex health settings and systems, yet most of our work to make it all make sense is not seen or recognised.
As soon as he said it, I realised that those of us with diabetes are hit with a double whammy. Not only is the work we do invisible, but so is our health condition. We don’t ‘look sick’. There is often very little to point to our diabetes and how it can challenge, frustrate, exhaust us. I frequently talk about what it takes to ‘do diabetes’ – the arduous, momentous, all encompassing tasks that it relentlessly demands of us. But how many people actually see that? Diabetes isn’t alone here; there are certainly other invisible conditions.
We need to exist and function within health systems that sometimes feel as thought they are working against us and as health becomes more and more corporatised, our frustrations grow. Perhaps it’s just me, but with every mission statement and strategic plan that promises to do better by people (with diabetes or whatever), all I seem to see is less recognition of what real life for us is like. My consulting side hustle often has me being asked to review these documents, and the question I ask most is ‘And what does this mean exactly for the people you are meant to be serving? How exactly are you going to reduce the burden?’ (or whatever it is that they have promised to do). In most cases they can’t answer and furthermore, there is a genuine lack of understanding of what that burden is.
Is making the work of being a ‘patient’ more visible to more people what is required to systems to change? I know that in the case of diabetes, it is those health professionals who recognise what we do to make our invisible condition tick are the ones who are often more generous in their dealings with us. My endocrinologist has frequently acknowledged just how much there is to do with diabetes, how hard it is, and understands that no one really wants to have to do it. She’s right. On all counts. But I wonder how she knows that when so many others simply don’t.
We regularly hear about how overworked healthcare professionals are and how our under-resourced health systems are working to capacity and I don’t for a moment doubt any of that. But you know who else is working to capacity? Those of us living with health conditions. But for us, looking after our health is a burden on top of ‘every day life’. It’s a job on top of our jobs. It’s just that we do it all hidden from plain sight.
The only way that the work we do will become visible is if we talk about it, and work to quantify it. Justin Walker’s comment at the DData event back in 2018 went some way to doing that when he said ‘By wearing OpenAPS, I save myself about an hour a day not doing diabetes‘. I can’t tell you the number of times I have quoted this because it shows two things: firstly, just how effective Open Source AID (and perhaps commercial systems too) can be at reducing the burden of diabetes tasks, and secondly, to highlight how much time those tasks take. Getting back an hour of my day, each day, has been brilliant. But there are still minutes lost every day to diabetes. And what we do during those minutes is largely unseen. It’s the invisible work Victor spoke of.
The invisible work extends to the hoops we need to jump through simply to exist. I hear from friends in the US the hours and hours of work they need to do to sort through health insurance issues. This week, I’ve spent hours upon hours of my time trying to navigate VicRoads (the state’s licensing authority) and the decision that, despite no changes to my diabetes, additional medical reports were necessary for me to keep my license. The final outcome was the sensible one – no need for anything further, after all – but it took emails, several phone calls where I was required to explain and explain and explain again, text messages to my endocrinologist, and my own inside-out knowledge of the guidelines before the right outcomes was reached.
I feel that as health system frequent flyers, we have simply come to expect that this is part and parcel of the process and I so appreciated Victor highlight the work, and suggest that the burden that has fallen to us should be remembered. I have thought about it a number of times since the event: after waiting for 45 minutes to see a nurse for a vaccine last week, only to be told the vaccine wasn’t in stock and I’d need to source it (even though I asked if it was available); as I raced between two different pharmacies to collect said vaccine after the one I called first didn’t have it available, despite them promising me they did just ten minutes earlier when I called, while listening to hold music as I waited for 15 minutes so I could speak with someone to reschedule a screening check that had been cancelled for no apparent reason, as I rearranged a meeting so that I could get to the local pathology centre for a fasting blood check (after being sent away the previous afternoon because I wasn’t aware that I needed to fast for that particular check). And while speaking to the third medical reviewer at VicRoads yesterday.
I don’t know anyone who wants to do the invisible work of being ‘a patient’. And yet, I feel that we all know that there isn’t a choice. We accept that the toils of managing diabetes persist, silently and profoundly hidden in the shadows. And feel locked into a contract that expects us to do hours and hours of work apparent to no one. Invisible, perhaps. But real? Absolutely.

Diabetes stigma is a hot button topic in the diabetes world. It has been for some time. I wrote just last month how stigma was one of the most talked about issues at ADA. That week, we also launched an Open Letter from the Diabetes Community, asking health professionals to join us in our call to stop diabetes stigma.
And behind the scenes, for all of this year, another exciting, BIG, project has been hatching and I’m so excited to share it today.
Earlier this year, in an unprecedented show of unity and determination, a group of 51 experts from 18 countries joined forces to pool our lived, research and clinical experience to address diabetes stigma and discrimination. Together, we’ve reviewed the scientific evidence and established an international consensus on 49 Statements of Evidence and Recommendations. The full report on this review has been submitted and is currently under review.
Excitingly, the group also reached a consensus on a Pledge dedicated to bringing an end to diabetes stigma and discrimination. And that’s where you come in! Everyone can sign to show your commitment stop the ingrained negative judgments, stereotypes, and prejudices that influence attitudes about diabetes, and contribute to the stigma so many of us face. This isn’t just for the community. We know there is sometimes an echo chamber as we say the same things to each other, over and over. We also know that while diabetes stigma is indeed prevalent within our community, we also need to tell the story of its harm outside the diabetes world.
Well, here’s an easy way to do both. Please sign the pledge and share details across your social platforms. You can sign as an individual, and we’d also love for you to see if your place of work, school, community group, hospital, church, sporting team, favourite cafe…basically anywhere that is likely to come into contact with people with diabetes (i.e. literally everyone!) would be interested in signing too.
This is a true community effort, with involvement from stakeholders from across the diabetes landscape, across the world. You won’t see logos anywhere, because this for and about all people with diabetes. The names of the people involved in the work so far is on the website.
Are you with us?

A few weeks ago, I saw a post on LinkedIn from Nick Dawson. Nick was around Twitter health communities a lot when I first joined and it was great to read his post and take a wander down Twitter’s memory lane.
The feeling of nostalgia was strong. I don’t remember joining Twitter, but I do remember when I started actually using it to connect with others with diabetes from around the globe and how my diabetes world suddenly seemed infinitely bigger. No longer was I constrained to only people in my own networks, or even my own country. I was a global citizen in the diabetes online world. And it felt great.
Twitter became the cornerstone of a lot of my own advocacy and connections online. I never missed a weekly #DSMA tweet chat, expertly moderated by Cherise Shockley. The rapid fire hour of diabetes power often included hundreds of people. Dana Lewis’ #HCSM weekly chats brought together from different health communities, opening my eyes not only to different healthcare struggles, but also to solutions that helped me with my own diabetes. I used Twitter to find people who were doing incredible things that elevated the voice of people with diabetes. It was on Twitter that I followed along with the first Roche blogger summit that brought together US social media pioneers. I used those sorts of events to shape the Australian Social Media Summit that was held at the end of 2012, coordinated by Diabetes Victoria, bringing together Australian diabetes social media folk and Kerri Sparling from the US.
I was part of the team that started the weekly #OzDOC tweet chats in July 2012, working with Cherise to help get things started close to home. Around the same time, the first #GBGoc tweet chat happened and the first #dedoc° chat, #FRDoc and #ItDOC followed soon after. Back then, those chats were brilliant at highlighting local issues, but by and large, they were indeed global.
Twitter was the tool I used to take notes at conferences, live tweeting sessions to share with those not in the room, and then pulling the information together in briefing documents at works, and writing articles here and on other platforms. And Twitter was the channel where remarkable whole community events happened. Remember Kelly Kunik’s #IWishPeopleKnewThatDiabetes and those #DayOfDiabetes discussions? Or the groundbreaking and overwhelming community event that was #Simonpalooza? It was peer support on demand. There was no need to feel alone with your diabetes if you were on Twitter!
And then, I don’t know when, Twitter changed. Or I changed. Or the community changed. It became harder to find the people who had shone so brightly and made Twitter a place of support and community. I stuck close to old friends who never advertised the Twitter following count, because who cared? I learnt the difference between an advocate and an influencer. And I started to steer completely clear of parts of the community which was so alien to what it had been like when I first joined. #DSMA chats became less frequent because Twitter chats became kind of old hat. #OzDOC chats completely stopped because there hadn’t been a sustainability plan in place and there really wasn’t anyone to take over. Perhaps this was a reflection of how the community wanted to engage and what they…what we…wanted.
For me, most of the day-to-day reaching out I used Twitter for moved to being via private channels. And that worked fine and became the same lifeline that the public space Twitter had once been.
There have absolutely been some bangers recently that have made me remember how great Twitter can be. The weekly #DiabetesChat, using Spaces, launched a new community that, although based in the UK, was very much global. Tom and the organisers went out of their way to include people from other places around the world to be interviewed and lead discussions. I loved it straight away for the beautiful open and welcome feeling that was there and embraced it. #dedoc° isn’t really a Twitter based organisation, but the #dedoc° voices use it brilliantly, and diabetes conference are so visible because of their prolific sharing.
In the last few days, a new Twitter-like app called Threads has been launched and I tentatively signed up and had a nosy look around. It felt like Twitter in 2012. Friendly. Fun. Open. I’ve found Threads friends (thriends?) who I’ve not seen around the Twitter traps for years and have re-engaged. I’ve managed to steer clear from the parts of diabetes Twitter that I’ve actively avoided over recent years.
It’s not perfect. There needs to be an option for people to add ALT text to photos, because that’s not there yet. Apparently it is coming. (But, you know, accessibility should have been a first level consideration, not an after thought…) A desktop version would be useful – it’s annoying only having the option to type on a phone keypad. The lack of hashtags is annoying. (Just today, I went back and read the tweets from that first Australian social media summit by searching the hashtag. What a treasure trove!) Again, this is said to be on the cards. As is the capability to see only threads from people you’re following rather than the mishmash right now. Having said that, sprinkled in amongst the predominantly diabetes focused threads I’ve been seeing, I’m not too disappointed with the cat pics, recipes and book recommendations that I’m seeing a lot of. Also pleasing is that I’ve managed to avoid so much as a hint of the crappy, manipulative, misogynist side of the diabetes world that clouded my Twitter experience for a while before I worked out how to block it out completely.
Is this the future of Twitter? Over here on this new app? Threads feels like the nostalgia Nick wrote about. It really does feel like the ghost of Twitter past and I like it a whole lot more than the ghouls of Twitter present. Come and visit if you’re not there already. I’m @RenzaS and you’ll see me sharing diabetes stuff, pet photos, books. And asking people about their diabetes experiences to help me make sense of my own. I hope to see you there!

All too frequently, when talking about meaningful lived experience engagement, I hear about ‘Hard to Reach Communities’. A number of years ago, I called rubbish on that, putting a stop to any discussion that used the term as a get out of jail free card to excuse lack of diversity in lived experience perspectives.
‘People with type 2 diabetes don’t want to be case studies’ or ‘Young people with diabetes don’t respond to our call outs for surveys’ or ‘People from culturally and linguistically diverse communities won’t share their stories’ or ‘Folks in rural areas don’t come to our events’. These are just some real life examples I heard when asking why there was no diversity in the stories I was seeing.
See how the blame there is all on the people with diabetes? They don’t want, don’t respond, won’t share, won’t attends. It’s them. They’re the problem. It’s them.
I stood on stage at EASD in Stockholm last year and challenged the audience to stop using the term ‘hard to reach’. Because that’s not the case at all. The truth is that in most cases, the same old, uninventive methods are always employed. And those methods only work for a very narrow segment of the community.
I recently heard someone begrudge that all applicants who responded to a recent call out for a new committee were the same: white, had type 1 diabetes, city-dwelling. ‘Of course they are,’ I said. ‘That’s the group that loves a community advisory council and responds to an expression of interest call out on socials. They are able to attend meetings when they are scheduled, are confident to speak up and are willing to share their story, because they probably have before and received positive feedback for doing so Plus, they’re expecting everyone else at the table will look and sound just like them.’
But the lack of diversity isn’t the problem of the people who didn’t respond. It’s the problem of whoever is putting out a call and expecting people to reply because that’s how it’s Always Been Done.
This was a discussion at a meeting during last week’s American Diabetes Association Scientific Sessions. The #dedoc° voices were meeting with the ADA’s Chief Scientific Officer, Dr Bob Gabbay, and Vice President in Science & Health Care, Dr Nicole Johnson. The question about how to reach a broad audience was asked. At #dedoc°, efforts have been made to attract a diverse group of people to our scholarship program, and have, to a degree there as been some success. A glance at any one of the #docday° events, or scholarship alumni will see people who had not previously been given a platform within the diabetes community. But there is always more than can be done.
The discussion in that meeting at ADA mirrored many that happened throughout the week. And it’s not surprising that US diabetes advocate Chelcie Rice came up with the perfect way to explain how to do better at engaging with the who have previously been dismissed as ‘hard to reach’. He said: ‘You can’t just put pie in the middle of the table. Deliver the pie to where they are.’ And he’s right. Those tried and true methods that work for only one narrow segment of the community have been all about putting pie in the middle of the table, knowing that there will be some people ready with a plate and a fork. But a lot of people are not already at the table, or comfortable holding out their plate. Or maybe they don’t even like that pie. But we never find out because no effort is really made.
Chelcie once said ‘If you’re not given a seat at the table, bring your own chair‘ and I’ve repeated that quote dozens, if not hundreds of times. And his words ring very true for people like me who have felt very comfortable dragging my own chair, and one for someone else and insisting that others scramble to make room for us. But that metaphorical table isn’t enough anymore. Not everyone wants to sit at a table and we need to stop expecting that. Instead, it’s time to find people where they are – the places, the settings, the environments they feel comfortable and at home. That’s how you do engagement.

On day 2 of the American Diabetes Association Scientific Sessions, rushing between meetings, I overhead another attendee say this: ‘I’ve never heard so many people talking about diabetes stigma’. I turned to them, a bright smile on my face and said, ‘I know, right?’, (a phrase I only ever utter when I’m in the US).
Just a few hours earlier, Jazz Sethi and I had tweeted simultaneously, setting free an open letter from the diabetes community about diabetes-related stigma. You may have seen it; thousands of people have. And others have shared, commented and even translated it into different languages (I think we’re at 6 translations and counting). Here it is!



When we first asked advocates from the community if they would like to add their logo to the letter we were surprised by the quick response. Almost everyone we went to said yes. We hadn’t gone out too widely – we wanted to test the waters first. The first version of the open letter includes advocates and peer support groups from across the world. Amazing!
And after our very low-key, (i.e. a couple of tweets from unverified Twitter accounts, so who knows what the algorithm did with them!), we were once again inundated by people asking for us to add their logos. (We haven’t managed to add them yet, but absolutely will in coming weeks. Please give us time if you’ve shared your logo. We’ll get there. And I’ll update this post with the new final page when that happens.)
There is something magic about these sorts of very grassroots, very community, very inclusive initiatives. Not only are they great because they collaboratively offer a narrative from people with diabetes, highlighting an issue that is of great importance to many. They also show you just how powerful and united our community is while also pointing to individuals and groups who are keen to work together, support each other and power the importance of lived experience. And that’s pretty special!
Imagine a community where people come together to make things happen. You don’t have to look far, really. Just look at the diabetes community!
Here’s something new from some folks (Jazz Sethi, me and Partha Kar) who are desperately trying to reshape the way diabetes is spoken about, and how fortunate I feel to have been involved in this project!

The thinking behind these particular language resources is to truly centre the person with diabetes when thinking about communication about the condition. In this series, we’ve highlighted three groups where we know (because these are the discussions we see in the diabetes community) language can sometimes be stigmatising and judgemental. This isn’t a finger-pointing exercise. Rather it’s an opportunity to highlight how to make sure that the words, images, body language – all communication – doesn’t impact negatively on people with diabetes.
A massive thanks to Jazz and Partha. Working together, and with the community, to create and get these out there has been a joy. (As was sneaking into the ATTD Exhibition Hall before opening time so we could get a coffee and find a comfortable seat to work before the crowds made their way in!) And a super extra special nod to Jazz who pulled together the design and made our words look so bright pretty! And a super, super, super special thanks to Jazz for designing my new logo which is getting its first run on the back of these guides.
You can access these and share directly from the Language Matters Diabetes website. These don’t belong to anyone other than the diabetes community, so please reach out if you would like to provide any commentary or be involved in future efforts. There’s always more to do!

On Sunday, one of those annoying diabetes things happened – a kinked insulin pump cannula, subsequent high glucose levels followed by a little glucose wrangling tango where, instead of rage blousing, I tried to gently guide my numbers back in-range. I thought about how frustrating diabetes can be – unfairly throwing curve balls at us even when we are doing ‘all the right things’. And so, I used this little story for a post on LinkedIn to illustrate why I am so dedicated to making sure that stories like this are heard and lived experience is centred in all diabetes conversations.
Meanwhile, anyone who has even the barest of little toes dipped in the water of the diabetes community would have heard about Alexander Zverev being told by French Open officials that he was not permitted to take his insulin on court. He was expected to inject off court and, according to Zverev, was told ‘looks weird when I [inject] on court’. Insulin breaks would be considered as toilet breaks.
What’s the connection between this story and my LinkedIn story? Absolutely none. Except there kind of is.
I’m not about to write about sports or try to connect my story with that of a top-ranking tennis player. That would be totally out of my lane. (The couple of years of tennis I took when I was in grades five and six give me no insight into life of a tennis player.)
However, when it comes to discussing diabetes and the stigma surrounding it, I’m definitely in my lane. I understand and am very well-versed when it comes to talking about the image problem diabetes faces and how that fuels the stigma fire.
The response from the diabetes community when the Zverev story broke. Most people were incredibly supportive of the tennis player and rightfully indignant of the incident. JDRF UK responded swiftly with an open letter to the French Open organisers, eloquently highlighting why their ruling needed to be changed. And changed it was.
My LinkedIn post was shared a few times and there were comments from people saying that these stories help others better understand our daily challenges and work to cut through a lot of the misconceptions about diabetes.
And then there was this direct message:
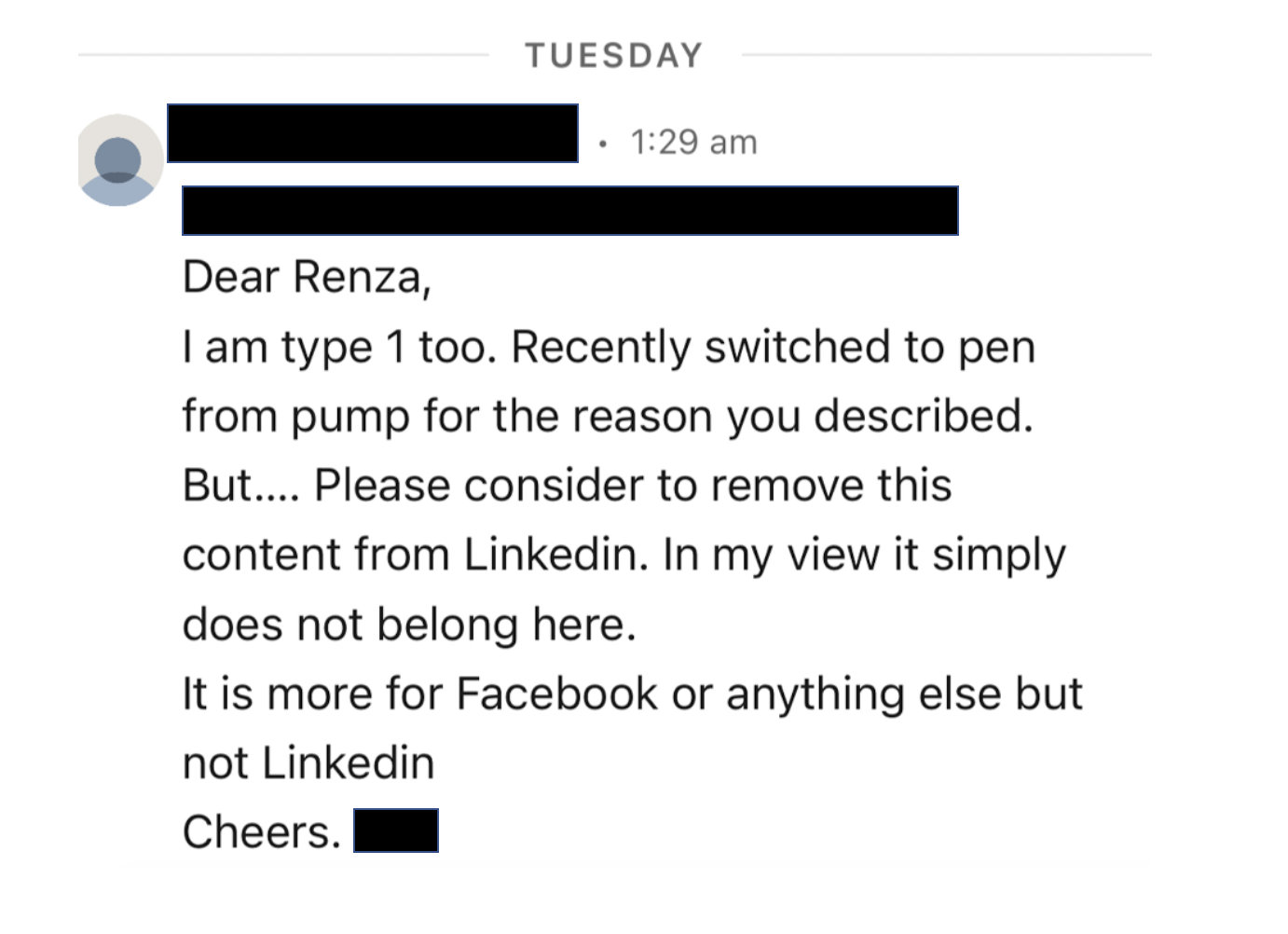
I bristled as I read it. My initial response was ‘How dare this man try to tell me what I can and can’t post on LinkedIn. Who is he to tell me what I can and can’t share?’ I snapped a reply back to him where I pointed out: ‘…I am a diabetes advocate, working to change attitudes and raise awareness about living with diabetes. My post belongs here on LinkedIn as it very much aligns with the work I do.’
But I haven’t been able to stop thinking about it because as problematic as it is for someone trying to silence what people with diabetes share online, there was more that was troubling me.
The idea that diabetes is a topic only appropriate in certain contexts and should be hidden away from others reinforces shame. Suggesting work settings are not the place to talk diabetes plants that seed that diabetes, and people with diabetes, could be liabilities in the workplace. Talking about diabetes on LinkedIn – a platform for business and workplace networking – is relevant because people with diabetes exist in business and workplaces, and the reality is that diabetes sometimes interferes with our work. Which is perfectly okay. Last week, I needed to refill my pump during a meeting. So, I let others on the call know what I was doing and carried on. On another day, I was recording a short video about a research program and after take 224 realised I needed to treat a hypo and did so. I shouldn’t need to feel that these aspects of daily life with diabetes are only allowed to happen out of view.
Essentially, this is what Alexander Zverev was being asked to do at his workplace: hide away when he needed to perform a task that keeps him alive, as if there is something shameful and disgusting about it. In my mind, this top ranked tennis player playing in a Grand Slam competition should be commended. I mean, any tennis player who does that is remarkable. Zverev does it and then goes about performing the duties of a pancreas. His opponents don’t have to do that! Their pancreas doses out the perfect amount of insulin without any help. Talk about an unfair advantage!
Not everyone wants to talk diabetes with others and that’s fine. But those of us who are happy to speak about and ‘do diabetes’ wherever we are shouldn’t feel that we are doing anything wrong. Diabetes stigma exists because there are so many wrong attitudes about diabetes. It’s insidious and it’s damaging. It erects barriers creating a climate of shame and perpetuates misconceptions that lead to ignorance. And it pressures us to hide away the realities of diabetes, as if there is something to be ashamed of. But there is nothing shameful about living with diabetes. There is nothing shameful about injecting insulin on Centre Court at Roland-Garros, or sharing frustrations on LinkedIn. Or anywhere else. Diabetes has a place wherever your workplace might be. Stigma, however, does not.

I live right near one of the busiest streets in inner Melbourne and Fridays are extra busy. This morning, I was walking quickly to grab a coffee, a mental checklist working through my mind of the things I needed to get done for work for the day.
I was stopped at a light, waiting for green so I could cross. ‘Meeting in 45 mins to discuss the next project; review proposal that was sent this morning; reply to email about Melbourne Uni presentation; send bio and headshot for program for conference in August; amend flights for San Diego trip, call…. Wait. Am I low?’
The unmistakable urgent low alarm of my Dex snapped me out of my to-do list, and I pulled my phone from my pocket. My Dex line was straight, my number in range. I shook my head thinking I must have dreamed the blaring alarm. As I was shoving my phone away, I saw a woman next to me rummaging through their bag. The next second, she crouched down and turned its contents onto the footpath.
‘Hey,’ I said quietly, knelt down so I was level with her. I handed over an unopened packet of Mentos. She looked at me, surprised. I smiled. And said, ‘I’ve done that very thing more times than I care to remember.’ I passed her a small purse and a couple of pieces of paper that escaped from the dumped bag debris. She thanked me and we stood up together. ‘Are you all okay?’ I asked. She nodded. ‘Yep, I’m okay. Thanks.’
The light changed and I set off, giving a little wave. ‘Wait,’ she called after me, breaking the Mentos packet in two and handing half to me. ‘Take this in case you need it?’ I shook my head. ‘You hold onto them; I’m nearly home. Hope the rest of your morning is hypo-free.’
I picked up my pace and turned down a paved laneway, and into a café. As I waited for my coffee, I thought about how that brief encounter was a snapshot of the invisible community of people with an invisible condition. Until, of course, it’s not. Community isn’t always apparent. It doesn’t have to be the coming together for face-to-face meetings, or long Twitter exchanges. Sometimes, it simply lies within fleeting moments of strength and vulnerability and solidarity that provide solace and remind us that there are others out there who truly get it.

My husband is a secondary school music teacher and it’s been fascinating hearing educators’ thoughts on using artificial intelligence (AI) tools in the classroom. I’ve generally heard two schools of thought about AI, such as ChatGPT. Some teachers identify how useful it can be and are excited about the myriad ways it can enhance education and support students’ learning in new and innovative ways; others see it as pure evil, signalling the end of education as we know it and will be exploited by pesky students. Thankfully, my husband is very firmly in the first group!
My daughter is a freshly minted university student, and of course, AI is front and centre of university faculty minds, with students receiving warnings about misusing the technology, and how assessors would be on the lookout for any assignments turned in that appear more ChatGPT and less CramGPT-AllNight. But again, it’s interested to hear about how some of her lecturers and tutors are using the technology to develop novel and engaging ways to learn. And students are finding ways to use AI tools to assess the work they are doing and pinpoint shortcomings to allow them to go back in and work on specific areas that might need attention.
But where are we in diabetes? What are we thinking about how AI could be useful in diabetes education and support? The ADA’s Diabetes Care journal weighed into the issue with this article published recently. The article provided a generally balanced view of what AI could do when it comes to providing diabetes education.
Some of the pitfalls noted include: inaccuracy in the information provided, (and limited updates on new evidence and developments) and the potential for presenting false information convincingly, leading to safety concerns due to factual inaccuracies. There is often a lack of nuance in differentiating insulin types and variation in blood glucose units. Obviously, it has a reliance on a general information database, not specific medical knowledge. There was also a comment about there being inconsideration for the needs and wishes of individuals (but then, I’m pretty sure some HCPs I’ve had to deal with could be accused of the same thing). The reliance at the end of almost every response to ‘consult your healthcare team’ is a helpful if people have access to such a team but could be problematic for those who don’t. The downsides it listed were fair, although I suspect most could be easily overcome.
And the advantages that were highlighted were also spot on, and included: increased access to information, and the provision of systematic, concise, well-organised responses, with clarity around any jargon used. The ability to augment basic levels of education and offer more detail if requested by the user means that people with diabetes can customise their education to suit their level of understanding, needs and interests and regional and cultural contexts, rather than be at the mercy of generic education models and information that is often all that is offered. Of course the fact that education can be on-demand – when and where people with diabetes want it – is hugely convenient! These certainly are all valuable and could address many of the frustrations experienced by people with diabetes when it comes to seeking and receiving diabetes education.
But there was one glaring omission in the advantages list. ChatGPT comes with neutrality and with that neutrality comes a lack of prejudice about diabetes and people with diabetes. It doesn’t judge and it doesn’t blame the person with diabetes either. At no time is ChatGPT going to accuse the person seeking education that they are lying about their glucose levels (yes, that happened to me), or imply they are in denial about their diabetes (yes, so did that), or suggest the person is simply not trying hard enough (yes, and that) or isn’t caring about their health (yep – on more than one occasion). AI bots in diabetes care, and health more widely, can be seen to create a supportive space where people can seek guidance without feeling self-conscious.
The fact that there is no emotion in an AI bot means that they come without the baggage of preconceived ideas and previous experience. And they come without human interaction, and yes, I realise that this is in direct contradiction with my frequent calls for HCPs to be more human and person-centred.
Before any diabetes educators come at me for trying to do them out of a job, please know that’s absolutely not what this post is about. Rather, I’m trying to highlight what it is that AI offers that could overcome some of the barriers (and those barriers can be mighty, mighty difficult to overcome!) that are experienced by people with diabetes when it comes to diabetes education.
I don’t think it needs to be said that this is a conversation that is going to be had more and more. AI isn’t in the scary future of diabetes education; it’s here and now, and smart CDEs will be the ones who work out how it can be used to enhance their work and be added as an additional tool to support people with diabetes. In fact, I would be looking for health professionals who are actively embracing this sort of tech rather than expressing scepticism about it.
Because here’s the thing: AI is going to put more control and power into the hands of people with diabetes. It’s already doing that and it’s only going to increase as AI models get smarter and can learn and adapt to each user, faster and more accurately. And this is going to mean less reliance on HCPs for aspects of diabetes care. But this is a great thing, in exactly the same way that diabetes tech such as home glucose monitoring, insulin pumps. CGM and automated insulin delivery have delivered similar outcomes.
The way diabetes care is evolving is at a crossroads. Better diabetes-specific technology, better drugs, ever-growing peer-led innovation, learning and support, all augmented by AI. The potential to create opportunities to better support people with diabetes and enhance our care is huge. I’m not for a moment suggesting that AI is a substitute for human interaction, but it undoubtedly has benefits over traditional healthcare approaches and offers new dimensions of support, in ways that can be customised and more relevant for people with diabetes. And if, at the foundation of all this, is the opportunity to remove stigma and help people with diabetes feel less blamed and shamed for their condition, that is a massive win!
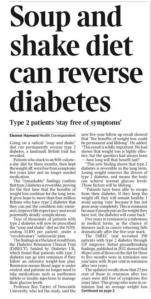
I woke up (at 4am thanks to a hypo, but that’s another story all together) and scrolled through a variety of social media feeds and, because I seem to follow a lot of diabetes-related pages and people, was bombarded with the below. And so, these are my very early morning musings, a stream of consciousness mess, the logic and rationality of which is most likely influenced by low blood sugar. (The typos, however, are all mine.)
So, let me begin by saying that this is important work – of course it is. The DiRECT trial has really put the idea of diabetes remission on the research agenda, encouraging further research into the issue, provided another potential diabetes treatment option for people with type 2 diabetes, and supporting people with type 2 diabetes looking at this way of managing their diabetes. Choice. It’s a good thing!
Today we have some follow up data (after the initial two years of the trial), providing updates on how research participants are going. Again. It’s important research, and it is helping increase knowledge and understanding of type 2 diabetes. Good stuff!
But one of the things I am all about is accuracy in reporting and this, my friends, isn’t it.
I wasn’t going to even touch the heading of the article, because surely the inaccuracy of it doesn’t need highlighting at all, but let’s go there anyone. The DiRECT trial is researching people with type 2 diabetes, and it probably would be good to mention that. I guess that nugget is in the sub-heading, but it might be good to not relegate it there.
But let’s look at that sub-heading. ‘Stay free of symptoms’ is an interesting thing to highlight when we know that in many cases, people with undiagnosed T2D don’t have any symptoms anyway. Surely focusing on what it means in terms of day-to-day life with diabetes (i.e. medication, monitoring requirements, daily burden of ‘doing diabetes’, frequency of HCP visits) would be more meaningful.
Back to the heading and we have the word reverse which is pretty much incorrect in all ways possible. The word they’re looking for is remission. Why? Because even if the result from those in the study is that they don’t require diabetes meds, and their glucose levels are back in range, they still do have diabetes.
I’m not a statistics person. Data hurts my head and numbers make me cry, and I get the complete and utter irony of saying that considering that I live with a condition that depends on me understanding data and numbers, but now is not the time to come at me and my 2.9mmol/l self. Please and thank you.
But there is a number in this research that seems to be jumping out at me and it’s this number: 23%. Let me clarify (this is from the Diabetes UK press release): 23% of participants who were in remission from type 2 diabetes at two years in the original trial remained in remission at five years.
It’s important to also point out that this isn’t 23% of the total people who started in the DiRECT trial five years ago – not all participants were in remission after two years. At two years, 36% remained in remission. Or 53 out of the original 149 research participants in the intervention group (plus a additional 5 people in the control group).
So that 23% is of 58 people who remain in remission now at five years. That’s 13 people. Or about 8% of the starting number. That’s a very different story to what is being presented in news stories, media releases and cross socials today, isn’t it?
And that matters. Big time. Because there is real danger that many people will read the media reports today and in their minds that will mean that remission from type 2 diabetes is a far more likely outcome than reality and is the likely outcome for everyone.
I’m not here to argue whether remission is a thing or not – it is. FOR SOME PEOPLE with type 2 diabetes. Adding pieces to help understanding of the giant puzzle that is diabetes is brilliant for everyone. Research helps us do that. Sharing that research so that people living with diabetes better understand the options available and learn more about how our particular brand of diabetes works is gold!
But I am here to argue that publishing grand sweeping statements about how to ‘reverse’ type 2 diabetes, or telling only part of the story about the research, without the necessary nuance, is inaccurate and will further stigmatise type 2 diabetes and those living with it, especially those who are not able to achieve remission of their condition. The very idea that they could be made to feel that they are not trying hard enough or that they have failed is not being sensationalist.
The stigma associated with type 2 diabetes is considerable and everyone has a responsibility to making it better and not add to it. And surely an even heavier burden of that should fall to those who are working in diabetes. If my 4am, glucose-starved brain is able to grasp how stigmatising something like this could be to people with type 2 diabetes, then it should be glaringly obvious to anyone who has even a passing interest in the condition.






